Medicare Will Spend More Than $13 Billion on the Medicare Advantage Quality Bonus Program in 2026
The Medicare Advantage quality bonus program, established by the Affordable Care Act, increases Medicare payments to Medicare Advantage plans that qualify by having a star rating of 4 or above (on a five-star rating system). (See the KFF brief on Medicare Advantage payments for more detail.) Plans may, but are not required to, use the increase in payments to cover the cost of supplemental benefits, including reduced cost sharing, extra benefits not covered by traditional Medicare (e.g., vision, hearing and dental), lowering Part B premiums, and/or subsidizing Part D prescription drug coverage. The star ratings are intended to help consumers make informed decisions when choosing among Medicare Advantage plans and the potential for additional funding is intended to encourage plans to improve quality. However, the Medicare Payment Advisory Commission (MedPAC) and others have suggested that the star ratings incorporate too many measures, do not adequately account for social risk factors, and may not be a useful indicator of quality because star ratings are reported at the contract rather than the plan level. Medicare Advantage contracts typically include multiple plans, which may have different benefits, costs, networks, service areas, and enroll different populations (i.e., plans that are open for general enrollment and special needs plans that limit enrollment to dual-eligible individuals).
Critiques of the quality bonus program have led to calls to replace, reform or end the program. In 2018, the Congressional Budget Office estimated that eliminating the quality bonus program would lower federal spending by almost $100 billion over ten years. Given the sharp increase in both actual and projected Medicare Advantage enrollment since CBO’s analysis, the savings from eliminating the quality bonus program could be substantially higher. For example, 35 million people are enrolled in Medicare Advantage in 2026, which is 5 million more than CBO projected at the time of the analysis. The degree to which changes to the quality bonus program would impact plan quality or the availability of supplemental benefits would depend on the specifics of any proposal and how insurers modified plan offerings in response.
Recently, the Centers for Medicare & Medicaid Services (CMS) finalized changes to the star ratings system (effective for 2029 star ratings, based on the 2027 plan year performance) that include removing several administrative measures and others that CMS stated no longer meaningfully differentiate plan quality. Though this change is a step toward simplifying the quality measurement system, because it is not combined with other changes to the Medicare Advantage payment system, the change is projected to increase Medicare Advantage spending by $18.6 billion over the next 10 years. That increase in spending is in part because more Medicare Advantage plans are expected to qualify for a payment increase under the quality bonus program as a result of the changes.
This analysis examines trends in Medicare spending resulting from the quality bonus program, enrollment in plans in bonus status (plans that qualify for a benchmark increase based on their quality star rating), and how these measures vary across plan types and insurers using publicly available information on Medicare Advantage enrollment, payment rates, and quality ratings (see methods).
Key Takeaways:
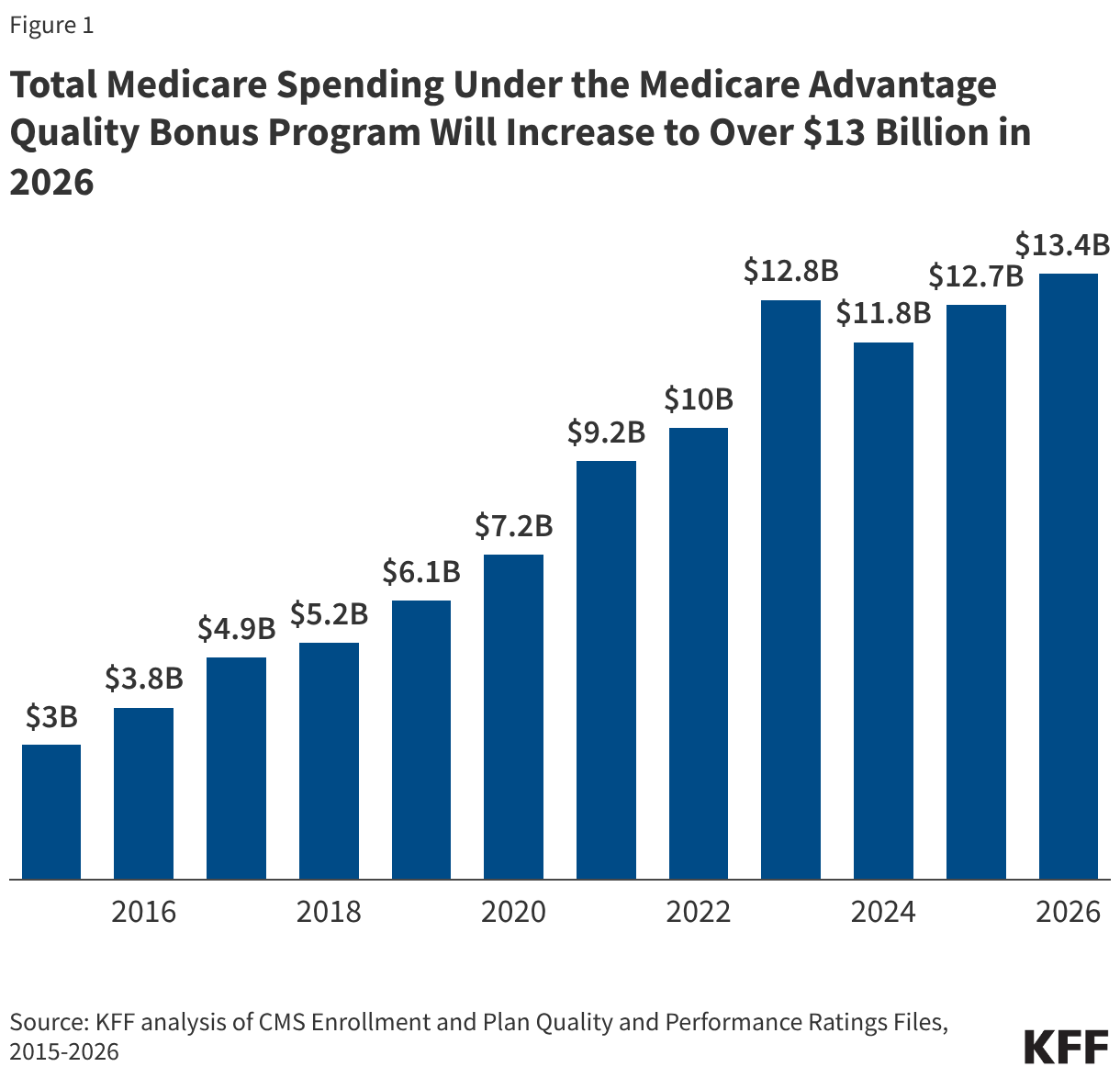
- Federal spending related to the Medicare Advantage quality bonus program will reach at least $13.4 billion in 2026, somewhat more than in 2025 ($12.7 billion), and more than four times higher than in 2015.
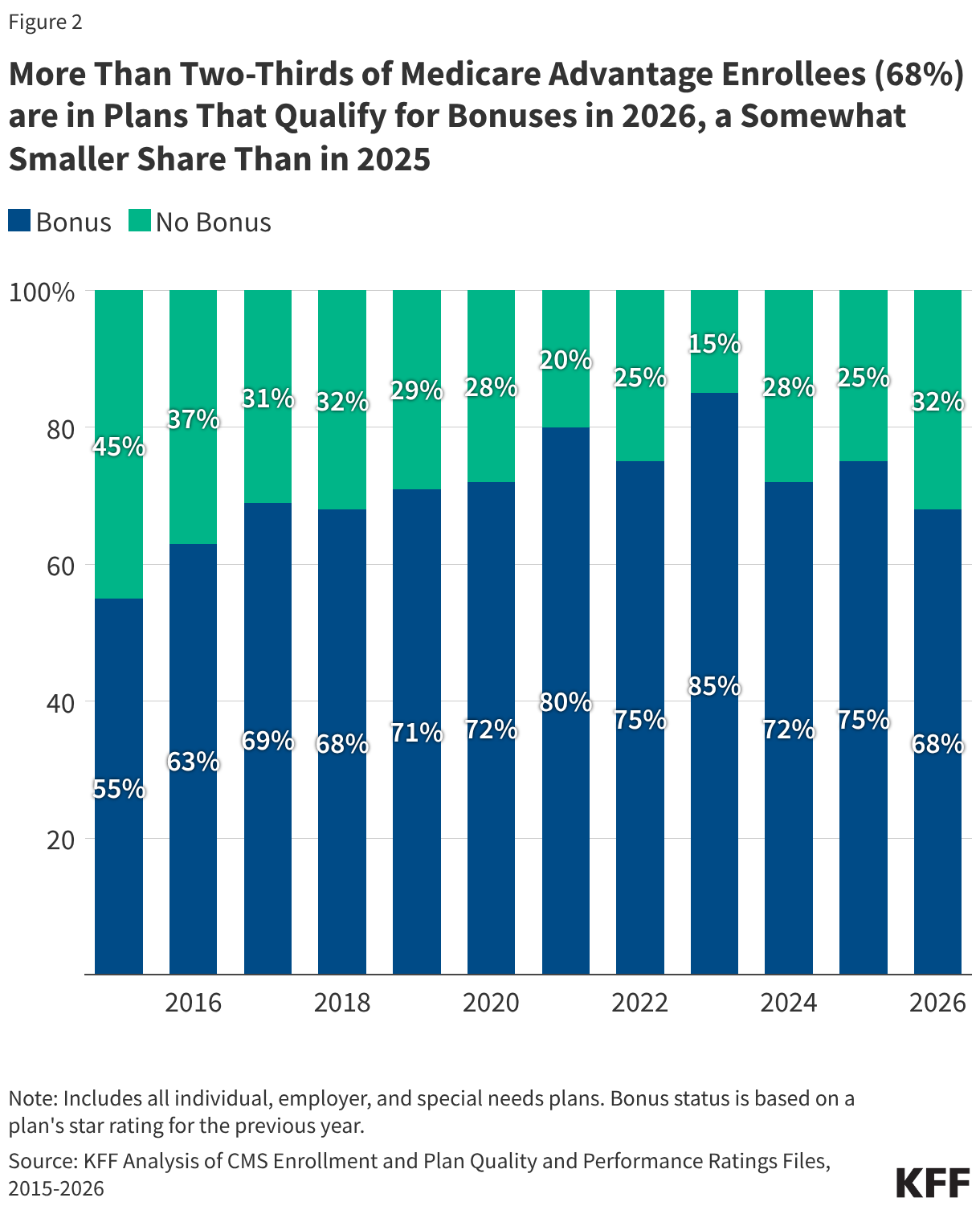
- More than two-thirds of Medicare Advantage enrollees (68%) are in plans that qualify for the quality bonus program in 2026, a decline from 75% in 2025, and the lowest share since 2018.
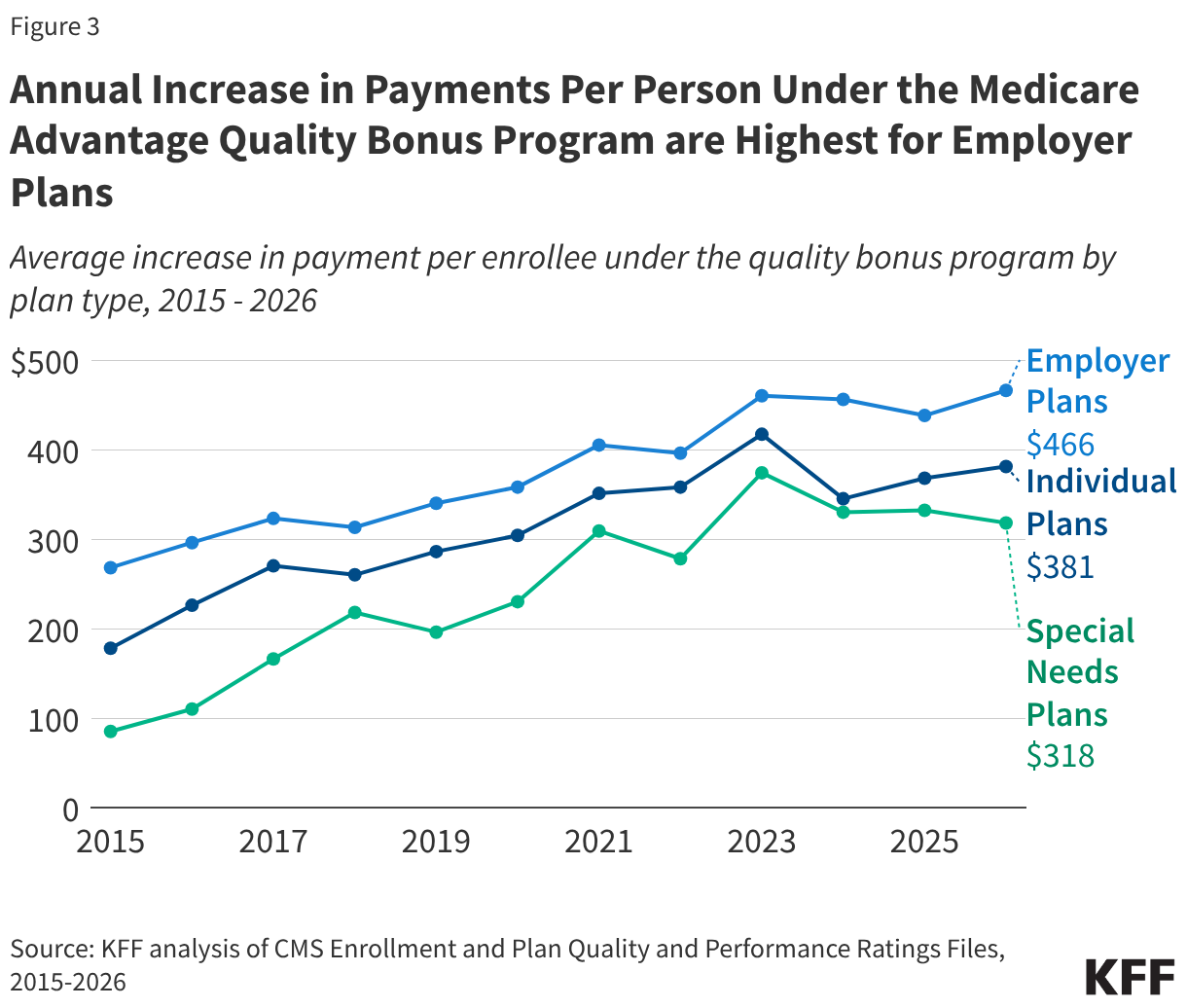
- The average increase in payment per enrollee because of the quality bonus program is highest for employer- and union-sponsored Medicare Advantage plans ($466) and lowest for special needs plans ($318).
- Medicare spending under the quality bonus program varies across firms with UnitedHealth Group receiving the largest increase in payments ($3.9 billion) because of the quality bonus program (relative to what payments would have been otherwise) and Kaiser Foundation Health Plans receiving the largest increase in payments per person ($577). The variation is largely due to the share of enrollees in plans that qualify for increases under the quality bonus program but also relates to the average star ratings of plans that qualify.
Medicare will spend more than $13 billion on the Medicare Advantage quality bonus program in 2026.
Estimated federal spending on the Medicare Advantage quality bonus program will total at least $13.4 billion in 2026, somewhat more than 2025 ($12.7 billion). Spending on the quality bonus program has increased sharply since the program started, more than quadrupling from $3.0 billion in 2015 to $13.4 billion in 2026 (Figure 1). Total spending on the quality bonus program is 2.3% of the projected payments to Medicare Advantage plans in 2026 ($574 billion).
These estimates are a lower bound because they assume that, on average, Medicare beneficiaries enrolled in each plan that qualifies for additional payments under the quality bonus program are of average health status as measured by their risk score (that is, having a risk score equal to 1). However, increased coding intensity in Medicare Advantage suggests the risk scores are likely higher, which would increase the additional payments. For example, MedPAC estimates the increase to risk-adjusted benchmarks under the quality bonus program will add about $16 billion in Medicare spending in 2026. The estimates also do not include additional Medicare spending that results if plans increase their bids when their benchmark is higher because of being in bonus status (See Box 1 for more detail on star ratings and Medicare Advantage payments). For example, a plan might increase its bid to increase payments to providers, add more expensive providers to its network, or retain a larger amount as profit, provided they meet medical loss ratio requirements. (The medical loss ratio is the share of premium revenues going to pay for claims versus administrative overhead and profit.)
Medicare spending under the quality bonus program has grown faster than enrollment in Medicare Advantage, which has doubled since 2015. This spending comes at a time when the Medicare program is facing growing fiscal pressures. Medicare Advantage benchmarks (and corresponding spending) grew faster than traditional Medicare spending between 2017 and 2024 in part because of the increase in spending under the quality bonus program. The quality bonus program also exacerbates the impact of higher coding intensity and favorable selection in Medicare Advantage, which together add $76 billion to Medicare spending in 2026. (Note, the higher spending under the quality bonus program is not additive to the $76 billion.)
More than two-thirds of Medicare Advantage enrollees (68%) are in plans that qualify for the quality bonus program.
In 2026, nearly 24 million people, or 68% of Medicare Advantage enrollees, are in plans that qualify for higher payments under the quality bonus program. That compares to just under 9 million people (55%) in 2015 (Figure 2). Both the number and share of enrollees in plans that receive bonuses in 2026 declined from the previous year (26 million or 75% of Medicare Advantage enrollees) and is the lowest share since 2018. That is a result of changes to the cut points, or scores plans are required to achieve to get higher quality ratings, values that CMS recalculates every year. In particular, substantially fewer Medicare Advantage contracts achieved at least a 4-star rating in 2026 compared to the previous year (209 vs 261). Star ratings are based on a Medicare Advantage contract’s performance on about 40 different measures, such as the share of enrollees that receive certain cancer screenings and annual flu vaccinations, whether people with chronic conditions are getting recommended services, enrollees’ ratings of their health plan, and customer service. For each measure, CMS establishes “cut points”, which are used to assign a rating between one and five stars for that measure. These are then combined into an overall rating for the Medicare Advantage contract.
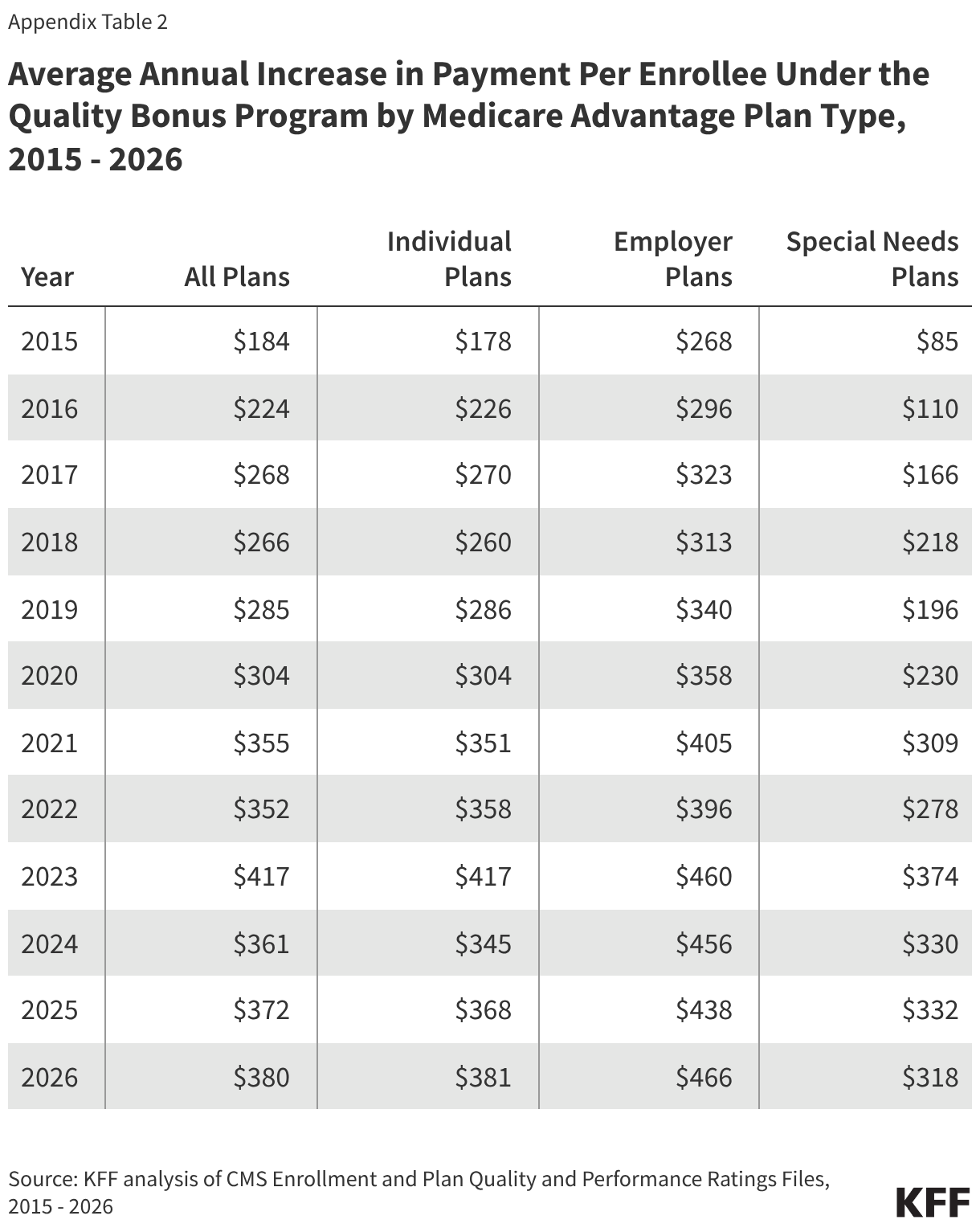
The average annual increase in payments per person under the quality bonus program are highest for employer- and union-sponsored plans.
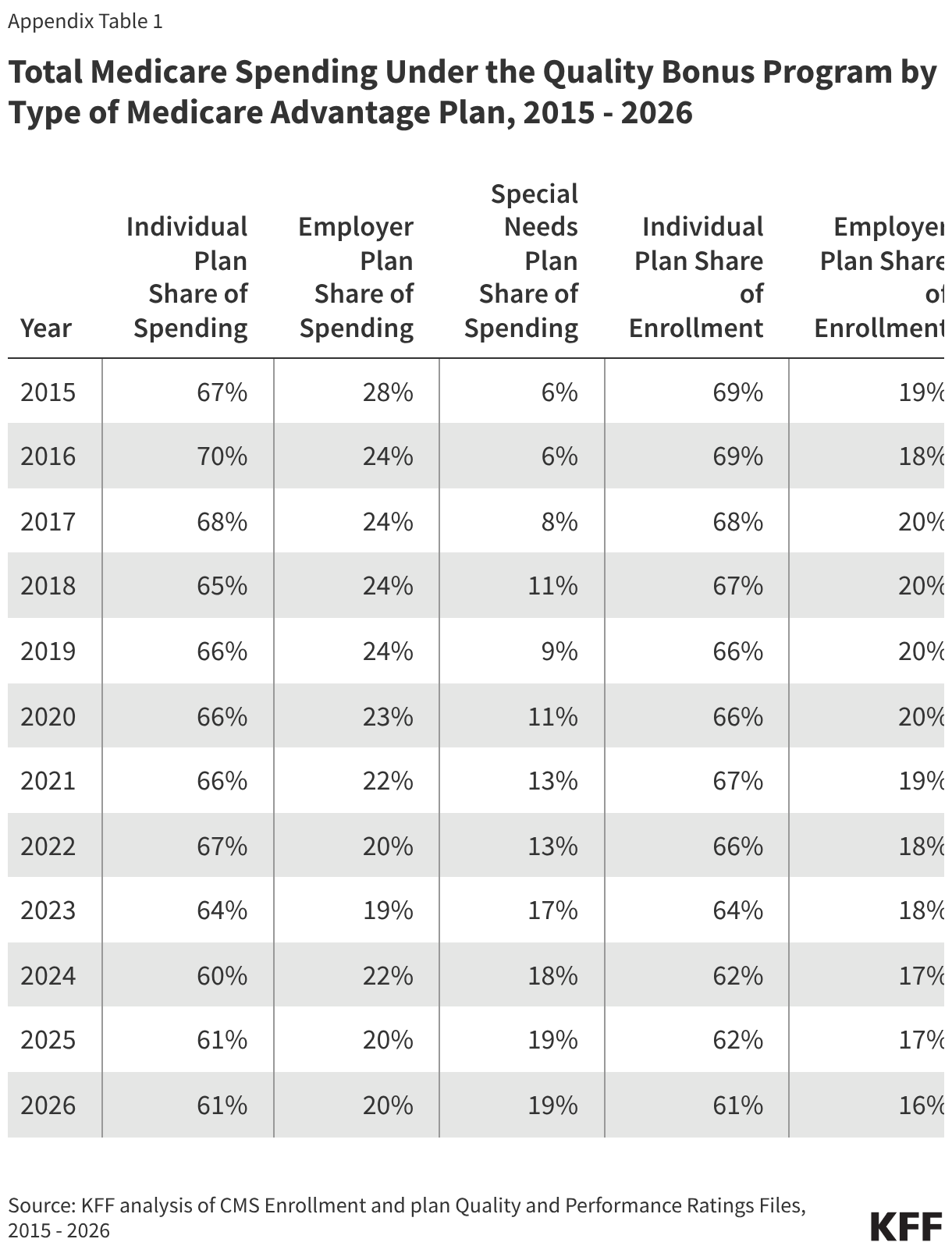
Employer- and union- sponsored Medicare Advantage plans account for a larger share of spending under the quality bonus program (20%, or $2.6 billion) than enrollment in Medicare Advantage (16%) (Appendix Table 1). Consistent with this, and similar to previous years, the average increase in payments per person as a result of the quality bonus program to group employer- and union-sponsored plans ($466) are higher than for individual ($381) or special needs plans ($318) (Figure 3).
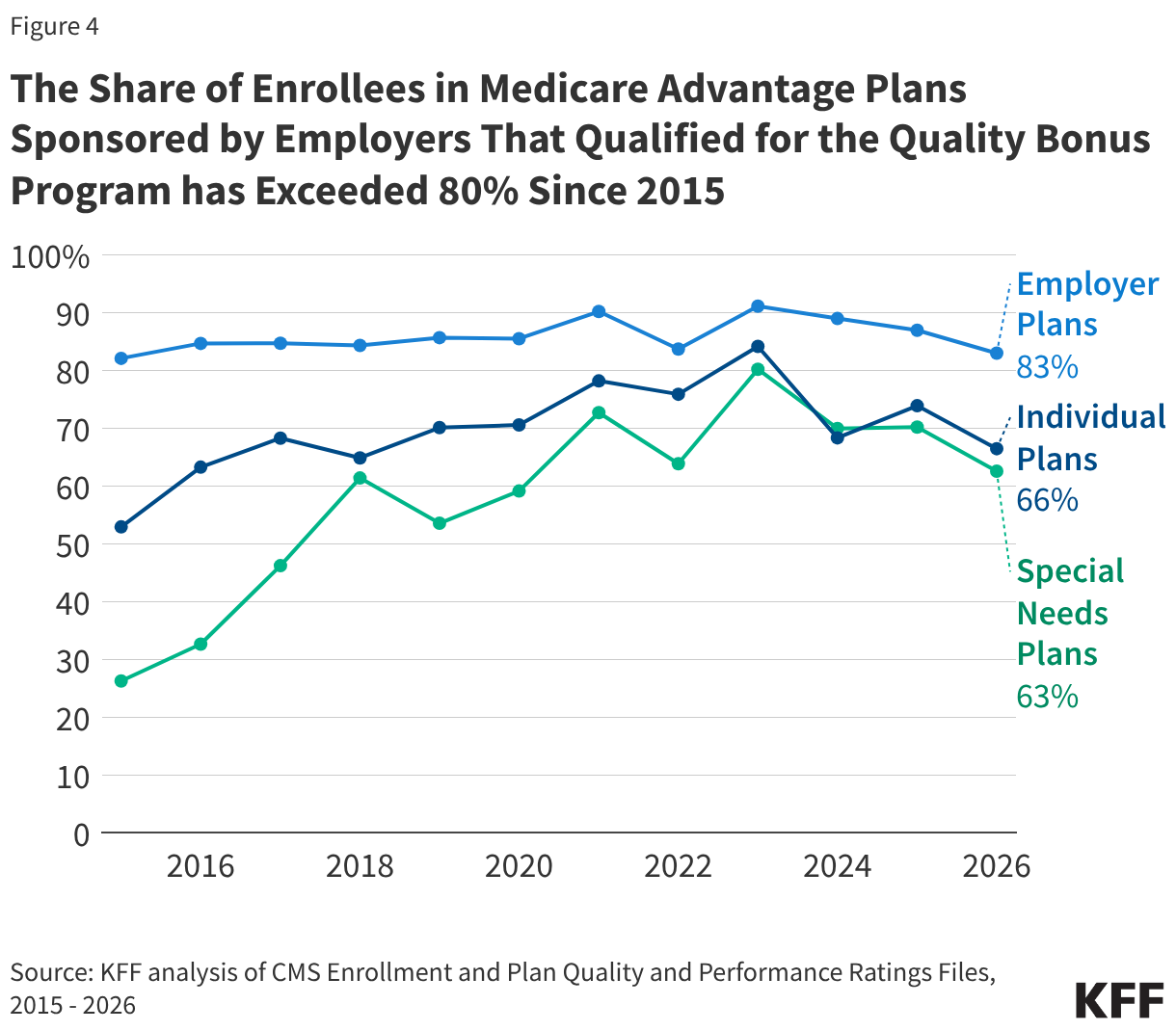
The increase in payments per enrollee stemming from the quality bonus program are higher for employer- and union-sponsored plans because these plans have higher average star ratings, resulting in a larger share of enrollees receiving coverage from plans that qualify for bonuses. Across the entire period of 2015 to 2026, the share of all enrollees in employer- or union-sponsored plans that qualified for the quality bonus program never dropped below 80%. In contrast, the share of enrollees in individual and special needs plans that qualified for the quality bonus program exceeded 80% in only one year – 2023 (Figure 4).
Special needs plans serve higher need beneficiaries, including people who are dually eligible for Medicare and Medicaid and people who require an institutional level of care. Despite critiques of the quality star rating system, lower star ratings for special needs plans, on average, raise questions about how well these plans are serving the needs of their enrollees. The higher share of employer- and union-sponsored plans that qualify for the quality bonus program also raises questions about whether these plans, which are restricted to retirees of specific employers or unions, include more generous coverage or extra benefits. However, gaps in Medicare Advantage data, including the lack of information about the costs and benefits of employer- and union-sponsored plans, mean it is difficult to examine these questions.
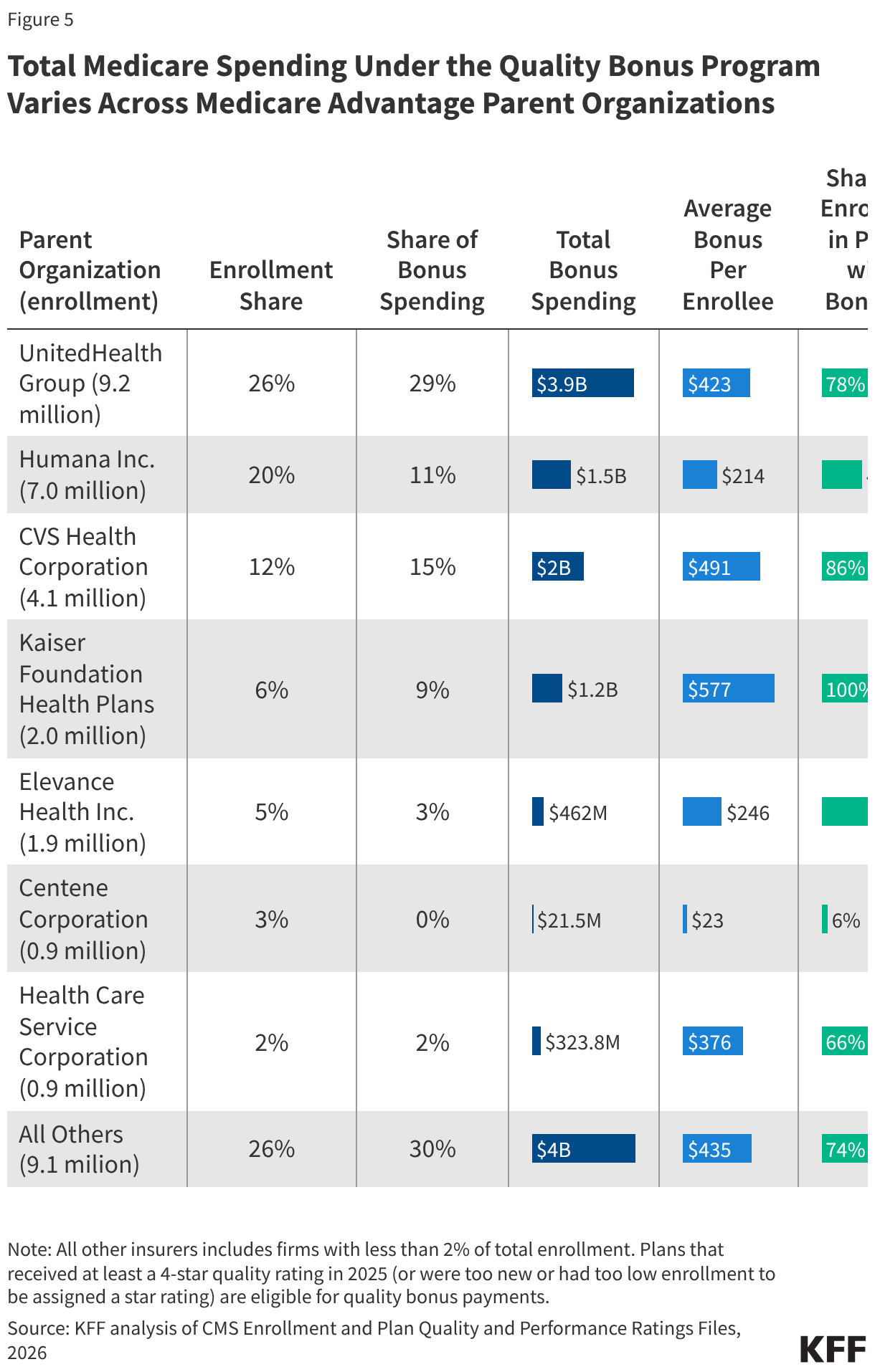
Total Medicare spending under the quality bonus program varies across Medicare Advantage parent organizations.
UnitedHealth Group enrolls just over one-quarter (26%) of Medicare Advantage enrollees and is expected to receive 29% of total Medicare spending under the quality bonus program, or $3.9 billion dollars in 2026 (Figure 5). Humana Inc., which has the second largest share of Medicare Advantage enrollment (20%), will receive a disproportionately smaller share of bonus spending (11%), or $1.5 billion in 2026. Humana’s average star rating dropped considerably for the 2025 plan year (which is the year used for 2026 bonus eligibility), after the star rating for one of its largest contracts dropped from 4.5 to 3.5. Humana sued CMS over the change, but to date, the courts have sided with the Administration. In recent years, Medicare Advantage insurers have increasingly challenged the star ratings calculations, and have prevailed in a handful of cases, prompting CMS to recalculate the ratings on occasion. For example, in response to a decision following a legal challenge from Clover Health, CMS announced it will recalculate the 2026 star ratings for all plans (which will affect the 2027 payment year), though only plans that see an increase in star ratings as a result of the recalculation will have their ratings changed.
The average increase in payments per enrollee under the quality bonus program ranges from $23 for people in Centene Corporation plans to $577 for those in plans sponsored by Kaiser Foundation Health Plans. The variation in total bonus spending across firms corresponds to differences in the share of enrollees in plans that are eligible for the quality bonus program, which is based on the ratings of those plans. Virtually all of the more than 2 million enrollees in a plans sponsored by Kaiser Foundation Health Plans (100%) are in a plan that receives increased payments under the quality bonus program because it has a quality rating of at least four stars, while just 6% of Centene’s 938,000 Medicare Advantage enrollees are in a plan that receives bonus payments in 2026. The only Centene sponsored Medicare Advantage contracts that qualify for the quality bonus program payments in 2026 are those that are too new or have too low enrollment to receive star ratings. Differences also reflect variation in the star ratings of plans that qualify for the quality bonus program, because plans with at least 4.5 stars get a larger increase.
Box 1. Medicare Advantage Star Ratings
A key feature of the quality bonus program is the star rating system. Star ratings are used to determine two parts of a Medicare Advantage plan’s payment: (1) whether the plan is eligible for a bonus, and (2) the portion of the difference between the benchmark and the plan’s bid that is paid to the plan. The benchmark is the maximum amount the federal government will pay for a Medicare Advantage enrollee and is a percentage of estimated spending in traditional Medicare in the same county, ranging from 95 percent in high-cost counties to 115 percent in low-cost counties. The bid is the plan’s estimated cost for providing services covered under Medicare Parts A and B.
Since 2015, plans that receive at least four (out of five) stars have their benchmark increased. For most plans in bonus status, the benchmark is increased by five percentage points. Plans in “double bonus” counties – defined as urban counties with low traditional Medicare spending and historically high Medicare Advantage enrollment—have their benchmark increased by 10 percentage points. In addition, the benchmarks for plans without ratings due to low enrollment or being too new are increased by 3.5 percentage points. The benchmarks are capped and cannot be higher than they would have been prior to the ACA. This can result in plans that are eligible under the quality bonus program receiving a smaller increase to their benchmark, or in some cases, no increase at all.
The benchmark increases under the quality bonus program for qualifying plans mean that per enrollee payments are higher than if the plan did not qualify. There is no separate bonus payment. Rather, the bid and/or rebate components of the payment are higher.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Appendix
Methods
This analysis uses data from the Centers for Medicare & Medicaid Services (CMS) Medicare Advantage Enrollment, Crosswalk and Landscape files for the respective year.This analysis includes HMO, POS, local PPO, regional PPO, and PFFS plans. Enrollment counts in publications by firms operating in the Medicare Advantage market, such as company financial statements, might differ from KFF estimates due to inclusion or exclusion of certain plan types, such as SNPs or employer plans.To calculate federal spending on the quality bonus program, we first obtained information on star ratings from the Part C and Part D Performance Data, Star Ratings Data Table for the previous plan year. These are the ratings on which a plan’s benchmark is based. We then determined each plan’s benchmark using these data and information from the Medicare Advantage Rate Book, Rate Calculation Data, which provides the benchmark by county for plans with a 5%, 3.5% and 0% bonus. A plan’s increase in payment per enrollee under the quality bonus program is equal to the difference between its quality adjusted benchmark (either the 5% or 3.5% bonus rate) and the benchmark if the plan was not in bonus (0% bonus rate), multiplied by the relevant percentage based on its star rating and year (for example, 65% for plans with 4 stars and 70% for plans with at least 4.5 stars in 2026). The increase per enrollee is multiplied by enrollees in March of each year to get total spending. Actual bonus spending will depend on the risk scores of Medicare Advantage enrollees. According to the plan payment data release by CMS, the average risk score of MA enrollees was above 1 for every year from 2015 through 2024 (the most recent year for which data are available), meaning our estimates likely understate actual spending.