Decoding Medicare Advantage Coding Intensity
In recent years, federal payments to Medicare Advantage plans, and how they are adjusted for enrollee health status, have come under increased scrutiny. Medicare Advantage plans receive a capitated amount for each enrollee, and these payments are “risk adjusted” based on the diagnosis codes reported by the insurer to the Centers for Medicare & Medicaid Services (CMS) for each enrollee. Plans receive higher payments for enrollees who are sicker and expected to have higher health care spending, and lower payments for enrollees who are healthier and expected to have lower health care spending. The purpose of this risk adjustment is to ensure plans receive adequate payments to treat sicker, higher-cost patients and reduce incentives to enroll primarily healthier, lower cost, beneficiaries. However, since the approach to risk adjusting payments relies heavily on the diagnosis codes recorded for Medicare Advantage enrollees, it provides a strong financial incentive for private insurers to capture as many diagnosis codes for each enrollee as possible, which increases payments and contributes to higher Medicare spending.
In contrast, payments under traditional Medicare only require the diagnosis codes necessary to support the services delivered. This means physicians and other health care providers do not have the same incentive to maximize the number of health care conditions documented through diagnosis codes. Differences in coding practices between traditional Medicare and Medicare Advantage (also referred to as coding intensity) mean that Medicare Advantage enrollees appear to be in worse health than they would if they received their Medicare benefits through traditional Medicare. Since the Medicare Advantage risk adjustment model is calibrated on traditional Medicare beneficiaries, the payments to Medicare Advantage plans are higher than necessary to cover expected costs, on average. According to the Medicare Payment Advisory Commission (MedPAC), in 2026, total payments to Medicare Advantage plans are $76 billion higher than traditional Medicare would spend for the same beneficiaries, of which $28 billion is attributed to coding intensity.
CMS has expressed a commitment to improving the accuracy of payments to Medicare Advantage and reducing the role coding practices play in determining the amount private plans receive from the federal government. Toward this end, the 2027 rate notice finalized a policy changing how certain diagnoses are considered when adjusting federal payments to Medicare Advantage plans for an enrollee’s health status. As policymakers and administration officials consider issues related to Medicare Advantage payments, this issue brief answers key questions about coding intensity, recent steps taken by CMS to address the impact of coding on payment, the effects on Medicare beneficiaries, and other proposals to improve Medicare Advantage payment accuracy.
What is coding?
Doctors and other health care providers include diagnosis codes on claims they submit to payers (either Medicare Administrative Contractors (MACs) for traditional Medicare or private insurers for Medicare Advantage) indicating a patient’s health conditions that support the health care services they delivered. The diagnosis codes for traditional Medicare beneficiaries are also used by CMS, along with other information, to develop a risk adjustment model estimating the relationship between a person’s health status (expressed as a “risk score”) and their projected health care spending. Medicare Advantage insurers submit the diagnosis codes documented by health care providers serving their enrollees to CMS for use in adjusting the payments the plans receive from the federal government using this risk adjustment model.
While the diagnosis codes used to develop the risk adjustment model only come from the claims providers submit for services rendered to traditional Medicare beneficiaries, those used to adjust payments to Medicare Advantage plans can be supplemented in two ways. First, Medicare Advantage plans may conduct health risk assessments (HRAs) and include the diagnosis codes for any conditions identified during this questionnaire in what is submitted to CMS – even when there are no related services delivered during the year to treat those conditions. KFF analysis finds that insurers often use rewards and incentives to encourage enrollees to complete HRAs. Second, Medicare Advantage plans may conduct chart reviews, which examine a person’s medical records, sometimes using AI tools, to determine if they are consistent with the information submitted by health care providers to the insurer. KFF analysis finds that chart reviews are used to add diagnosis codes that do not otherwise appear on a record for an encounter with a physician, increasing payments from CMS to Medicare Advantage insurers for one in six Medicare Advantage enrollees.
What is coding intensity?
Coding intensity is the degree to which a person’s health care conditions are documented through diagnosis codes. Differences in coding patterns across groups of beneficiaries, such as Medicare Advantage enrollees and traditional Medicare beneficiaries, or those in Medicare Advantage plans sponsored by different insurers, are described as differences in coding intensity. Higher coding intensity is not necessarily fraudulent, but fraud can contribute to higher coding intensity.
Because Medicare Advantage payments are generally higher for enrollees with more diagnosis codes (and therefore higher risk scores), private insurers have an incentive to document more health conditions, but there is no similar incentive in traditional Medicare. Recognizing this incentive, lawmakers have required CMS to reduce Medicare Advantage risk scores by at least 5.9% across the board before adjusting payments to private plans. However, that adjustment does not fully account for difference in coding patterns, and a number of studies have documented that risk scores are still higher in Medicare Advantage after applying the coding intensity adjustment than they would be if enrollees received their Medicare benefits under traditional Medicare. The magnitude of the uncorrected coding intensity after the adjustment has varied over time, ranging from as low as 2% in 2016 to 10% in 2023, and is estimated to be approximately 4% in 2026, according to MedPAC. The magnitude also varies by insurer and is larger for insurers comprising a larger share of enrollment. See Box 1 for an illustrative example of higher coding intensity and the effect on Medicare Advantage payments.
Box 1. Illustrative Example of How Higher Coding Intensity in Medicare Advantage Increases Payments to Private Insurers.
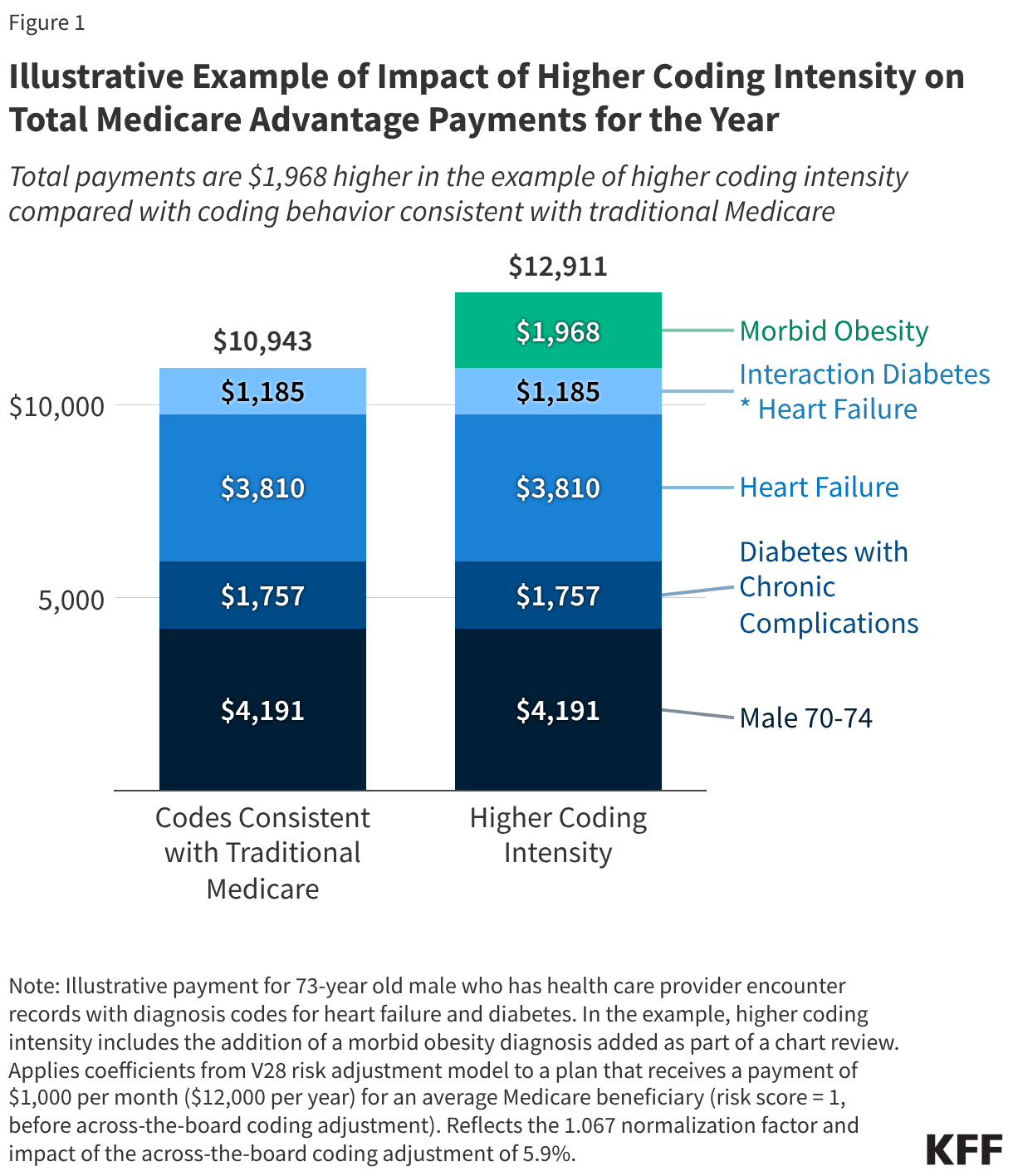
The risk adjustment model, which is used to assign a risk score to all Medicare Advantage enrollees, specifies “coefficients” for each factor that contributes to a person’s risk score. Each coefficient reflects the average marginal impact, or how much higher traditional Medicare spending is expected to be, due to that factor. To illustrate how coding intensity increases Medicare Advantage payments, consider Mr. Smith, who is 73-years old, living in the community, and received health care services to treat type 2 diabetes and heart failure last year. He is enrolled in a Medicare Advantage plan that receives $12,000 per year for an average Medicare beneficiary (risk score = 1).
If Mr. Smith’s Medicare Advantage plan codes consistent with traditional Medicare, the coefficients from the 2026 Risk Adjustment Model for each of the factors contributing to Mr. Smith’s risk score would be: Male 70-74 years – 0.396, Diabetes with Chronic Complications (HCC37) – 0.166, Heart Failure (HC226) – 0.336, and an interaction for having both diabetes and heart failure – 0.112. Mr. Smith’s risk score would be equal to the sum of these coefficients, 1.034, or 0.912 after applying the 1.067 normalization factor for the 2026 plan payment year (which is used to ensure the average risk score is equal to 1 in years beyond the initial estimation year) and the 5.9% coding adjustment (which applies to all plans regardless of whether they code consistent with traditional Medicare or have higher coding intensity). The plan would receive payments totaling $10,943 for Mr. Smith if he is enrolled the entire year ($12,000 * 0.912).
If instead the Medicare Advantage plan has higher coding intensity, it is possible that an additional diagnosis (or diagnoses) could be added to Mr. Smith’s record. For example, if the plan does a chart review and uncovers that Mr. Smith also meets the definition for morbid obesity, a condition that is documented more often in Medicare Advantage than traditional Medicare, his unadjusted risk score would increase by 0.186, bringing it up to 1.220. After applying the 1.067 normalization factor and 5.9% coding adjustment, his risk score would be 1.076. The plan would receive payments totaling $12,911 if Mr. Smith is enrolled the entire year ($12,000 * 1.076).
As a result of higher coding intensity, the plan receives nearly $2,000 more over the year for Mr. Smith – 18% more – than if it coded consistent with traditional Medicare (Figure 1).
What has CMS done to reduce coding intensity?
Risk Model Revisions. CMS periodically revises the risk adjustment model. Most recently, CMS updated the data used to calibrate the model and changed how certain conditions that were coded more frequently in Medicare Advantage than traditional Medicare were incorporated (or not). The move to the new model (referred to as V28 because it is the 28th version of the model) was phased in between 2024 and 2026.
Following full implementation of the new risk adjustment model, MedPAC estimated that the impact of coding intensity on Medicare Advantage payments has declined from increasing payments by 10% in 2022 to 4% in 2026 (the first year the V28 model is fully in effect). A recent analysis from CMS staff approached the analysis from a different angle – examining what the impact of using V28 would have been in 2022 if it had been in effect. That analysis finds uncorrected coding intensity (after applying the 5.9% adjustment) would have been between 1.5% and 2.0%, compared to 10% under the previous risk adjustment model (V24) that was in effect in 2022. This is consistent with the findings of other researchers, but the estimate for 2022 is not directly comparable to the MedPAC analysis because the CMS analysis modeled the impact of V28 in an earlier year in which it was not in effect, while MedPAC looks at the uncorrected coding intensity using the risk model in effect in the current payment year (2026).
Analyses of Medicare Advantage risk score trends have consistently found that coding intensity grows over time. Thus, the CMS staff estimate that uncorrected coding intensity would have been between 1.5% and 2.0% if the V28 model had been fully implemented in 2022 is consistent with MedPAC’s higher estimate of uncorrected coding intensity in 2026 of 4%, which incorporates growth in coding intensity between 2022 and 2026.
Coding Intensity. CMS also routinely makes other changes to the risk adjustment process separate from moving to a new model. For example, in the 2027 rate notice, CMS finalized a policy to exclude diagnosis codes added for enrollees based on chart review records that are not linked to an encounter with a health care provider (referred to as “unlinked” chart reviews). CMS estimates the new policy will reduce average payments to Medicare Advantage plans by 1.5% compared to what they would have been otherwise. While that estimate is similar in magnitude to the CMS staff estimate of uncorrected coding intensity in 2022 if the V28 model had been in effect, the two are not directly comparable because the impact of removing unlinked chart reviews applies to the 2027 plan year payment.
The use of chart reviews has come under scrutiny because analysis of Medicare Advantage insurers’ coding practices consistently finds that chart reviews are the primary contributor to higher coding intensity in Medicare Advantage. However, chart reviews are likely to continue to contribute to higher coding intensity in Medicare Advantage even after excluding diagnoses from unlinked chart reviews. Based on KFF analysis of Medicare Advantage encounter data for 2022, diagnoses from unlinked chart reviews comprised one-third of all diagnoses added through the chart review process in 2022, meaning that diagnoses from chart reviews that were linked to an encounter account for most of the diagnosis codes added during the chart review process.
Additionally, it is likely that an even smaller share of all diagnoses added on chart reviews will be impacted by the new policy to exclude diagnosis codes from unlinked chart reviews because the condition categories for which specific diagnoses were most commonly added in an unlinked chart review in 2022 were substantially impacted by the move to the V28 risk adjustment model. For example, vascular disease was among the most common conditions added on an unlinked chart review in 2022 that increased payment, but this condition category was substantially narrowed as part of the shift to V28 – meaning that many of these diagnoses codes would no longer count towards payment under the risk adjustment model regardless of the policy change related to unlinked chart reviews. Finally, the impact could be less than CMS estimates if insurers put more effort into linking chart reviews to encounters so that included diagnoses can be considered for risk adjustment purposes.
How are Medicare beneficiaries impacted by coding intensity and changes to the risk adjustment model?
Since higher risk scores increase Medicare payments to plans, higher coding intensity provides plans with the option to offer more extra benefits to enrollees, such as dental, vision, and hearing coverage, as well as reduced cost sharing. In addition, this additional funding from the federal government can be used for other purposes, such as increasing plan margins or paying for more advertising, as long as the Medicare Advantage insurer meets the minimum medical loss ratio required under law. (The medical loss ratio is the share of premium revenues going to pay for claims versus administrative overhead and profit.)
Industry representatives have raised concerns that payment changes, including efforts to address coding intensity, could result in plans offering fewer extra benefits or raising costs for Medicare Advantage enrollees. While there have been some changes to plan benefits and costs following the implementation of V28, including modest increases in out-of-pocket limits and decreases in some extra benefits, such as the availability of funds provided to pay for over-the-counter drugs and supplies, private insurers have generally absorbed a large portion of payment changes. An analysis of the first two years of the phase in of the new risk score model finds that insurers reduced benefits or raised costs by between 17% and 24% of the anticipated reduction in plan payments. That is a smaller effect than previous analysis of the impact of changes to Medicare Advantage payments, which found that private insurers passed through about half of the payment change in the form of fewer benefits and/or higher costs.
What additional steps can be taken to improve the accuracy of Medicare Advantage payments?
Policy proposals to address the remaining uncorrected coding intensity in Medicare Advantage include expanding the sources of diagnoses that are ineligible for risk adjustment to include all chart reviews and HRAs, increasing the 5.9% across-the-board adjustment to risk scores, or applying a tiered adjustment to risk scores based on historical coding intensity (so plans with higher coding intensity in previous years would have larger adjustments to their risk scores). Additionally, updates to the risk score model, such as those proposed but not finalized by CMS for 2027, may also better align the adjustments for health status to the expected impact on spending by incorporating more recent data to better reflect current treatment patterns and costs.
Beyond coding intensity, favorable selection into Medicare Advantage also increases payments above what traditional Medicare would spend for the same beneficiaries. Favorable selection occurs when the people who enroll in Medicare Advantage have lower actual health care use and spending, on average, than what is predicted by the risk score model. For example, previous KFF analysis found that Medicare beneficiaries who enroll in Medicare Advantage have lower spending than those who remain in traditional Medicare, after adjusting for health risk using the risk adjustment model. MedPAC estimates that the largest component of higher payments to Medicare Advantage plans relative to traditional Medicare is favorable selection into Medicare Advantage. The impact of favorable selection has been relatively stable over time, ranging between 9% and 11%, according to MedPAC; in other words, resulting in payments to Medicare Advantage plans for enrollees that are 9% to 11% higher than costs would be in traditional Medicare. In 2026, favorable selection is estimated to add $57 billion to Medicare spending.
To address the impact of favorable selection on Medicare Advantage payments, policymakers could make changes to the maximum amount the federal government is willing to pay Medicare Advantage plans, also known as benchmarks. One approach is an across-the-board reduction in benchmarks, such as the “discount rate” proposed by MedPAC. This would account for Medicare Advantage enrollees having lower expected health care spending, before any effects of Medicare Advantage plan design, than traditional Medicare beneficiaries with similar risk profiles, on which current benchmarks are based. Other options include expanding the sources of data used in the risk adjustment model to predict a Medicare Advantage enrollee’s costs, such as prescription drug claims, clinical data from electronic health records, or certain measures currently included in the Consumer Assessment of Healthcare Providers and Systems (CAHPS) (see for example, a recent proof-of-concept study). These measures could be applied on equal footing between Medicare Advantage and traditional Medicare, and among different Medicare Advantage plans. In addition, two-sided reinsurance, which would provide additional payments to insurers with enrollees who have extremely high and unexpected costs and require insurers with enrollees with substantially lower than predicted spending to make payments into the program, could be added to the Medicare Advantage payment system. That would reduce the financial rewards for attracting enrollees who use substantially fewer health care services and protect insurers against the financial costs of enrollees who use substantially more health care services.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.