A Closer Look at the Growing Role of Special Needs Plans in Medicare Advantage
Enrollment in Medicare Advantage, the private plan alternative to traditional Medicare, has increased steadily over the past two decades, and since 2023, more than half of eligible beneficiaries have enrolled in Medicare Advantage. Amidst this growth, an increasing number of beneficiaries are enrolling in special needs plans (SNPs), especially since 2018, when SNPs became a permanent part of the Medicare Advantage program. SNPs now account for 21% of all Medicare Advantage enrollees, compared with just 13% in 2018. The increase in the share of Medicare Advantage enrollees in SNPs also means that SNPs contribute disproportionately to the growth in Medicare Advantage enrollment. For example, between 2024 and 2025, growth in SNPs comprised nearly half (48%) of the total increase in Medicare Advantage enrollment.
There are three types of SNPs, and enrollment in each is restricted to specific groups of beneficiaries, all of which comprise some of the highest-need beneficiaries in the Medicare population. Over 4 in 5 (82%) SNP enrollees are enrolled in dual eligible SNPs (D-SNPs), which are limited to people with both Medicare and Medicaid (“dual-eligible individuals”). Dual-eligible individuals tend to have lower incomes, more chronic conditions, and more functional and cognitive impairments than Medicare beneficiaries without Medicaid coverage. The two other types of SNPs are chronic condition SNPs (C-SNPs, 16% of enrollees), which are limited to people with certain chronic conditions, and institutional SNPs (I-SNPs, 2% of enrollees), which are limited to people who require an institutional level of care. All SNPs are required to have a model of care, or framework detailing how the plan will identify the needs of each enrollee and address those needs through the plan’s care management practices. Other requirements vary across the three types of SNPs. D-SNPs may have additional requirements depending on the state in which they operate. (See Box 1 for additional information.)
In recent years, the Centers for Medicare and Medicaid Services (CMS) has made several changes to requirements for D-SNPs and other Medicare Advantage plans, which may affect insurer decisions about the types of plans they offer and promote. To better understand the growing role of SNPs in Medicare Advantage and the potential implications for beneficiaries of changes to SNP and Medicare Advantage plan requirements, this brief examines SNP enrollment patterns and trends using recent Medicare Advantage enrollment data published by CMS.
Key Takeaways
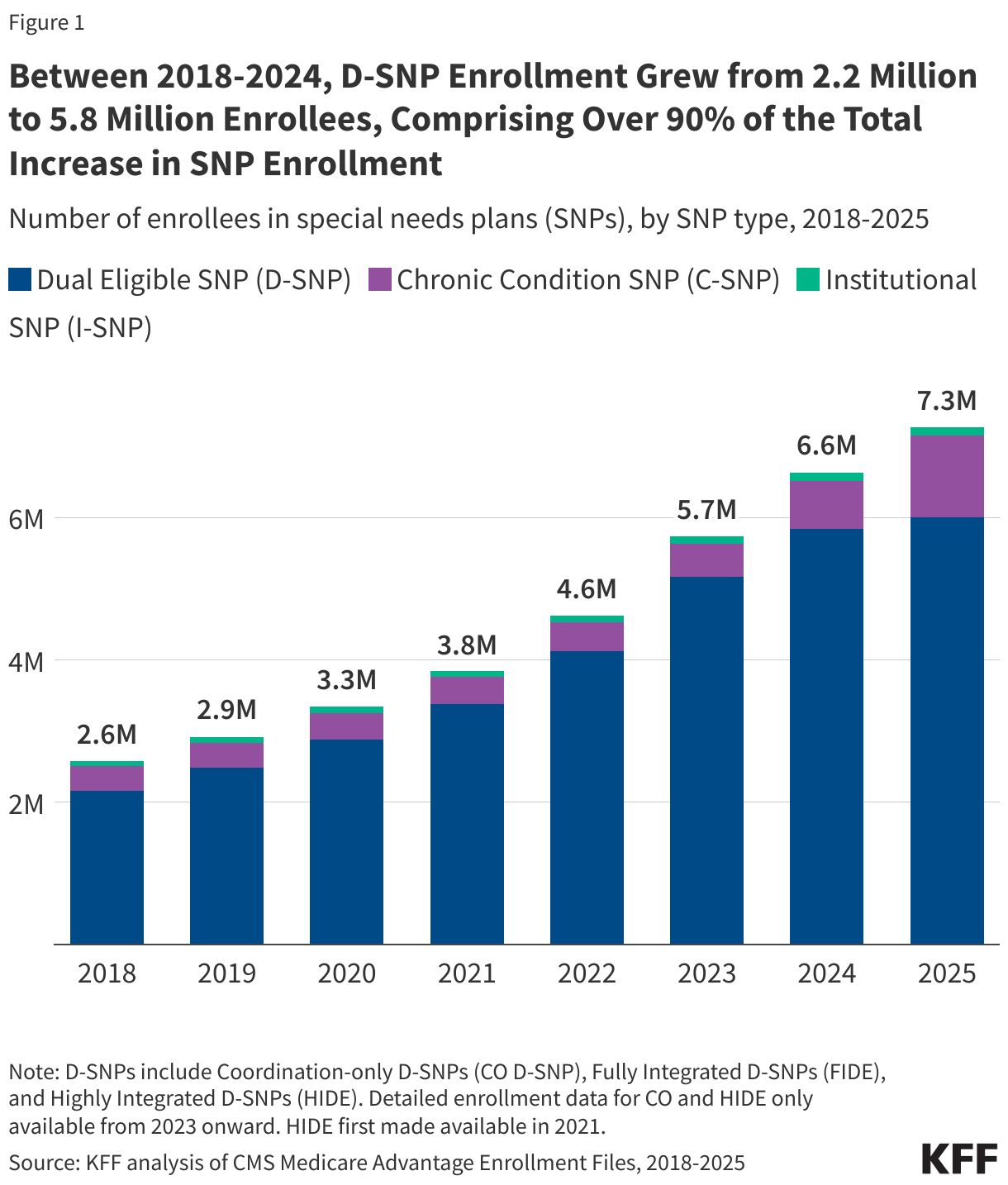
- Since 2018 when SNPs became a permanent part of the Medicare program, SNP enrollment has tripled, rising from 2.6 million to 7.3 million, an increase of nearly 4.7 million enrollees.
- Through 2024, growth in SNPs was driven by an increase in enrollment in D-SNPs, which grew from 2.2 million enrollees in 2018 to 5.8 million enrollees in 2024, comprising more than 90% of SNP enrollment growth over that time.
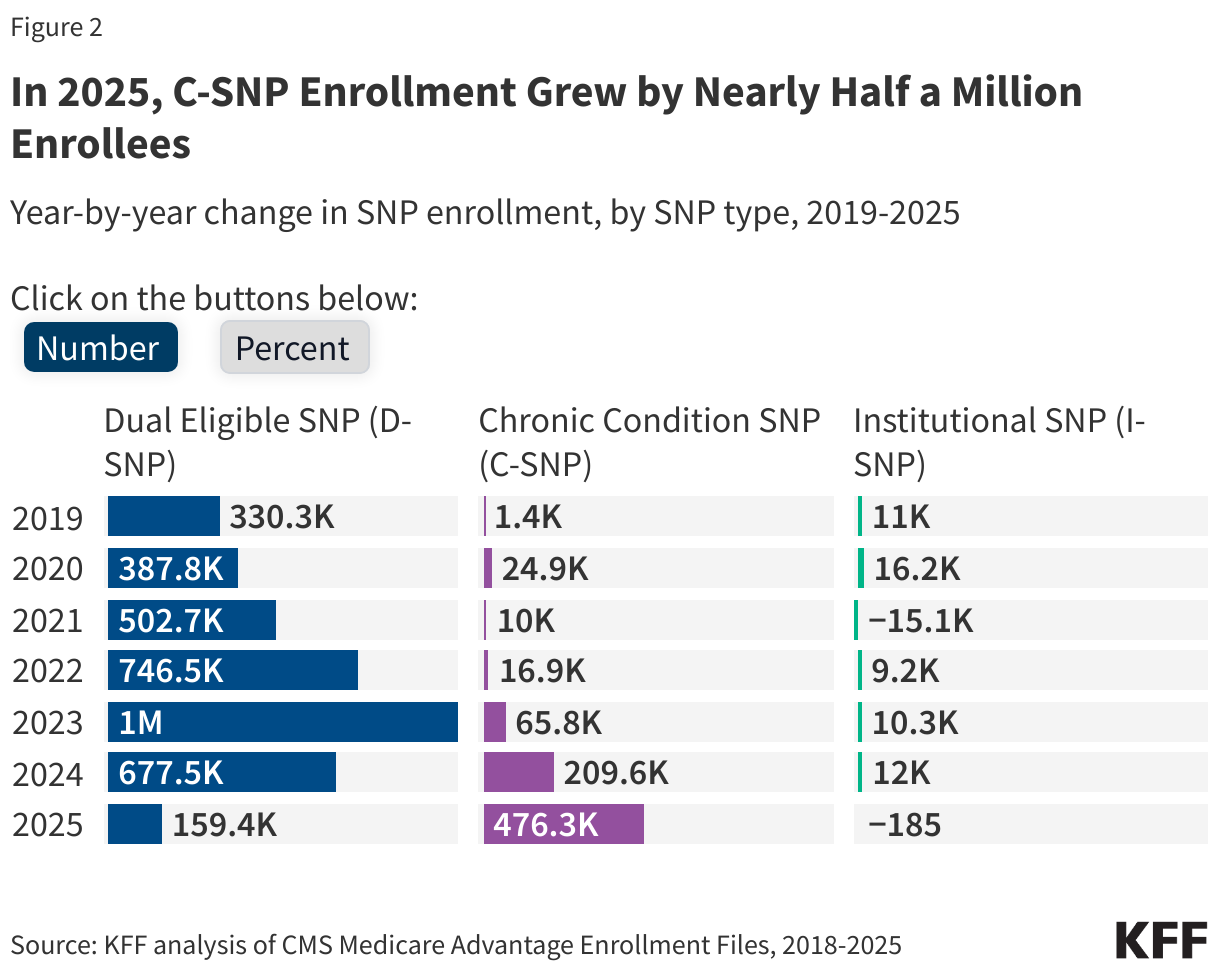
- C-SNPs comprised 75% of total SNP enrollment growth between 2024 and 2025, in contrast to prior years, where enrollment growth was mainly in D-SNPs. In 2025, C-SNP enrollment increased by 476,300 new enrollees, triple the increase in D-SNP enrollment (159,400 new enrollees).
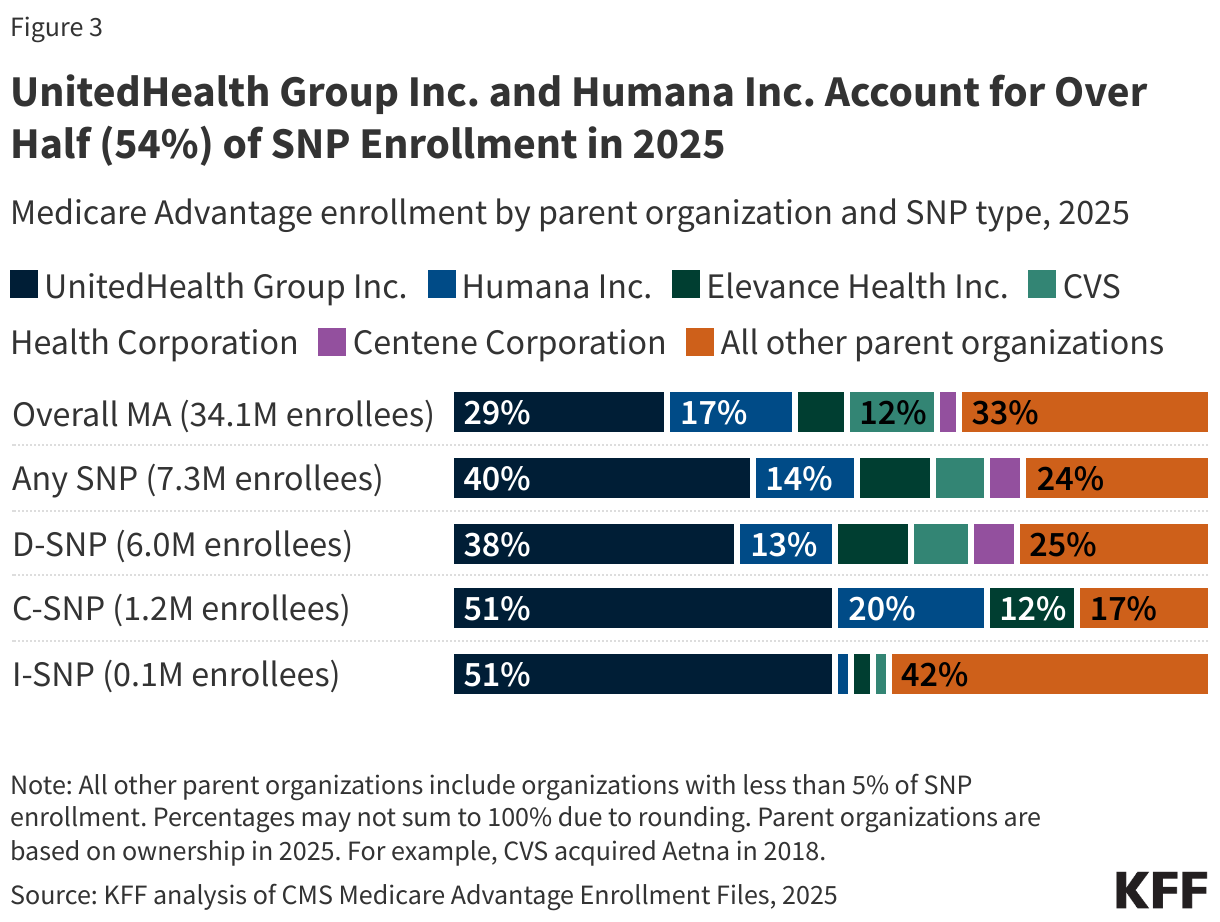
- A small share of SNP enrollees, just 14%, are in plans administered by non-profit insurers. SNP enrollment is highly concentrated among a small number of large national carriers, with UnitedHealth Group and Humana plans comprising over half (54%) of total SNP enrollment. UnitedHealth Group accounts for half of all C-SNP enrollees.
- The acceleration of C-SNP enrollment growth and slowing of D-SNP enrollment growth coincided with implementation of new rules for D-SNPs requiring greater integration between Medicare and Medicaid. C-SNPs are not required to have a similar level of integration.
From 2018-2024, growth in SNP enrollment was driven by increases in D-SNP enrollment, plans for dual-eligible individuals.
From 2018, when SNPs became a permanent part of the Medicare Advantage program, through 2024, growth in SNP enrollment was predominantly due to growth in enrollment in D-SNPs. In 2018, 2.2 million people were enrolled in a D-SNP, and in 2024, 5.8 million people were enrolled in a D-SNP. That increase comprises more than 90% of the total increase in SNP enrollment between 2018 and 2024.
C-SNP enrollment and I-SNP enrollment also increased during this period, though on a smaller scale relative to D-SNP enrollment growth. C-SNP enrollment grew from 346,000 enrollees in 2018 to 674,500 enrollees in 2024, and I-SNP enrollment grew from 71,500 enrollees in 2018 to 115,100 enrollees in 2024.
SNPs receive higher per capita payments under the Medicare Advantage payment system, on average, because enrollees have higher expected spending due to their higher health care needs. It is well-documented, however, that Medicare Advantage pays more for Medicare Advantage enrollees than spending would be for the same people if they were covered under traditional Medicare, and in 2025, MedPAC estimates that payments were 20% higher, on average. The higher payments are largely driven by the risk adjustment system, which pays more for people who are sicker, and less for those who are healthier, relying heavily on diagnosed heath conditions to determine adjustments to payment based on health status. SNPs are potentially better positioned to leverage this system to increase their payments relative to enrollee’s costs, contributing to higher margins for SNPs, on average, than other Medicare Advantage plans. MedPAC found that in 2022, the average margins for D-SNPs (7.5%) and C-SNPs (7.4%) were double the average margins of Medicare Advantage plans overall (3.6%). In turn, those higher payments leave more resources for plans to offer supplemental benefits that appeal to a population with complex health care needs.
Enrollment growth in SNPs from 2024-2025 was driven by an increase in enrollment in C-SNPs, plans for people with chronic conditions.
In recent years, CMS has made several changes to requirements for Medicare Advantage plans generally available to the public and D-SNPs, but not C-SNPs, which may affect insurer decisions about what types of plans to offer. Starting in 2022, CMS no longer contracts with conventional Medicare Advantage plans that enroll at least 80% dual-eligible individuals (“D-SNP look-alikes”). In 2025, this threshold was lowered to 70% and is scheduled to be lowered to 60% starting in 2026. Additionally, beginning in 2025, fully integrated dual eligible (FIDE) SNPs and highly integrated dual eligible (HIDE) SNPs have new enrollment, benefit, and coordination requirements (see Box 1 for additional details). The additional requirements are intended to promote better integration between Medicare and Medicaid for enrollees but could make D-SNPs less attractive to private insurers. These requirement changes could incentivize efforts to enroll more dual-eligible individuals in C-SNPs, which are not subject to the look-alike thresholds like conventional Medicare Advantage plans or Medicaid integration and coordination requirements like D-SNPs, particularly since many dual-eligible individuals have chronic conditions that may qualify them for C-SNP enrollment.
In contrast to previous years when enrollment growth in SNPs was driven by increased enrollment in D-SNPs, the largest increase in enrollment in SNPs from 2024 to 2025 was in C-SNPs, comprising more than three-quarters of the change in overall SNP enrollment. C-SNP enrollment increased sharply, rising by 476,300 enrollees from 2024 to 2025. That translates into a 71% jump over a one-year period. D-SNP enrollment and I-SNP enrollment remained relatively stable over the same period, with D-SNP enrollment growing by only 3% (159,400 enrollees) and I-SNP enrollment staying essentially unchanged.
While C-SNP enrollment has increased more quickly since the D-SNP look-alike rules first went into effect in 2022, the change accelerated over the last year, as the rules tightened further and other Medicaid integration and coordination requirements for FIDE and HIDE SNPs went into effect. This is the first time that the number of additional C-SNP enrollees has surpassed the number of additional D-SNP enrollees. A recent analysis of 2025 enrollment data (not yet available to KFF) shows that through January of 2025, just under 20% of the increase in C-SNP enrollment was comprised of dual-eligible individuals.
Dual-eligible individuals comprised a larger share of enrollment in SNPs than in non-SNP Medicare Advantage plans. For example, in 2023, 93% of SNP enrollees were dual-eligible individuals, which aligns with the dominance of D-SNPs in the SNP market. Over 90% of I-SNP enrollees were also dual-eligible individuals in 2023, reflecting the fact that Medicaid is the primary payer of long-term care, so people relying on an institutional level of care are more likely to be enrolled in both Medicare and Medicaid. In 2023, a quarter of enrollees in C-SNPs were dual-eligible individuals, while 9% of enrollees in individual Medicare Advantage plans were dual-eligible individuals.
For all SNP types, enrollment is highly concentrated among a small number of large national carriers.
Across all three SNP types, which enroll some of the most vulnerable beneficiaries in the Medicare population, a few large national carriers account for larger shares of enrollment in the SNP market as compared with the overall Medicare Advantage market. The distribution of D-SNP enrollment by insurer is more heavily concentrated in UnitedHealth Group Inc. (38% vs 29%) and Elevance Health Inc. (10% vs 7%) than for the overall Medicare Advantage market. UnitedHealth Group Inc. accounts for half (51%) of all C-SNP enrollment. Additional firms comprising larger shares of enrollment in C-SNPs than in the overall Medicare Advantage market include Humana Inc. (20% vs 17%) and Elevance Health Inc. (12% vs 7%). Although UnitedHealth Group Inc. accounts for a majority (51%) of I-SNP enrollment in 2025, smaller insurers play a larger role in the I-SNP market than in the overall Medicare Advantage market (42% vs 33%). Overall, 14% of SNP enrollees are in a plan offered by a non-profit organization (16% of D-SNP enrollees, 3% of C-SNP enrollees, and 5% of I-SNP enrollees).
For dual-eligible individuals, D-SNPs offer more integration with Medicaid than C-SNPs.
To facilitate integration of Medicare and Medicaid coverage, D-SNPs are required to contract with state Medicaid agencies, while C-SNPs are not subject to additional integration requirements. The minimum D-SNP requirements, which are set at the federal level, differ across the three categories of D-SNPs and can change year-to-year during annual rule making. D-SNPs with higher levels of integration, HIDE and FIDE SNPs, have additional requirements (see Box 1 for more details). Additionally, D-SNPs can be designated as applicable integrated plans if they meet federal requirements, including exclusively aligned enrollment, covering at least some Medicaid services through the D-SNP or an affiliated Medicaid managed care plan, and a unified grievance and appeals system. Given the lack of C-SNP integration requirements, to the extent the acceleration in C-SNP enrollment was driven by dual-eligible individuals, efforts to encourage greater integration between Medicare and Medicaid may face challenges.
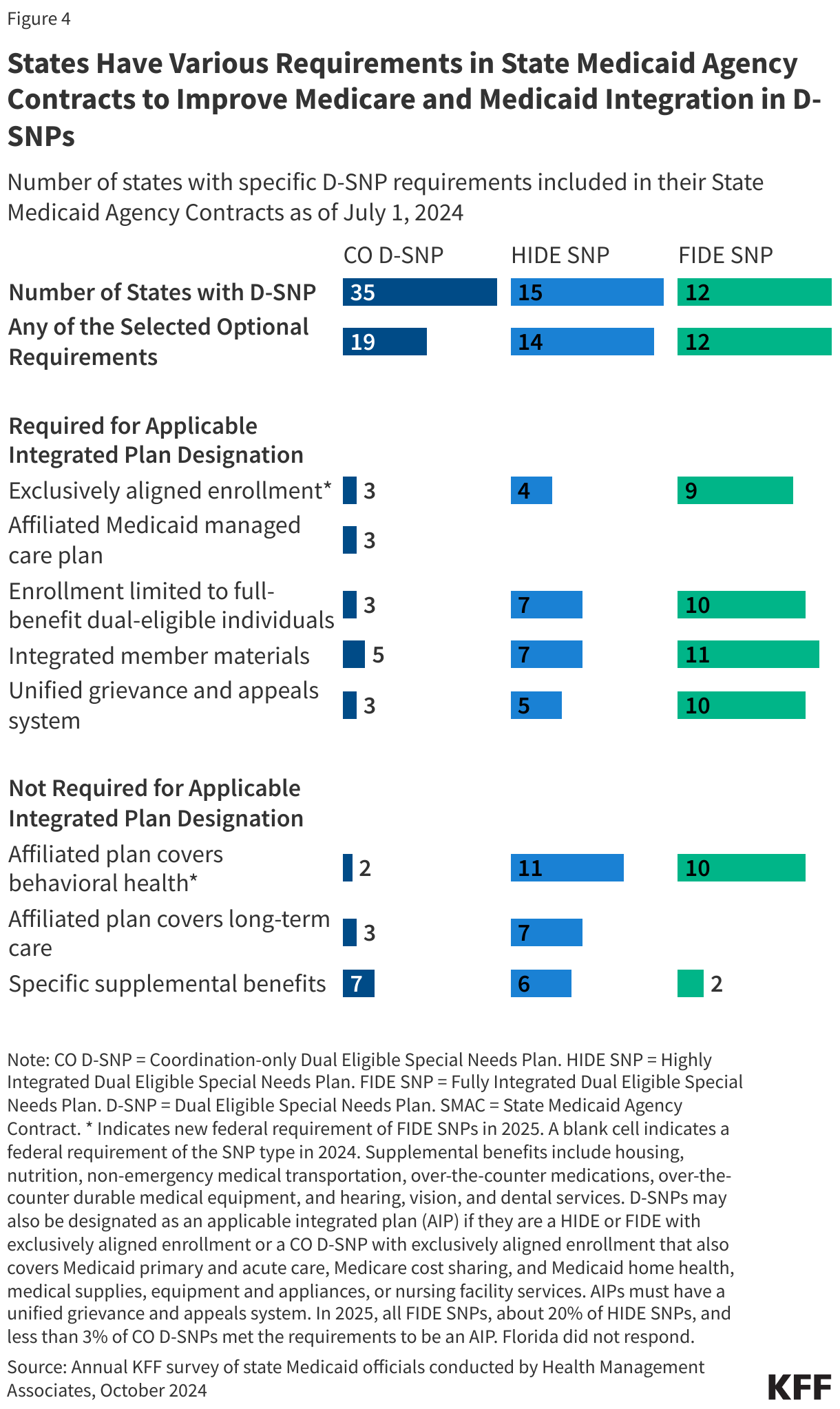
States may establish additional requirements for D-SNPs through their contracts. Responses from KFF’s 24th annual budget survey of Medicaid officials in all 50 states and the District of Columbia in July 2024 show that these requirements vary across the different types of D-SNPs. For example, just over half (19) of the 35 states with coordination-only D-SNPs required these plans to include any of the additional optional requirements, the most common of which was offering certain supplemental benefits (7 states) and providing integrated member materials, such as one summary of benefits document that provides information on benefits covered by both Medicare and Medicaid (5 states). HIDE and FIDE SNPs operated in less than half of states in 2024, though most states had additional requirements for these types of plans beyond the federal requirements (14 of 15 for HIDE SNPs and all 12 states for FIDE SNPs) (Figure 4). New federal requirements for HIDE and FIDE SNPs went into effect in 2025. For FIDE SNPs, these include exclusively aligned enrollment, which limits enrollment to full-benefit dual-eligible individuals who were enrolled in the affiliated Medicaid managed care plan, and the requirement that the affiliated plan cover behavioral health, and certain other Medicaid benefits. To the extent these were not previously required by states, the new requirements may represent an additional burden for Medicare Advantage insurers and could influence their decisions on which plans to offer. In 2024, most states with FIDE SNPs did have these requirements. Specifically, of the 12 states with FIDE SNPs, 9 required exclusively aligned enrollment and 10 required the affiliated Medicaid managed care plan to cover behavioral health. (New requirements for HIDE SNPs were not among the items asked in the budget survey.) While these requirements are intended to facilitate integration and coordination between the programs, the relatively low availability of HIDE and FIDE SNPs may limit how effective they are at achieving that goal.
Box 1. Types of Special Needs Plans
Dual Eligible Special Needs Plans
Dual eligible special needs plans (D-SNPs) are limited to people who are enrolled in both Medicare and Medicaid. There are three types of D-SNPs:
Coordination-only Dual Eligible Special Needs Plans: This type of D-SNP provides Medicare-covered services and is required to coordinate the delivery of benefits with the Medicaid program, contract with state Medicaid programs, and notify states when enrollees are admitted to an inpatient hospital or skilled nursing facility.
Highly Integrated Dual Eligible Special Needs Plans: This type of D-SNP must meet the requirements of coordination-only D-SNPs (except the notification requirements) and must also include coverage of long-term care, behavioral health, or both.
New for 2025: HIDE SNPs must have aligned service areas, meaning they must also have a Medicaid plan operating in the same counties as the D-SNP.
Fully Integrated Dual Eligible Special Needs Plans: This type of D-SNP must meet the requirements of coordination-only D-SNPs (except the notification requirements) and provide Medicare and included Medicaid covered services through a single managed care organization. The same organization that offers the FIDE SNP must also offer a Medicaid managed care plan for any Medicaid benefits not included in the FIDE SNP. In some cases, certain Medicaid benefits may be provided by the state or by a different health plan. FIDE SNPs are paid by Medicare for Medicare-covered services and supplemental benefits included in the plan, and by Medicaid for Medicaid-covered services.
New for 2025: FIDE SNPs must have exclusively aligned enrollment, meaning they may only enroll full-benefit dual-eligible individuals who are enrolled in both the FIDE SNP and the Medicaid plan sponsored by the same organization, and either the D-SNP or Medicaid plan must cover long-term care and all Medicaid benefits via a separate capitated payment arrangement.
Chronic Condition Special Needs Plans
Chronic condition special needs plans enroll individuals who have specific severe or chronic disabling conditions. Nearly all (97%) C-SNPs plans are for people with diabetes or cardiovascular conditions.
Institutional Special Needs Plans
Institutional special needs plans enroll individuals who need services to be provided in a long-term care facility for at least 90 days.
Methods
Data: SNP enrollment data are from the Special Needs Plan (SNP) data published by Centers for Medicare & Medicaid Services (CMS) in the Medicare Advantage (MA)/Part D Contract and Enrollment Data section in March of the respective year. Enrollment data are only provided for plan-county combinations that have at least 11 beneficiaries; thus, we exclude any plans that do not meet this enrollment threshold.
This analysis uses data from the CMS Medicare Advantage Benefit and Landscape files for the respective year. Medicare Advantage enrollment and dual-eligible beneficiary enrollment are based on analysis of the Centers for Medicare & Medicaid Services (CMS) Chronic Conditions Data Warehouse (CCW) research-identifiable Master Beneficiary Summary File (MBSF) Base in 2023.
Identifying dual-eligible enrollees as a share of SNP enrollees: Beneficiaries with a valid contract ID and plan ID in March 2023 were identified as enrolled in Medicare Advantage. To determine the type of plan in which the beneficiary was enrolled, the contract ID and plan ID were matched to the March 2023 Monthly Enrollment by Plan, or the Special Needs Plan Report data published by CMS. This includes enrollment in all private plans which are predominately Medicare Advantage plans.
Counts of dual-eligible individuals include both full-benefit and partial-benefit dual-eligible individuals. Dual status in March (03) 2023 was identified using the Medicare monthly dual status code DUAL_STUS_CD_03 with values of 01,02,03,04,05,06, or 08. Enrollees also had to have both Part A and B in March 2023 to be included in this analysis. We excluded enrollees from Puerto Rico and the Virgin Islands from this analysis.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.