Proposed Changes to Title X: Implications for Women and Family Planning Providers
Issue Brief
Key Takeaways
- The Trump administration has issued new proposed regulations for the federal Title X family planning program that would make significant changes to the program and to the types of providers that qualify for funding.
- These proposed regulations would:
- Block the availability of federal funds to family planning providers like Planned Parenthood that also offer abortion services;
- Curtail counseling and referrals to abortion services by Title X funded providers;
- Eliminate current requirements that Title X sites offer a broad range of medically approved family planning methods and non-directive pregnancy options counseling that includes information about prenatal care/delivery, adoption, and abortion; and
- Direct new funds to faith-based and other organizations that promote fertility awareness and abstinence as methods of family planning.
- Sites that do not offer abortion services may still qualify for Title X funds, but may decide not to participate because of concerns about clinical standards of care, medical liability, and burdensome administrative requirements.
- If fully implemented, the proposed changes to Title X would shrink the network of participating providers and have major repercussions for low-income women across the country that rely on them for their family planning care.
Introduction
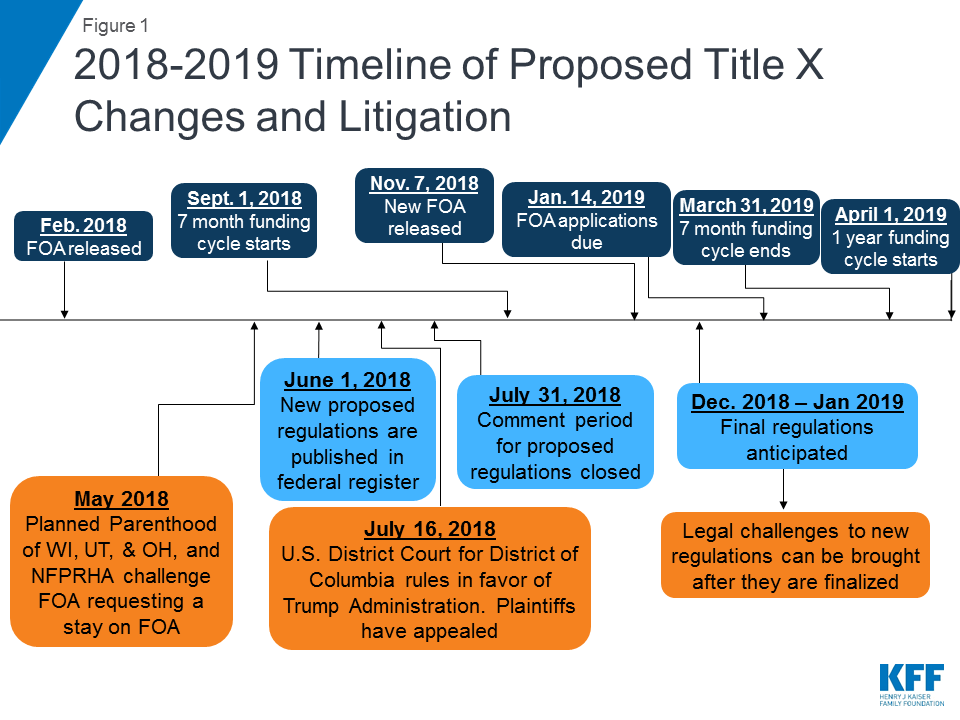
The Trump administration has taken numerous steps to alter significantly the Title X program, the federal grant program that supports family planning services to low-income women. These actions would block the availability of federal funds to family planning providers that also offer abortion services like Planned Parenthood, curtail counseling and referrals to abortion services by Title X funded providers, and direct new funds to faith-based and other organizations that promote fertility awareness and abstinence as methods of family planning. On June 1, 2018, the Trump administration issued a new proposed regulation that would restore Reagan-era restrictions regarding abortion and Title X that could significantly shrink the network of clinics available to provide family planning services to low-income women. This new proposed regulation comes in the midst of an already fraught and delayed new funding cycle for the Title X program that is being legally challenged by family planning groups and providers (Figure 1). This brief provides an overview of the Title X program, discusses the new 2018 funding announcement and related litigation, and reviews the Trump administration’s proposed regulations and the implications of these changes.
Background
The statute governing Title X requires that program funds must serve low-income populations at low or no cost, provide clients with a broad range of acceptable and effective family planning methods and services, and ensure that the services are voluntary.1 It also stipulates that funds may only go to entities where “abortion is not a method of family planning.” Current regulations interpret this provision to mean that Title X projects are prohibited from using Title X funds to pay for abortions and must keep any abortion-related activities financially separate from their Title X activities. Title X projects are required to provide nondirective counseling to pregnant women on prenatal care and delivery, infant or foster care, adoption, and abortion. Pregnant women desiring an abortion must be provided with a referral if asked, but the provider cannot promote abortion, schedule an appointment, negotiate rates, or arrange transportation for women desiring abortions.
Key Facts – Title X National Family Planning Program
- Title X, enacted in 1970, is the only federal program specifically dedicated to supporting the delivery of family planning care.
- Administered by the HHS Office of Population Affairs (OPA), and funded at $286.5 million for Fiscal Year 2018, the program serves over 4 million low-income, uninsured, and underserved clients.
- Nearly 4,000 clinics nationwide received Title X funding in 2017, including specialized family planning clinics such as Planned Parenthood centers, community health centers, state health departments, as well as school-based, faith-based, and other nonprofit organizations.
- Title X grants made up about 19% of revenue for participating clinics in 2017, providing funds to not only cover the direct costs of family planning services, but also pay for general operating costs such as staff salaries, staff training, rent, and health information technology.
- Participating programs have been required to offer a broad range of FDA-approved contraceptive methods onsite and follow the CDC and OPA guidelines for Quality Family Planning (QFP) including: counseling about correct and consistent use; onsite dispensing, “quick start” (to begin contraception at time of visit); provide or prescribe multiple cycles of pill, patch, or ring; easily and inexpensively available condoms; and, if a client’s method is not available on-site/same day, offer an alternate method.
2018 Title X Funding Opportunity Announcement (FOA)
On February 23, 2018, the Trump administration issued the 2018 Title X Funding Opportunity Announcement (FOA) after a five-month delay. Three Planned Parenthood affiliates and the National Family Planning and Reproductive Health Association (NFPRHA) sued HHS claiming that the FOA violates the Title X statute and regulations and was not promulgated through proper rulemaking.2 ,3 On July 16, 2018, the U.S. District Court for the District of Columbia ruled in favor of the Trump administration, a decision the plaintiffs have since appealed.
The Office of Population Affairs funded all of the prior grantees, but issued contracts for only 7 months, ending March 31, 2019. On November 7, 2018, the Trump administration issued a new FOA due on January 14, 2019, for grants beginning April 1, 2019, and although the proposed regulations have not yet been finalized, many anticipate them to be published in late 2018/early 2019. The November 2018 FOA includes priorities that stand in sharp contrast to those of the Obama administration (which focused on achieving clinical standards of care and the provision of a broad range of contraceptive methods). Like the February 2018 FOA, the November 2018 FOA elevates natural family planning, infertility services, and abstinence counseling to a program priority. The FOA also promotes the provision of family planning care in a primary care setting and “fostering interaction with faith-based organizations,” deemphasizing the role of specialized family planning clinics such as Planned Parenthood, a significant provider of family planning services to low-income women in the US.4 References to hormonal contraception and clinical guidelines such as the QFP were re-introduced in the November 2018 FOA after being excluded in the February 2018 FOA.
New Proposed Regulations
On June 1, 2018, new proposed regulations for Title X grants were published in the Federal Register with a 60-day public comment period, which closed July 31, 2018. The proposed regulations would make many changes to the requirements for Title X projects that could significantly limit the network of providers who can qualify for funds; restrict the ability of participating providers from discussing and referring for abortion; and make other programmatic changes that could dramatically reshape the program and provider network available to low-income women through Title X. Specifically, they would:
Ban federal Title X funds from going to any provider that also provides abortion services. The Title X statute specifies that no federal funds appropriated under the program “shall be used in programs where abortion is a method of family planning.” HHS has changed its interpretation of this provision over time, but throughout the history of the program, the ban has generally been understood to mean that Title X funds cannot be used to pay for or support abortion, as is the policy under the current regulations (Appendix 1). The proposed regulation would:
- Require that Title X funded activities have full physical and financial separation from abortion-related activities. In addition to separate accounting and electronic and paper health records, providers would need to have separate treatment, consultation, examination and waiting rooms, office entrances and exits, workstations, signs, phone numbers, email addresses, educational services, websites, and staff. This new requirement would essentially disqualify any provider from receiving Title X funds if they also offered abortions.
- Prohibit grantees and subrecipients from participating in a variety of “activities that encourage abortion” including lobbying, attending an event during which they engage in lobbying, or paying dues to a group that uses the funds for lobbying. The proposed regulations are nearly identical regulations issued under President Reagan (Appendix 1), which were legally challenged by Title X projects and providers, but were ultimately upheld by the Supreme Court in Rust v. Sullivan in 1991 (Box 1).
Box 1 – Rust v. Sullivan, 500 U.S. 173 (1991)
In 1988, the Reagan administration issued proposed regulations that prohibited Title X projects from engaging in counseling concerning, referrals for, and activities promoting abortion as a method of family planning. The regulations also required Title X projects to be financially and physically separate from any prohibited abortion-related activities including separate personnel, accounting records, treatment, consultation, examination and waiting rooms, and banned signs or materials promoting abortion.
Title X grantees and doctors challenged the regulations with a lawsuit that ultimately reached the U.S. Supreme Court in Rust v. Sullivan. In 1991, the Supreme Court held that the regulations were a permissible interpretation of the statute and did not violate the First or Fifth Amendments. The Court ruled that the government is permitted to favor childbirth over abortion and may allocate funds consistent with this viewpoint without violating a woman’s right to choose to terminate her pregnancy.
Restrict referrals for abortions: The proposed regulations interpret counseling and referral for abortion to be activities that would be considered providing “abortion as a method of family planning” and would prohibit Title X grantees and subrecipients from providing, promoting, referring for, supporting, or presenting abortion services to patients.
The proposed regulations would allow for a limited exception –only if a pregnant Title X patient has already decided to have an abortion and explicitly requests a referral. In this case, a doctor (and not any other clinical staff) would be permitted–but not be required—to provide the pregnant woman with a list of health care providers that offer comprehensive prenatal care, some of which also provide abortion. The Title X doctor may not indicate which providers on the list offer abortion services.
Eliminate the requirement for nondirective pregnancy options counseling: The new regulations would eliminate the requirement that Title X projects provide nondirective pregnancy options counseling that includes discussion of abortion as an option. This would now be left up to each site and organization that participates (which may include those that do not support abortion) to decide whether to mention abortion as an option to pregnant women who seek counseling. However, the extent to which counseling for abortion is permissible is unclear. The text of the proposed regulations specifies that all pregnant women must be referred to prenatal care, regardless of their stated wishes and would not allow discussion of abortion during that counseling session. The preamble, a non-binding introduction to the regulation, states: “Recognizing, however, the duty of a physician to promote patient safety, a doctor would be permitted to provide nondirective counseling on abortion. Such nondirective counseling would not be considered encouragement, promotion, or advocacy of abortion as a method of family planning.”
New primary care requirements for Title X projects: Title X projects would be required to offer “comprehensive primary health services onsite or have a robust referral linkage with primary health providers who are in close physical proximity.” There is no definition of the term “close physical proximity” in the regulations.
Extended federal oversight, enforcement, and recordkeeping: The new proposed regulations grant enforcement and oversight authority of grantees and subrecipients to the Secretary of HHS. In the past, grantees were subject to review by HHS, but all subrecipients and partners were under the authority of the grantee organization. In addition, there are new and significant informational requirements of the grantees including reporting detailed information about all subrecipients, referral agencies, and community partners including a description of the extent of the partnership and the process by which the grantee will “ensure adequate oversight and accountability for quality and effectiveness of outcomes.” Title X grantees and subrecipients would also be required to maintain and report records indicating the age of minor clients and the age of their sexual partners as specified under state notification laws.
Eliminates requirement that projects offer the full range of family planning methods. The only types of family planning methods that the proposed regulations specify that all Title X projects must offer are natural family, planning methods, infertility services, and services for adolescents. No Title X project would be required to provide every acceptable and effective family planning method or service. Instead, the regulation only requires a “broad range of family planning methods” that includes, but is not limited to: male condom, spermicide, cervical cap, fertility awareness based methods, female condom, diaphragm, vaginal contraceptive ring, IUD, oral contraceptives, shot/injection, implantable rod, vasectomy, and sexual risk avoidance (or abstinence). Under current regulations, any organization that desires to provide only a single method, or a limited number of methods of family planning, may participate, as long as the Title X project as a whole offers a broad range of methods. However, this provision is emphasized in the new proposed regulations, and there is no requirement that the services include a contraceptive method.
New definition for “Low-income:” The proposed regulations would modify the definition of “low-income” (currently defined as income below 100% of the federal poverty level) to include women who receive employer-sponsored insurance offered by an employer who refuses to cover contraceptives in their plan due to religious or moral objections. In October 2016, the Trump administration issued new interim final regulations that significantly broaden the ability of employers to be exempt from the Affordable Care Act’s (ACA) contraceptive coverage requirement based on a religious or moral objection to contraceptives. Although several states have legally challenged these regulations, and there is currently a stay blocking their implementation pending the outcome of the litigation, in November 2018, following a public comment period, the administration issued final regulations which were similar to the 2016 interim final regulations in most regards. The Trump administration contends that women affected by the regulation could be able to obtain contraceptive services at Title X clinics. The revised definition of “low-income” would expand eligibility to this new group of women who do not meet the income guidelines but do not have contraceptive coverage. However, at this point, no additional funds have been made available to Title X clinics to accommodate this new eligibility group.
Implications of the Proposed Regulations
Access to family planning services is still a challenge for many low-income women. Should this proposed regulation become final, the impact would be far reaching and would change the network of providers that are eligible to participate, limiting rather than expanding access.
Family planning providers that also perform abortions would no longer be eligible to participate in Title X, dramatically reducing the network of family planning providers serving women under the program. The proposed regulations essentially disqualify any provider that offers abortion services or is affiliated with an abortion provider from receiving Title X funds. The provisions that require physical and financial separation would make it impossible for clinics like Planned Parenthood and any other provider that also offers abortion services to comply with the new requirements of the program. Furthermore, restrictions on infrastructure support and affiliations would make it impossible for them to continue to participate in Title X.
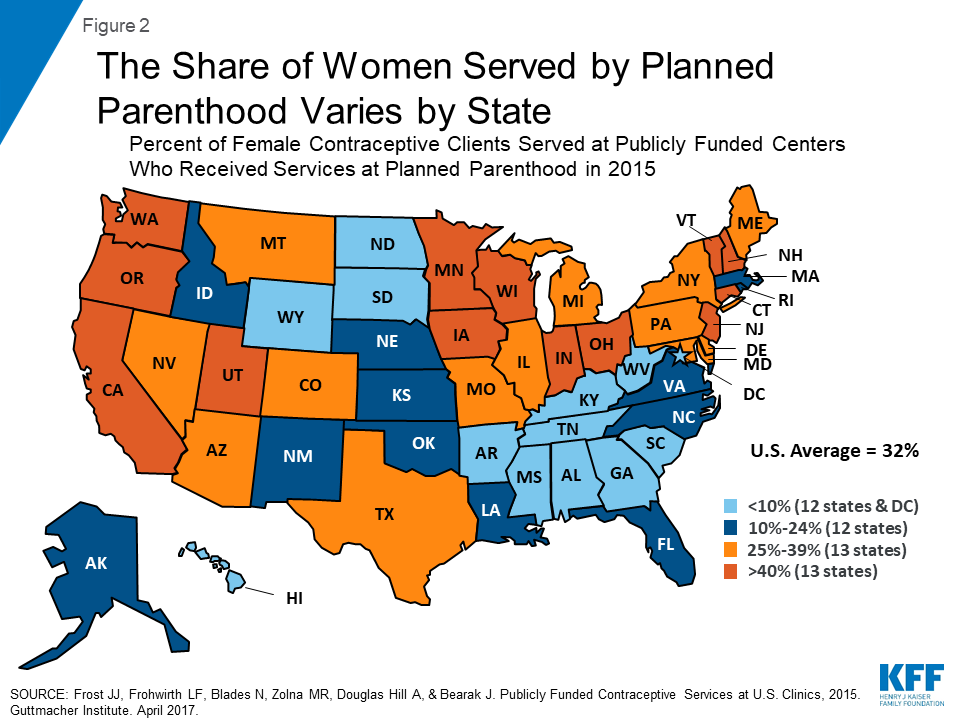
The impact of banning federal Title X funds to Planned Parenthood, in conjunction with the counseling and referral restrictions that would be imposed on Title X projects, will vary across the country. In 13 states, Planned Parenthood clinics were the site of care for over 40% of women who obtained publicly funded contraceptives (Figure 2).5 Research has shown that blocking Planned Parenthood from receiving public funds can reduce low-income women’s access to contraceptives.6 ,7 In 2013, the Wisconsin legislature approved family planning cuts directed at Planned Parenthood, which resulted in the closure of five Planned Parenthood clinics in rural areas. Women who used the Planned Parenthood clinics were referred to other clinics that were usually further away, with waiting lists, and that did not provide the full range of contraceptive methods.8 A study conducted by Health Management Associates for Planned Parenthood concluded that women in seven Wisconsin counties would have no alternative family planning provider should Planned Parenthood centers close there.9
The proposed restriction on referrals for abortions would compromise the quality of family planning care women receive through Title X providers. The Institute of Medicine’s landmark study on health care quality identified six dimensions of quality: safety, timeliness, patient-centeredness, effectiveness, efficiency, and equity.10 Providers that withhold information about abortion and, if provided, limit the list of providers that pregnant women seeking abortion are offered would compromise the quality of care they provide. Care offered under those restrictions would not be patient-centered, could lead to delayed care, and would be inequitable. Adherence to medical standards of care requires providers to offer patients referrals to the highest quality providers that can offer care in the timeliest manner and respects a patient’s decision to seek that care. In the event a woman is able to obtain a list of referrals that include abortion, the proposed regulation stipulates that only comprehensive prenatal care providers– some of whom also offer abortion — can be given to a pregnant woman (and only by a medical doctor). The referral could not show which of the prenatal providers also offer abortion. This list would primarily be comprised of hospitals and doctor’s offices, which, while accounting for roughly half of the abortion-providing facilities, only provide about 5% of all abortion procedures. In contrast, abortion clinics and nonspecialized clinics, such as Planned Parenthood, provided 90% of abortions.11 Services delivered at a hospital are much more costly than those provided in a clinic setting, and many private physicians do not accept Medicaid or uninsured patients. Women who live in rural communities or in states with few abortion providers would have to travel even greater distances to obtain abortion care at hospitals or doctor’s offices rather than be sent to freestanding abortion providers.
Restrictions on counseling and referral could place participating providers at risk of medical liability. Providers who still qualify for Title X funds because they do not offer abortion may find themselves facing a medical liability risk if they opt to participate in the program that restricts referrals for abortions. As Rosenbaum and her colleagues cite, the case of Wickline v. State of California finds that it is “no defense in a medical liability case to argue that physicians simply have followed a payer’s instructions,” which in this case, would be the Title X program.12 They argue that because Title X participating providers would be required to withhold information about services and referrals to qualified providers, they could be held liable and potentially jeopardize other funding they receive through the program that funds the federal Community Health Center program. Some community health centers may decide to discontinue their Title X participation because of concerns about medical liability and because this regulation would force them to offer their patients poorer quality care by restricting their ability to offer counseling and referral that includes abortions.
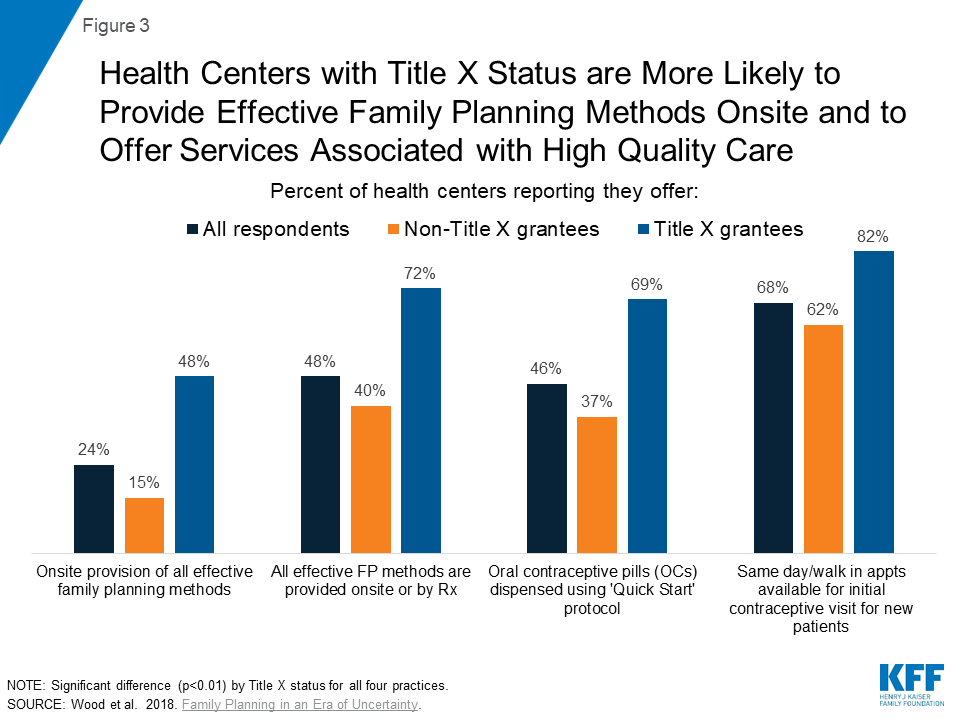
A Kaiser Family Foundation and George Washington University study is illustrative of the difference that having Title X support makes in terms of the quality and range of family planning services offered by Federally Qualified Health Centers (FQHCs) (Figure 3).13 Because they adhere to the QFP guidelines, Title X-funded sites consistently offer patients a larger range of onsite contraceptive methods, including natural family planning instruction and emergency contraception. Title X-funded health center sites offer all seven of the most effective methods onsite at three times the rate of sites not receiving Title X funding (48% to 15% respectively). Title X-funded sites also consistently show greater incorporation of evidence-based best practice methods, such as use of the “quick start” method for oral contraception that ensures that women who seek it have rapid access to effective contraceptive services.
Some stand-alone family planning clinics, particularly in rural communities, may not be in close proximity to other primary health providers, and therefore may not qualify for funding. Excluding family planning clinics because they do not offer comprehensive primary care or are not near a primary care provider could make it more difficult for women, particularly in rural areas, to access the full range of family planning services that are available under the current program. Specialized family planning clinics have been shown to provide a wider range of contraceptive methods and higher quality family planning care than clinics providing comprehensive care, such as community health centers.14
Eliminating the requirement that Title X sites offer women the full range of family planning services would restrict the number of sites that offer low-income women comprehensive contraceptive and family planning services. The proposed regulation would no longer require that sites follow the QFP guidelines to provide “services that are consistent with current recognized national standards of care, including QFP, related to family planning, reproductive health, and general preventive health measures.”15 These requirements were added to Title X in 2014 following an exhaustive process by OPA and CDC to improve the standards of family planning services in clinics and other sites. By dropping this requirement, access to the full range of contraceptive services and other quality family planning services could be limited for low-income women.
The new regulation would channel new federal family planning funds to faith-based and other organizations that do not provide contraceptive services. The vast majority of women who seek family planning care at Title X sites use and seek contraceptive services. Women seeking contraceptives could find themselves at a federally funded faith-based provider that only offers natural family planning education and does not provide them with a referral or option for securing effective contraceptive methods including IUDs, implants, or oral contraceptives. While some women may seek to use natural family planning or fertility awareness methods to plan or avoid pregnancy, these methods are among the least effective and least commonly used methods to prevent unintended pregnancies.16 The proposed regulation permits and encourages the participation of these single service providers, so long as they are part of a Title X project that includes comprehensive services, and does not require that other contraceptive services be offered onsite.
Many elements of this regulation would be administratively burdensome for grantees and subrecipients. The program in its current state already has significant reporting requirements and oversight, and this proposed rule would go far beyond current practice. Subrecipients do not typically oversee the policies and referral practices of the organizations that they refer to for other services. This would require clinics to track services among referral networks they are not funded to provide. The documentation and reporting requirements for minors may also violate some state confidentiality laws and could provide a disincentive for minors and teens to seek services.
Looking Forward
If fully implemented, the proposed changes to Title X could have major repercussions for low-income women across the country that rely on Title X sites for their family planning care. As the regulations are finalized and likely litigated, the future of the Title X program and access to quality family planning services for millions of low-income women hangs in the balance.
Under the proposed regulations, all Planned Parenthood centers would be disqualified and countless other providers that currently participate in Title X could decide that limits on counseling and referral for abortion violate the clinical standards of care and informed consent. These actions could shrink the network of providers that offer low-income women comprehensive family planning services using federal support. In addition to the abortion-specific provisions, there are other notable changes in the proposed regulations that are administratively burdensome, weaken the clinical standards of family planning care offered by Title X providers, and redefine programmatic eligibility standards to promote Administration priorities. For low-income women, clinic-based providers are important sources of family planning services. One in three low-income women reported that they obtained birth control from a clinic-based provider such as Planned Parenthood or another health center or public health clinic.17 In 2016, 64% of clients seen at Title X clinics had family incomes at or below the poverty level, 37% were covered by Medicaid or another public program, and nearly half (43%) were uninsured.18
As the ACA coverage expansions are weakened and more women become uninsured, the robust network of providers that the Title X program now supports will become even more essential for women. The proposed regulation could vastly restrict the size and scope of this network and place considerable burdens on the providers who opt to stay in the program, but who may not be able to keep up with demand for care. In the 2017 Kaiser Family Foundation and George Washington University survey, many community health centers reported a limited ability to take on new patients given current staffing and space constraints, suggesting that these health centers may not have the capacity to fill the void if Planned Parenthood were excluded nationwide as a Title X provider. At the same time that the need for affordable family planning services is likely to grow, many women would be left with far fewer options to obtain affordable, comprehensive, and high quality family planning care.
Appendix
| Appendix 1: Federal Rules for Title X Projects on Abortion Services and Activities | |||
| 1988(only in effect for one month due to litigation and subsequent change of Administration) | 1993-Present | 2018 Proposed Regulations | |
| Counseling | Prohibited. | Nondirective counseling required for pregnant women addressing: prenatal care & delivery, infant care, foster care, adoption, pregnancy termination. | The language of the proposed regulation: “A Title X project may not provide, promote, refer for, support, or present abortion as a method of family planning.” The non-binding preamble to the proposed regulation states: “A doctor, though not required to do so, would be permitted to provide nondirective counseling on abortion.” |
| Referral | Prohibited. | Must offer referral for abortion if asked but cannot:
| Prohibited, unless a woman has already decided to have an abortion, and requests a referral. A medical doctor may provide a list of comprehensive health service providers, some but not all of which also provide abortion. |
| Requirements For How Abortion Activities Supported By Non-Title X Funds Must Be Handled | |||
| Financial | Separate accounting records. | Separate accounting records. | Separate accounting records, electronic and paper health records. |
| Facility | Separate treatment, consultation, waiting rooms. | Shared waiting room permissible as long as costs are properly pro-rated. | Separate treatment, consultation, examination, and waiting rooms, office entrances and exits, workstations, signs, phone numbers, email addresses, educational services, and websites. |
| Staff | Separate staff. | Shared staff permissible as long as all abortion related activities are financed separately from the Title X project. | Separate staff. |
| Prohibition on activities that encourage, promote, or advocate for abortion | Lobbying, providing speakers or educators who promote abortion, paying dues to an abortion advocacy group, legal action to make abortion available, developing or disseminating materials advocating for abortion. | No prohibition on these activities. | Lobbying, providing speakers or educators, attending events or conferences during which the grantee or subrecipient engages in lobbying, paying dues to an abortion advocacy group, legal action, developing or disseminating materials. |
| SOURCE: Kaiser Family Foundation analysis of federal regulations. | |||
Endnotes
- Title X of the Public Health Service Act, 42 U.S.C. 300, et seq. ↩︎
- National Family Planning & Reproductive Health Association v. Alex M. Azar II ↩︎
- Planned Parenthood of Wisconsin, Inc. v. Alex M. Azar II ↩︎
- Zolna MR and Frost JJ. (2016). Publicly Funded Family Planning Clinics in 2015: Patterns and Trends in Service Delivery Practices and Protocols. Guttmacher Institute. ↩︎
- Frost J., Frohwirth L, Blades N., Zolna M., Douglas-Hall, A., Bearak, J. Publicly Funded Contraceptive Services at U.S. Clinics, 2015. Guttmacher Institute. April 2017. ↩︎
- White K, et al. (2015). The Impact of Reproductive Health Legislation on Family Planning Clinic Services in Texas. American Journal of Public Health. ↩︎
- Stevenson AJ, et al. The Effect of Removal of Planned Parenthood from the Texas Women’s Health Program. The New England Journal of Medicine 2016;374:853-60. ↩︎
- Redden M. Healthcare without Planned Parenthood: Wisconsin and Texas Point to a Dark Future. The Guardian. January 17, 2017. ↩︎
- Health Management Associates. Challenges to Underserved Women’s Access to Family Planning Services in Wisconsin 2016. January 2017. ↩︎
- Institute of Medicine (IOM). (2001). Crossing the Quality Chasm: A New Health System for the 21st Century. ↩︎
- Jones RK and Jerman J. Abortion Incidence and Service Availability In the United States, 2014. Guttmacher Institute. ↩︎
- Wickline v. State of California (1986). ↩︎
- Wood et al. Kaiser Family Foundation and George Washington University. (2018). Community Health Centers and Family Planning in an Era of Policy Uncertainty. ↩︎
- Zolna MR and Frost JJ. (2016). Publicly Funded Family Planning Clinics in 2015: Patterns and Trends in Service Delivery Practices and Protocols. Guttmacher Institute. ↩︎
- https://www.hhs.gov/opa/sites/default/files/FY-17-Title-X-FOA-New-Competitions.pdf ↩︎
- Kaiser Family Foundation. (2018). Natural Family Planning as a Means of Preventing Pregnancy. ↩︎
- Kaiser Family Foundation. (2018). Women’s Sexual and Reproductive Health Services: Key Findings from the 2017 Kaiser Women’s Health Survey. ↩︎
- Fowler CI, Gable J, Wang J, & Lasater B. (2017). Family Planning Annual Report: 2016 national summary. RTI International. ↩︎