Medicaid
Medicaid work requirements
The Medical Frailty Exemption from Medicaid Work Requirements: Key Takeaways from the CMS Interim Final Rule
This brief describes new guidance and potential challenges states will face in operationalizing the medical frailty exemption when implementing Medicaid work requirements. Forty-four states must implement work requirements starting January 1, 2027, or sooner at state option.
new and noteworthy
Medicaid Program Integrity: Tracking State-Specific and Nationwide Federal Action
This page tracks emerging developments in the federal government’s approach to Medicaid program integrity, along with the implications of those actions for different states.
Spending on Medicaid State Directed Payments Before New Limits
Forty states and DC currently receive $93 billion in annual federal Medicaid spending through state directed payments (SDPs) and may be at risk due to forthcoming limits on these payments, according to new KFF estimates.
understanding medicaid
Medicaid Financing
Medicaid represents $1 out of every $5 spent on health care in the U.S. and is the major source of financing for states to provide health coverage and long-term care. This brief examines key questions about Medicaid financing and how it works.
Medicaid Program Integrity
This brief explains what is known about improper payments and fraud and abuse in Medicaid and describes ongoing state and federal actions to address program integrity.
Medicaid and Provider Taxes
All states except Alaska cover some state Medicaid costs with taxes on health care providers. This brief uses data from KFF’s 2024-2025 survey of Medicaid directors to describe current practices and the federal rules governing them.
Medicaid and Hospitals
Absorbing reductions in Medicaid spending could be challenging for hospitals, particularly for those that are financially vulnerable. This brief provides data on the reach of Medicaid across hospitals, patients, and charity care.
Medicaid Home Care
This issue brief provides an overview of what Medicaid home care (also known as “home- and community-based services”) is, who is covered, and what services were available in 2025.
Dual Eligibles
-
A Profile of Dual-Eligible Individuals
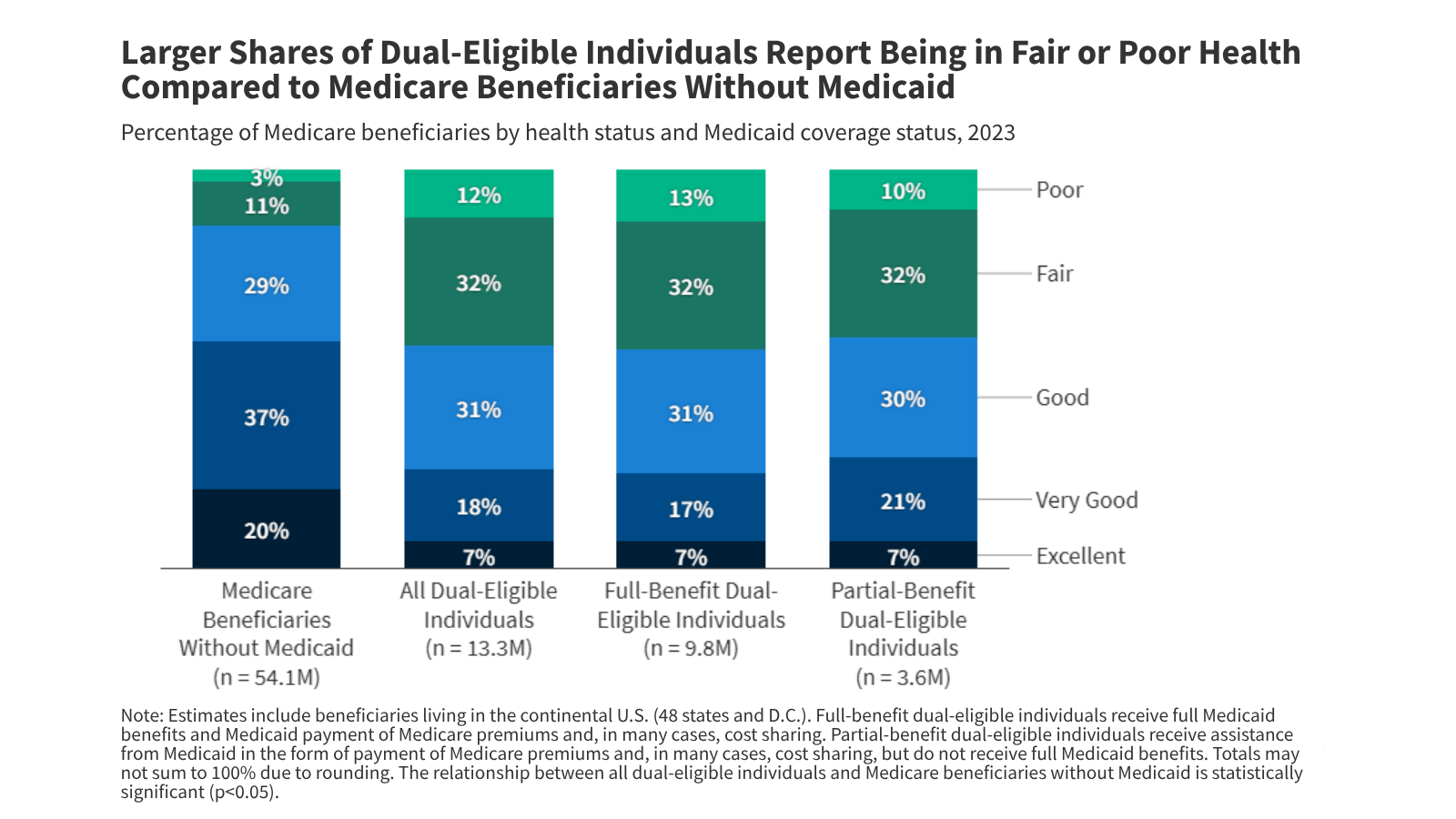
About 12 million people are enrolled in both Medicare and Medicaid. These dual eligible individuals are a diverse group, but are more likely than other Medicare beneficiaries to report fair or poor health and to have lower incomes and more chronic conditions.
-
5 Key Facts About Spending and Enrollment for People with Medicare and Medicaid
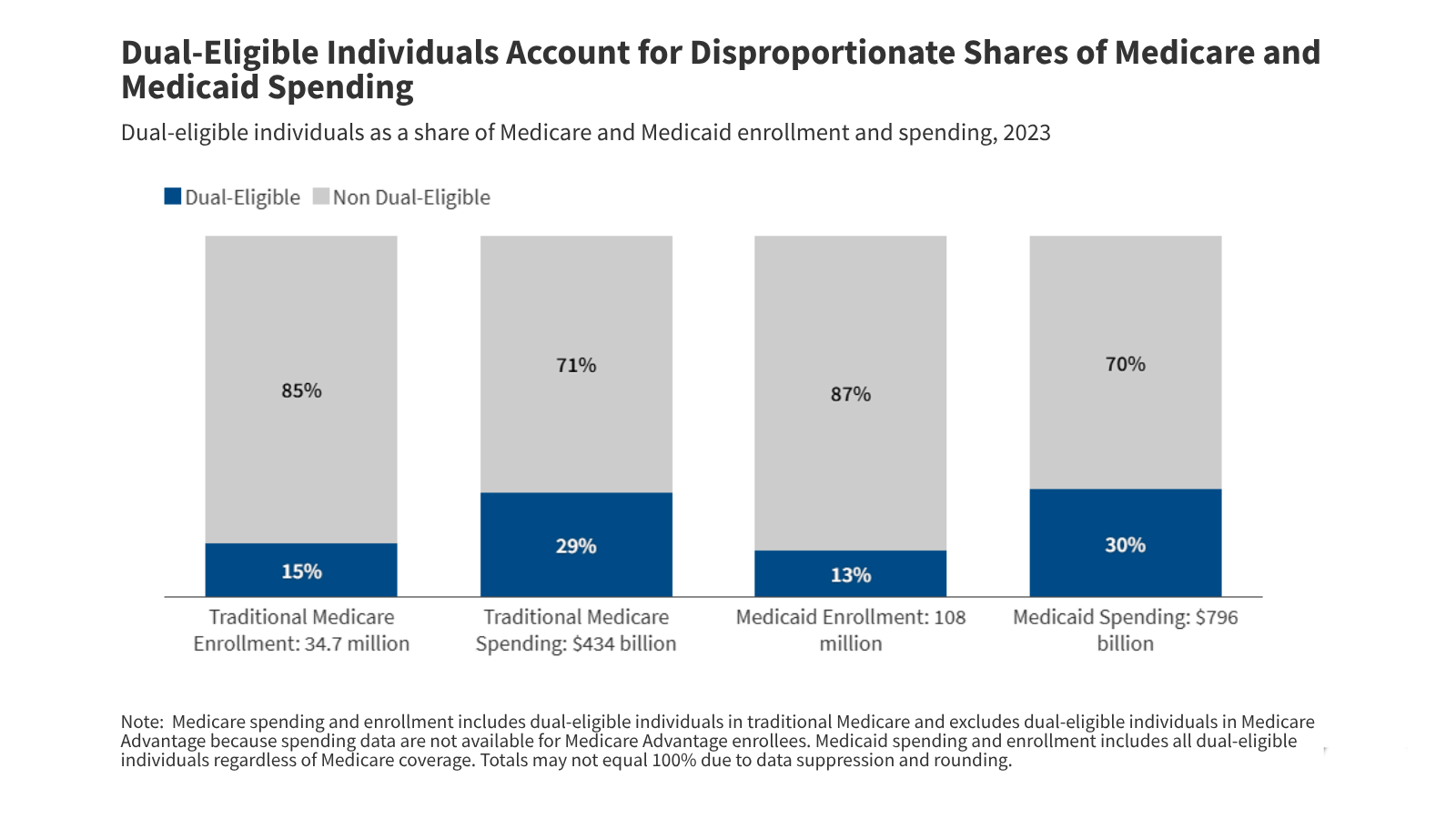
Dual-eligible individuals make up a disproportionately large share of Medicare and Medicaid spending relative to their enrollment, in part reflecting higher rates of chronic illness.
-
State Health Facts: Enrollment and Spending for Dual-Eligible Individuals
This data collection draws on Medicare and Medicaid administrative data to present national and state-level information on people covered by both Medicare and Medicaid.
Latest News
-

AI Is Being Used to Boost Medicaid Enrollment, but Not Without Concerns
-

People With Disabilities Fear Service Cuts as Trump’s DOJ Questions Legal Protections
-

Kennedy, Oz Contend Fraud Crackdown, Not Skyrocketing Prices, Led Millions To Leave Obamacare
-

Medicaid Insurers’ Contracts on the Line in Tight Governor’s Race

