Higher and Faster Growing Spending Per Medicare Advantage Enrollee Adds to Medicare’s Solvency and Affordability Challenges
Issue Brief
The number of people enrolled in Medicare has increased steadily in recent years, and along with it, Medicare spending. In particular, enrollment in Medicare Advantage, the private plan alternative to traditional Medicare, has more than doubled over the last decade. Notably, Medicare spending is higher and growing faster per person for beneficiaries in Medicare Advantage than in traditional Medicare. As enrollment in Medicare Advantage continues to grow, these trends have important implications for total Medicare spending, and costs incurred by beneficiaries. In its 2022 budget, the Biden Administration expressed support for reforming payments to private plans as part of efforts to extend the solvency of the Medicare Hospital Insurance (HI) Trust Fund and improve affordability for beneficiaries.
This analysis examines Medicare spending per person for beneficiaries in Medicare Advantage, relative to traditional Medicare. We build on prior work published by the Medicare Payment Advisory Commission (MedPAC) and the Centers for Medicare and Medicaid Services (CMS) Office of the Actuary (OACT) to provide estimates of the amount Medicare would have spent for Medicare Advantage enrollees had they been covered under traditional Medicare in 2019 (the most recent year for which data are available). We use publicly available data from CMS that includes spending for people who were enrolled in both Part A and Part B of traditional Medicare, by category of service, as well as information on average risk scores and enrollment by county. This allows us to calculate per-person spending for beneficiaries in traditional Medicare on a basis comparable to federal payments per enrollee in Medicare Advantage. We also examine the extent to which the projected growth in Medicare Advantage spending is attributable to the growth in enrollment and the increase in spending per person. We then illustrate potential savings to the Medicare program between 2021 and 2029 under two alternative scenarios where Medicare Advantage spending per person is lower or grows slower than under current projections. (See Methodology for more details on the data and analytic approach.)
Our analysis finds:
- Medicare spending for Medicare Advantage enrollees was $321 higher per person in 2019 than if enrollees had instead been covered by traditional Medicare. The Medicare Advantage spending amount includes the cost of extra benefits, funded by rebates, not available to traditional Medicare beneficiaries.
- The higher Medicare spending per Medicare Advantage enrollee, compared to spending for similar beneficiaries under traditional Medicare, contributed an estimated $7 billion in additional spending in 2019.
- Growth in Medicare Advantage enrollment explains half of the projected increase in total Medicare Advantage spending between 2021 and 2029 and half is attributable to growth in Medicare payments per Medicare Advantage enrollee, after accounting for inflation.
- If spending per Medicare Advantage enrollee was 2 percent less each year than projected by the Medicare actuaries, similar to the projected impact of a recommendation made by MedPAC, total Medicare spending would be $82 billion lower between 2021 and 2029. If instead Medicare payments per Medicare Advantage enrollee grew at the same rate as is projected for spending per person in traditional Medicare (4.4% vs 5.3%), total Medicare spending would be $183 billion lower between 2021 and 2029.
Background on Payments to Medicare Advantage Plans
Medicare beneficiaries have the option to receive their Medicare benefits through either the traditional Medicare program or by enrolling in a private health plan, such as an HMO or PPO, that contracts with Medicare, called Medicare Advantage. Medicare pays Medicare Advantage plans a set amount for each enrollee. The payment is determined through an annual process in which plans submit “bids” for how much they estimate it will cost to provide benefits covered under Medicare Parts A and B for an average beneficiary. The bids submitted by each plan are compared to a benchmark, which is an amount based on a set percentage of the projected average spending for beneficiaries in traditional Medicare in the same county. The benchmarks range from 95 percent in high spending counties to 115 percent in low spending counties. The benchmarks are subject to caps, meaning they cannot exceed the benchmarks that were in place before the Affordable Care Act. In addition, the benchmarks are increased by 5 percent for plans that receive at least 4 out of 5 stars under the quality bonus program, and 10 percent in certain “double bonus” counties.
Plans that bid below the benchmark receive a portion of the difference between the bid and the benchmark as a “rebate” (50 percent for plans with 3 or fewer stars, 65 percent for plans with 3.5 or 4 stars, and 70 percent for plans with 5 stars). Rebates must be used to reduce cost sharing, subsidize the standard Part B and/or Part D premium, or pay for supplemental benefits (such as vision, dental, and hearing). A portion of the rebate may also be used for administrative costs or retained as profit. Plans that bid above their benchmark receive the benchmark amount, and enrollees pay an additional premium equal to the difference between the bid and benchmark. The payments to plans are risk adjusted, based on the health status and other characteristics of enrollees, including age, sex, and Medicaid enrollment. Medicare payments are higher for plans with higher average risk scores because their enrollees are expected to incur higher costs.
While traditional Medicare spending is used to establish benchmarks, actual payments to Medicare Advantage plans can be higher or lower than spending for comparable beneficiaries in traditional Medicare. Changes in the Affordable Care Act initially reduced Medicare Advantage benchmarks. However, since 2017, benchmarks have risen on average, which increases the maximum possible payment a plan can receive. When benchmarks increase, plans that bid below the benchmark may be able to retain the same amount of rebate dollars, and thus offer the same level of extra benefits, while increasing their bid for Part A and B services. Alternatively, these plans could bid the same (or even slightly less) and receive higher rebate payments as the difference between the benchmark and bid widens because the benchmark is higher. Either response increases the payment Medicare Advantage plans receive as benchmarks increase. One reason for the recent increase in benchmarks is that more plans are in bonus status, and thus have 5 percent (or 10 percent in double bonus counties) added to their benchmark. In 2021, 81 percent of Medicare Advantage enrollees are in plans that receive a bonus payment. Similarly, rebates increase as star ratings increase, because plans with higher star ratings retain a larger percent of the difference between the benchmark and bid as a rebate.
In addition, risk adjustment can lead to higher payments for Medicare Advantage enrollees than would have been spent in traditional Medicare. This is because risk scores are largely based on diagnoses, and more diagnoses generally increase a beneficiary’s risk score, providing an incentive for diagnoses to be coded more comprehensively for Medicare Advantage enrollees than occurs for traditional Medicare beneficiaries. MedPAC estimates that this more comprehensive coding of diagnoses in Medicare Advantage increased risk scores 9.1 percent relative to traditional Medicare in 2019. There is also some concern that Medicare Advantage plans submit inaccurate diagnoses that increase risk scores and result in overpayments. The Health and Human Services Office of the Inspector General is currently conducting a targeted review of documentation submitted by Medicare Advantage organizations to determine whether diagnoses and associated risk scores comply with federal regulations. And in July, the Department of Justice announced that they were intervening in a False Claims Act lawsuit alleging that Kaiser Permanente had submitted inaccurate diagnoses codes for Medicare Advantage enrollees.
Findings
Spending per person
Medicare spent $321 more per person for Medicare Advantage enrollees than it would have spent for the same beneficiaries had they been covered under traditional Medicare in 2019. After adjusting for differences in health status and the geographic distribution of Medicare Advantage enrollees and traditional Medicare beneficiaries, spending per person for services covered under Parts A and B totaled $11,523 in 2019 for beneficiaries in traditional Medicare. This estimate for traditional Medicare reflects the categories of spending that are covered by Medicare payments to Medicare Advantage plans, and so excludes spending on hospice and payments for graduate medical education but includes administrative expenses. In addition, it adjusts for the impact of more intense coding of diagnoses in Medicare Advantage relative to traditional Medicare, as estimated by MedPAC, which makes Medicare Advantage enrollees look like they are in worse health. (See Methodology for additional discussion.)
In the same year, federal payments to Medicare Advantage plans were $11,844 per enrollee, or $321 more per person than Medicare would have spent if these beneficiaries had instead been covered by traditional Medicare. In other words, Medicare Advantage payments were about 103 percent of spending for comparable traditional Medicare beneficiaries. The higher spending occurred despite changes in law made by the Affordable Care Act that reduced payments to plans over time (which MedPAC estimated at 114 percent of traditional Medicare beneficiary spending in 2009).
As described above, Medicare payments per Medicare Advantage enrollee include two components: bid-based expenditures, which reflect the plan’s expected costs for providing services covered under Medicare Parts A and B (adjusted for health risk), and rebates, which pay for the cost of benefits not available to traditional Medicare beneficiaries, including reduced cost sharing, subsidized Part B and Part D premiums, and coverage of additional benefits, such as vision, dental and hearing. In 2019, the bid-based portion of the Medicare Advantage payment was $10,848 and the rebate portion was $996.
Higher Medicare payments per Medicare Advantage enrollee increased total Medicare spending by an estimated $7 billion in 2019. Across the approximately 22 million people enrolled in Medicare Advantage in 2019, higher spending of $321 per person led to about $7 billion in additional spending in that year. That is equal to about 3 percent of all Medicare Advantage spending in 2019.
Projected growth in Medicare Advantage spending
Growth in Medicare Advantage enrollment explains half of the projected growth in Medicare Advantage spending between 2021 and 2029, after adjusting for inflation. Between 2021 and 2029, federal spending on payments to Medicare Advantage plans is projected to increase by $316 billion, from $348 billion to $664 billion. After accounting for inflation (which represents $108 billion of this increase), the remaining $208 billion is explained by growth in payments per person ($105 billion, or 50 percent) and growth in enrollment ($104 billion, or 50 percent) (Figure 1).
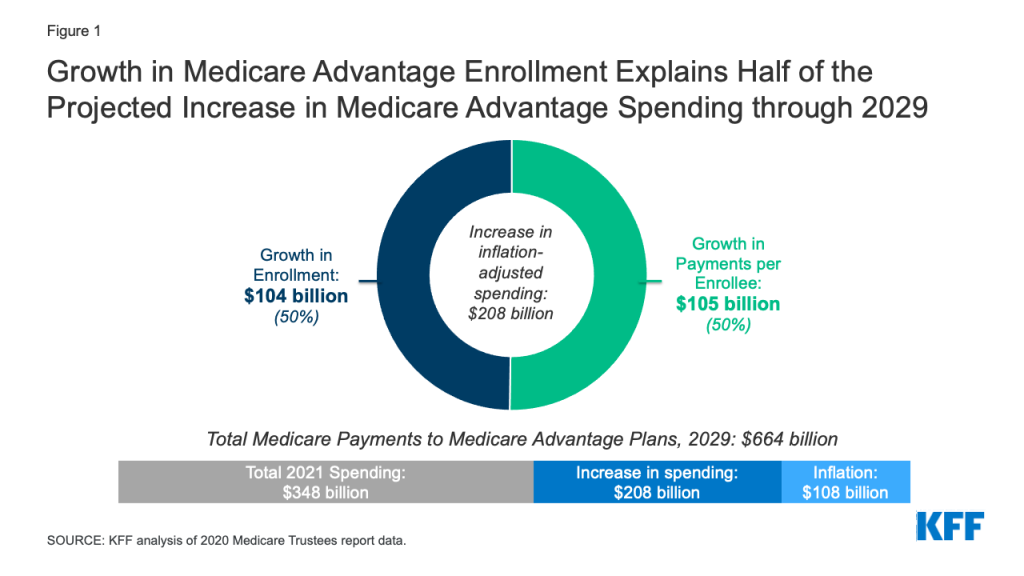
Notably, the rebate portion of Medicare Advantage payments, which must be used to cover the cost of additional benefits not available to traditional Medicare beneficiaries, is projected to grow between 2021 and 2029. Rebates account for about 10 percent of Medicare Advantage payments in 2021 ($35 billion of $348 billion) and are projected to rise to 12 percent ($80 billion of $664 billion) in 2029.
Medicare spending is projected to grow faster for Medicare Advantage enrollees than traditional Medicare beneficiaries. Spending per person in Medicare Advantage is projected to grow 5.3 percent a year on average between 2021 and 2029, an amount which is similar across plan types (based on KFF analysis of data from the 2020 Medicare Trustees Report). The projected growth in Medicare Advantage spending per person is somewhat higher than the 4.4 percent average annual growth projected for beneficiaries in traditional Medicare (see Methodology for details on data and methods).
According to the Medicare actuaries, the higher projected growth in Medicare payments per Medicare Advantage enrollee are in part explained by faster projected growth in the rebate portion of the payment. Rebates are projected to grow nearly 8 percent a year on average, which the actuaries attribute to “assumed increases in quality bonus payments and increases in benchmarks.”
It is also possible that the faster expected increase in spending per person in Medicare Advantage compared to traditional Medicare through 2029 is due in part to an assumption that sicker and higher cost beneficiaries, such as those dually eligible for Medicare and Medicaid, will enroll in Medicare Advantage at a higher rate than in traditional Medicare. For example, the number of Medicare Advantage enrollees in special needs plans (SNPs), which included just over half of all dually eligible beneficiaries in Medicare Advantage in 2019, is expected to increase slightly by 2029. However, the change is relatively small, and even if it represents only half of the total increase in Medicare Advantage enrollment by dually eligible beneficiaries, it suggests the projected increase in spending per Medicare Advantage enrollee is being driven by other factors, such as Medicare Advantage payment methodology. Additionally, starting in 2021, all Medicare beneficiaries with end-stage renal disease (ESRD) are eligible to enroll in a Medicare Advantage plan. Though beneficiaries with ESRD have substantially higher costs than the average Medicare beneficiary, they represent less than 1 percent of all Medicare beneficiaries, and so increased enrollment by beneficiaries with ESRD is likely to explain a relatively small portion of the growth in per-person spending in Medicare Advantage.
Alternative projections for Medicare Advantage spending
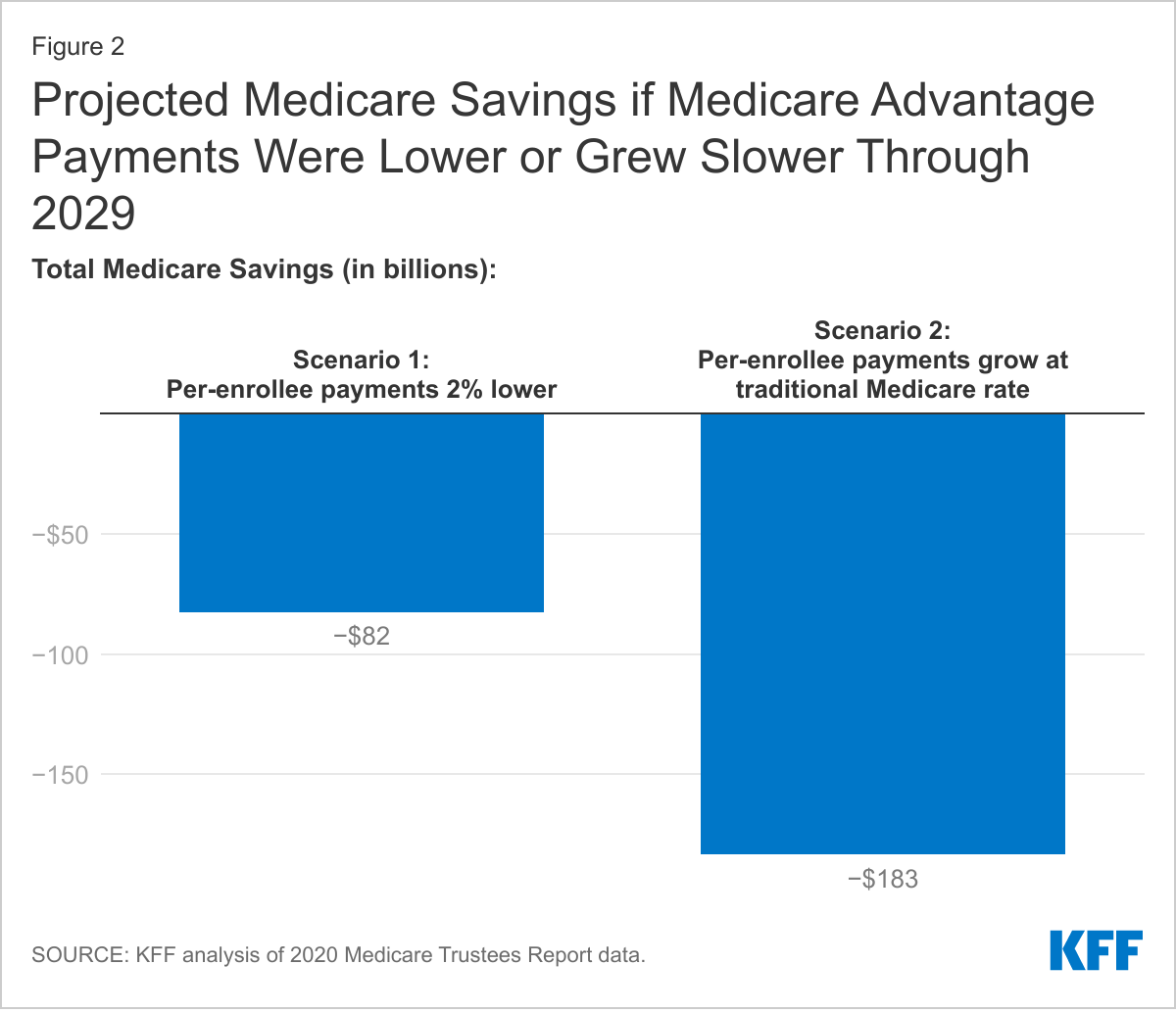
If Medicare Advantage spending per person was 2 percent less a year than projected, similar to the simulated effect of recommended payment changes from MedPAC, total Medicare spending would be $82 billion lower through 2029. MedPAC has proposed changes to how Medicare Advantage benchmarks are calculated and estimate these changes would result in a 2 percent reduction in Medicare Advantage payments in a single year. Applying this payment reduction to the projected Medicare Advantage payments per enrollee in each year between 2022 and 2029, total Medicare Advantage spending would be $82 billion lower through 2029 (Figure 2). The decrease is approximately 1 percent of total Medicare benefit spending over these years (and 2 percent of Medicare Advantage spending).
Even with the reduction in aggregate spending under this scenario where Medicare Advantage payments are reduced by 2 percent per year, projected Medicare spending per Medicare Advantage enrollee would still be higher and grow faster than projected spending per person in traditional Medicare. MedPAC expects implementing changes to the benchmark policy that result in a 2 percent reduction in payments in a given year would have only a modest effect on access to plans with lower cost sharing and reduced Part B and D premiums. For example, in their simulations, the vast majority (over 95 percent) of Medicare beneficiaries would continue to have access to Medicare Advantage plans that offer reduced cost sharing and Part B and/or D premium reductions. The number of plan sponsors and plan choices would vary across geographic areas, as they do under current policy, but would be somewhat reduced. In the quartile of counties with the lowest traditional Medicare spending per person, MedPAC estimates an average of 5 plan sponsors would offer 12 different plans (compared to 6 plans sponsors who offered 22 different plans in 2020). In the quartile of counties with the highest spending per person in traditional Medicare, an average of 8 plan sponsors would offer 22 different Medicare Advantage plans (compared to the same number of sponsors who offered 27 plans in 2020).
Under an alternative, illustrative scenario, where Medicare Advantage spending per person grew at the same rate as is projected for traditional Medicare, spending would be $183 billion lower between 2021 and 2029. For this scenario, we calculated the difference in projected Medicare spending if Medicare payments per person to Medicare Advantage plans grew at the same rate as spending per person in traditional Medicare (4.4 percent) between 2021 and 2029, rather than the higher 5.3 percent growth rate projection. While this approach is not directly pegged to a specific policy proposal, it illustrates the potential for savings, of, for example, a cap on the growth in total Medicare Advantage payments per enrollee. To adjust to such a cap, plans could find additional efficiencies in the coverage of Part A and B services, reduce supplemental benefits, restrict the future growth in supplemental benefits, lower administrative costs, reduce profits, or some combination of each. Limiting the growth in Medicare payment per Medicare Advantage enrollee directly or indirectly could also be achieved through other payment reforms.
Under the scenario where per-person spending growth in Medicare Advantage and traditional Medicare is equivalent, total Medicare Advantage spending over 2021 to 2029 would be $183 billion lower (Figure 2). For context, the savings under this scenario represents 4 percent of projected Medicare Advantage spending over this time period (and 2 percent of total Medicare benefit spending). That compares to an expected reduction in Medicare Advantage spending of 8.9 percent between 2010 and 2019 due to changes in the Affordable Care Act (based on CBO’s estimate of the health care law and its March 2009 baseline). While spending per person would grow at the same rate in both Medicare Advantage and traditional Medicare under this scenario, payments per Medicare Advantage enrollee would be higher than spending per beneficiary in traditional Medicare because of higher projected spending per person in Medicare Advantage in 2021.
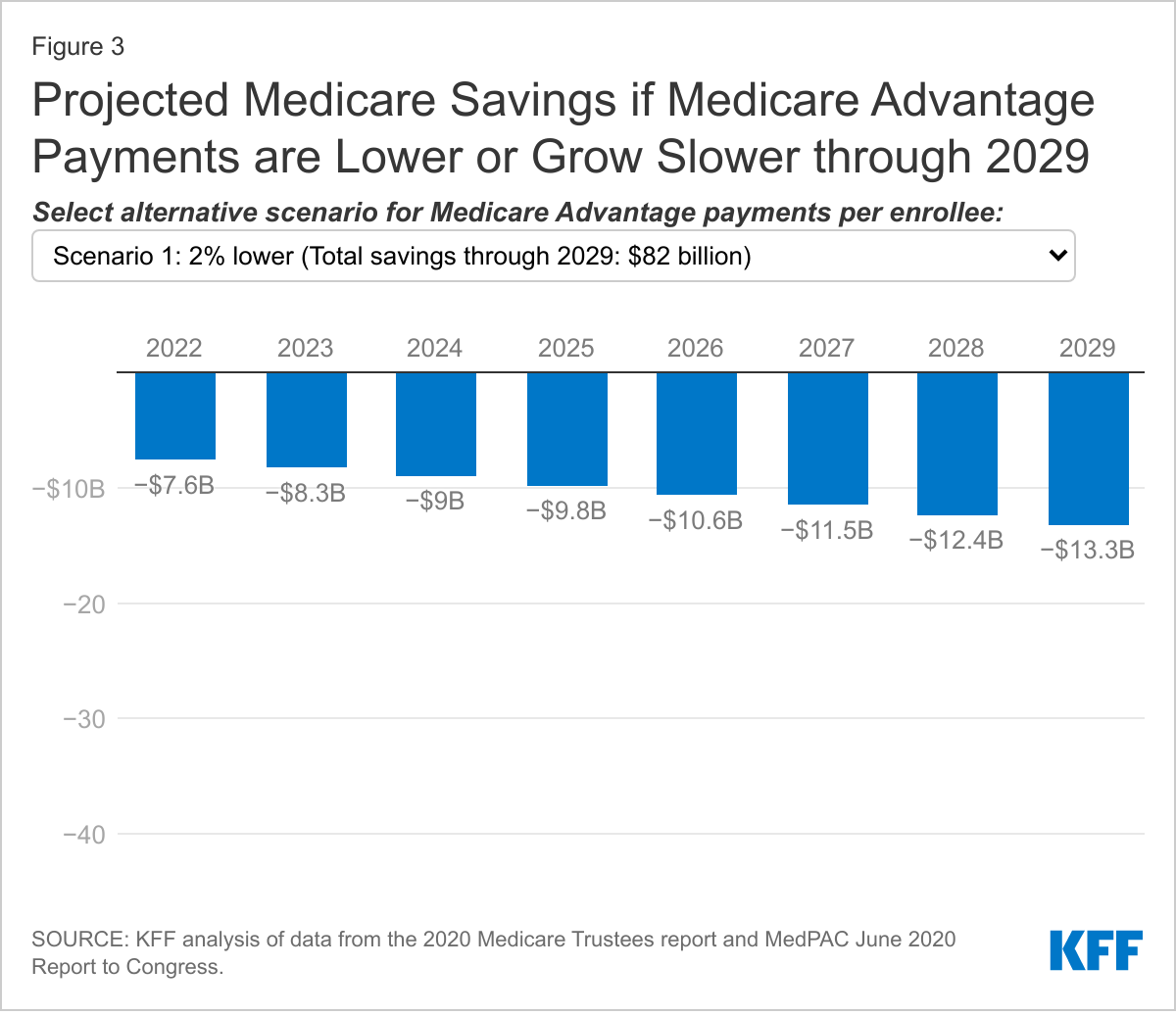
Comparing the two alternative scenarios, the reduction in Medicare Advantage spending is similar in the initial years of the time period. However, the Medicare savings accrue more rapidly under the scenario where growth in payments per Medicare Advantage enrollee is equal to the rate of growth in spending per person in traditional Medicare. This is because savings from lower growth compound over time. (Toggle between the two scenarios to see the year-by-year savings under each scenario in Figure 3).
These estimates assume no changes to projected enrollment, which may occur if supplemental benefits, cost sharing, or other features of Medicare Advantage plans change in response to lower payments from the federal government. However, while it is not possible to know exactly how plans will respond to lower payments, previous analyses of past payment changes demonstrate that plans have found savings elsewhere in order to maintain rebate dollars to fund supplemental benefits that may appeal to enrollees. For example, MedPAC examined the response of Medicare Advantage plans that lost bonus status between 2018 and 2019 and found that these plans reduced their profits and administrative costs, and had lower growth in their projected Part A and B costs compared to other plans. This allowed the plans to continue to provide similar levels of supplemental benefits. Further, despite predictions by CBO, Medicare actuaries, and others that enrollment in Medicare Advantage would fall following the reductions in payment to Medicare Advantage plans enacted as part of the Affordable Care Act, enrollment never declined and has instead risen rapidly. Plans offer more generous supplemental benefits in 2021 than at any other point in the program’s history and Medicare Advantage markets are robust, with the average Medicare beneficiary having more than 30 Medicare Advantage plans to choose from in 2021.
Conclusion
Historically, one goal of the Medicare Advantage program was to leverage the efficiencies of managed care to reduce Medicare spending. However, the program has never generated savings relative to traditional Medicare. In fact, the opposite is true. As a result, Medicare Advantage plans have been able to offer an increasingly robust set of extra benefits not available to beneficiaries in traditional Medicare. The annual cost of the rebate dollars used to pay for the extra benefits – $1,680 per Medicare Advantage enrollee for non-employer, non-SNP plans in 2021 – more than offset any savings that Medicare Advantage plans generate by bidding below the benchmark set by CMS for covering Part A and B services. The extra benefits improve coverage for beneficiaries who choose Medicare Advantage plans and have likely contributed to the substantial increase in Medicare Advantage enrollment. But the higher payments have also led to higher Medicare spending than would have occurred under traditional Medicare and higher Medicare Part B premiums paid by all beneficiaries, including those in traditional Medicare.
Our analysis finds that Medicare Advantage payments per enrollee in 2019 were approximately 103 percent of spending per person for comparable beneficiaries covered by traditional Medicare, consistent with estimates based on data submitted by private plans as part of the bidding process and concurrent projections by CMS of future spending in traditional Medicare. MedPAC’s most recent analysis of the relationship between Medicare Advantage payments and spending in traditional Medicare suggests that the difference has widened, with 2021 payments per Medicare Advantage enrollee estimated to total 104 percent of spending in traditional Medicare. That trend is in part attributed to the rise in the rebate component of Medicare Advantage payments, which increased 14 percent between 2020 and 2021. While part of the increase in rebates stems from a decrease in how much private plans bid to provide coverage of Part A and B services, other features of the Medicare Advantage payment methodology, including the quality bonus program payments and benchmark policy contribute to both the recent and projected growth in rebates, and in turn, total Medicare Advantage spending. For example, under the quality bonus program, payments from the federal government to Medicare Advantage plans will total $11.6 billion in 2021, at least a portion of which was paid as the rebate.
MedPAC recently recommended changes to how plan payments are calculated, observing that because most plans currently bid well below the cost of providing Part A and B services in traditional Medicare, there is an opportunity for the Medicare program to share in these efficiencies. Their simulations indicate that a 2 percent reduction in payments would not significantly affect access to private plans or supplemental benefits. A reduction in Medicare Advantage payments consistent with the simulated effect of MedPAC’s recommendations, would result in Medicare program payments per enrollee that would remain higher and still grow faster than spending under traditional Medicare. Alternatively, bringing Medicare Advantage spending growth in line with projected growth in traditional Medicare would achieve more than twice as much savings. Under that scenario, the absolute level of payments per enrollee to private plans would still be higher than spending per person for beneficiaries in traditional Medicare. Reduced federal payments could mean Medicare Advantage enrollees see fewer extra benefits and higher cost sharing and premiums compared to today (but still lower costs than compared to traditional Medicare without supplemental coverage), but plans could also reduce profits or administrative costs to make up the difference. Further, savings of this magnitude would be less than half of those included in the Affordable Care Act, which were followed by a period of robust Medicare Advantage growth.
Over the next decade, Medicare Advantage enrollment is expected to continue to grow. As more Medicare beneficiaries enroll in private plans, differences in Medicare payments across Medicare Advantage and traditional Medicare will lead to even higher Medicare spending, and more generous benefits for beneficiaries in Medicare Advantage than traditional Medicare. That higher spending increases Part B premiums paid by all Medicare beneficiaries, including those who are not in a Medicare Advantage plan, and contribute to the financing challenges facing the Medicare HI Trust Fund. Further, these projections raise questions of equity between Medicare Advantage and traditional Medicare because the faster growth in spending per Medicare Advantage enrollee, compared to traditional Medicare beneficiaries, is in part due to rising rebates to private plans, which cover the cost of benefits not available to traditional Medicare beneficiaries. Although taking steps to address the fiscal challenges facing Medicare are not front and center in current Medicare policy discussions, policymakers may soon be on the lookout for options to achieve Medicare savings to fund other spending priorities or extend the solvency of the Medicare HI Trust Fund. This analysis suggests that reducing the difference in payments between Medicare Advantage and traditional Medicare would generate savings, with the potential for reductions in extra benefits for Medicare Advantage enrollees.
This work was supported in part by Arnold Ventures. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methodology
Per-person spending
The Medicare Trustees’ report includes data on spending per enrollee in private plans, including the bid component, rebate component, and total amount by plan type and overall, since 2010. We use the 2019 total per enrollee in this analysis.
To calculate what Medicare Advantage enrollees would have spent if they had remained in traditional Medicare we start with total spending for Medicare beneficiaries enrolled in both Part A and Part B reported in the CMS Geographic Variation PUF, excluding hospice. We subtract spending on direct and indirect graduate medical education (estimated using data from CMS FFS Data file). Next, we calculate county-level per-person spending in traditional Medicare for this group. We adjust those estimates to account for the health status of Medicare Advantage enrollees compared to traditional Medicare beneficiaries in the same county, using the Geographic Variation PUF data, CMS Plan Payment Data and MedPAC estimates of unadjusted coding intensity. Our estimate of the national average per person spending in traditional Medicare is then calculated as the Medicare Advantage enrollment-weighted county average per person spending and administrative expenses are added. Each step is described in more detail below.
Note, we are unable to compare projected Medicare payments per Medicare Advantage enrollee to future spending per person in traditional Medicare for comparable beneficiaries. This is because detailed information about key inputs into our calculation are not available, specifically: expected health status and risk score information for Medicare Advantage enrollees and traditional Medicare beneficiaries, the geographic distribution of Medicare Advantage enrollees, and county level spending projections
Total Part A and Part B Spending: Part A spending is the sum of spending in the following service categories: Inpatient, PAC: SNF, PAC: IRF, and PAC: LTCH. Part B spending is the sum of Outpatient, Ambulatory Surgical Center, E&M, Procedures, Tests, Imaging, DME, Outpatient Dialysis Facility, FQHC/RHC, Ambulance, Part B Drugs, Other Services, and PAC: HH spending. In addition, Total Population Based Payment Reduction Costs are added to total spending. This category includes payments made to ACOs and other population-based-payment program payments. Note, we do not exclude disproportionate share hospital (DSH) program spending because the funding formula for Medicare Advantage plans includes an amount to cover these payments and may influence the prices negotiated between private plans and hospitals.
GME and IME: To estimate the amount of GME and IME spending to subtract, the GME and IME Part A spending shares in the FFS data are applied to Part A spending in the Geographic Variation file.
County Per Person Spending: The per person spending for traditional Medicare beneficiaries is calculated by dividing the sum of total spending, as described above, by the number of beneficiaries enrolled in Part A and Part B in the county.
Health Status and Unadjusted Coding Intensity: CMS provides the average risk score by county and plan type through 2017. We use these data and the Medicare Advantage enrollment data to calculate an enrollment weighted county average risk score for 2017. We then calculate the ratio between the Medicare Advantage risk scores and the average HCC score for traditional Medicare beneficiaries in each county. Since plan payment data are not available for 2019, we take the 2017 risk ratio and increase by the growth in the ratio of Medicare Advantage to traditional Medicare risk scores reported by MedPAC (2.0 percentage points between 2019 and 2017). To account for unadjusted coding intensity in 2017, we reduce the risk ratios by the Medicare Advantage coding impact on payment reported by MedPAC (1.4 percentage points in 2017, 3.2 percentage points in 2019) (Figure 12-7). There is some disagreement about the level of upcoding in Medicare Advantage. By using MedPAC’s estimates, we incorporate the more conservative estimates of coding intensity. For comparison, a recent brief by the Center for a Responsible Federal Budget suggests that coding intensity increased risk scores by 15.4 percent in 2017, more than twice MedPAC’s estimate (which was 7.1 percent in 2017, including the statutory adjustment of 5.7 percent in that year, which is reflected in the Medicare Advantage payment data in the Trustees report). The adjusted risk score ratio and the county per person spending estimate are then multiplied to get the county per-person spending for traditional Medicare beneficiaries.
National Average Per Person Spending: The contribution of each county to the national average is equal to its share of total Medicare Advantage enrollment in the analysis sample. The county per person spending amounts are multiplied by their county’s respective weight and summed. Note, we do not have complete information for counties with fewer than 11 traditional Medicare beneficiaries or fewer than 11 Medicare Advantage enrollees, and so these counties are excluded in our calculations. We also exclude counties where any category of spending is not reported due to too few beneficiaries contributing to that category of spending in the county.
Administrative Expenses: Private plans use payments received by Medicare to cover their administrative expenses, as well as the cost of Part A and B services and supplemental benefits. The data used to calculate spending among traditional Medicare beneficiaries does not include administrative expenses. We account for this by assuming that administrative expenses for the subset of beneficiaries enrolled in both Part A and Part B of traditional Medicare was the same share of Part A and B spending as it was for the full population of beneficiaries enrolled in either Part A or Part B, or 2.8 percent in 2019.
Decomposing projected growth in Medicare Advantage spending
To determine the drivers of Medicare Advantage spending growth, we first converted the Medicare actuaries’ projections of Medicare Advantage spending to 2021 dollars using the gross domestic product implicit price deflator. We then decomposed the change in annual spending into two components: growth in enrollment and growth in spending per person. Those are defined as follows.
Total spending: TSt = St * EtWhere,
- t is the year
- S is average spending per person, and
- E is total enrollment
The change in total spending in two consecutive years:
TSt – TSt-1 = St * Et – St-1 * Et-1= St-1*(Et – Et-1)+ (St-St-1)*Et-1+ (St – St-1)*(Et – Et-1)
-Where, the first term is the change due to the change in enrollment, the second term is the change due to the change in spending per person, and the third term is the combined effect of enrollment and spending per person. In each year, we allocated the combined effect to either enrollment or spending per person, based on the relative share of the first and second components. To calculate the cumulative impact of each component through 2029, we added the annual estimates together.
To calculate projected growth in spending per person for traditional Medicare we first calculate Part A spending per beneficiary in traditional Medicare by dividing Part A fee-for-service spending from table IV.A3 of the Medicare Trustees Report, less hospice, by the number of Part A enrollees, less part C enrollees, in table V.B3. We then calculated Part B spending per beneficiary in traditional Medicare by dividing Part B fee-for-service spending from table IV.B6 by the number of Part B enrollees, less part C enrollees, in table V.B3. Projected spending per traditional Medicare beneficiary is the sum of these two numbers. We then calculated the average growth rate between 2021 and 2029. Note, these per-person spending amounts are not directly comparable to the amounts we estimated for 2019 using the geographic variation public use file data, because they do not adjust for the distribution of Medicare Advantage enrollment or differences in health status between traditional Medicare beneficiaries and Medicare Advantage enrollees. We calculate growth in payments per Medicare Advantage enrollee using the data in table IV.C3. Data on private health plan enrollment by plan type comes from table IV.C1.
Compared to the Medicare actuaries’ most recent 2020 projections, the Congressional Budget Office (CBO) March 2020 Medicare baseline assumed that approximately 5 million more beneficiaries will be enrolled in Medicare Advantage in 2029. The CBO and OACT have similar estimates of Medicare payments per enrollee. As a result, Medicare Advantage spending is projected to grow more by 2029 under CBO’s baseline than the Medicare actuaries projected in 2020, due to higher enrollment growth. In its most recent July 2021 Medicare baseline, CBO increased its Medicare Advantage enrollment projections, and now expects 8 million more beneficiaries to be enrolled in Medicare Advantage by 2029 than was projected for that year in the 2020 Medicare Trustees Report. CBO did not, however, provide updated estimates of Medicare Advantage spending. Assuming no changes to spending per enrollee, higher enrollment growth would lead to even higher Medicare Advantage spending.