Racial and ethnic disparities in health and health care remain a persistent challenge in the United States. The COVID-19 pandemic’s uneven impact on people of color drew increased attention to inequities in health and health care, which have been documented for decades and reflect longstanding structural and systemic inequities rooted in historical and ongoing racism and discrimination. KFF’s 2023 Survey on Racism, Discrimination, and Health documents ongoing experiences with racism and discrimination, including in health care settings. While inequities in access to and use of health care contribute to disparities in health, inequities across broader social and economic factors that drive health also play a major role. Since taking office, the Trump administration has implemented policies that may erode progress addressing disparities in health and health care, including eliminating equity-related initiatives, reducing federal data collection and reporting, increasing and expanding immigration enforcement, and restricting immigrant access to coverage and health and social supports. Moreover, changes in the 2025 tax and spending law are anticipated to large coverage losses, which will likely exacerbate disparities.
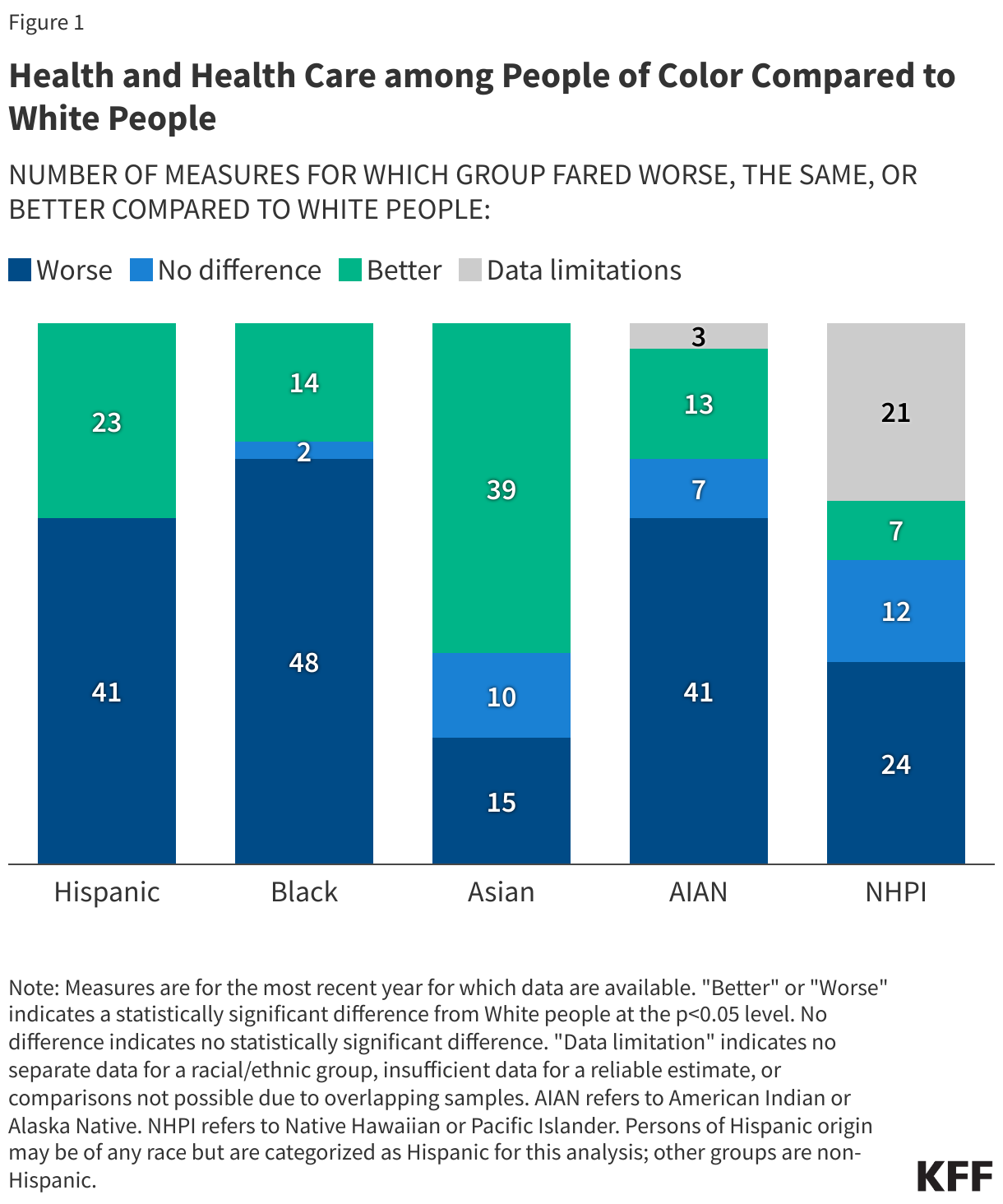
Data are key for identifying disparities and the factors that drive them, developing interventions and directing resources to address them, as well as for assessing progress and establishing accountability. This analysis examines how people of color fare compared to White people across 64 measures of health, health care, and social and economic factors that drive health using the most recent data available from federal surveys and administrative sets as well as the 2023 KFF Survey on Racism, Discrimination, and Health, which provides unique nationally-representative measures of adults’ experiences with racism and discrimination, including in health care (see About the Data).
Where possible, we present data for six groups: White, Hispanic, Black, Asian, American Indian or Alaska Native (AIAN), and Native Hawaiian or Pacific Islander (NHPI). People of Hispanic origin may be of any race, but we classify them as Hispanic for this analysis. We limit other groups to people who identify as non-Hispanic. When the same or similar measures are available in multiple datasets, we use the data that allow us to disaggregate for the largest number of racial and ethnic groups. Unless otherwise noted, differences described in the text are statistically significant at the p<0.05 level.
We include data for smaller population groups wherever available. Instances in which an estimate has a 95% confidence interval width greater than 20 percentage points or 1.2 times the estimate may not be reliable and are noted in the figures. Although these small sample sizes may impact the reliability, validity, and reproducibility of data, they are important to include because they point to potential underlying disparities that are hidden without disaggregated data. For some data measures throughout this brief we refer to “women” but recognize that other individuals also give birth, including some transgender men, nonbinary, and gender-nonconforming persons.
Social and Economic Factors
Racial Disparities in Social and Economic Factors
Social and economic factors like socioeconomic status, education, immigration status, language, neighborhood and physical environment, employment, and social support networks, as well as access to health care have an important influence on health. There has been extensive research and recognition that addressing social, economic, and environmental factors is important for addressing health disparities. Research also shows how racism and discrimination drive inequities across these factors and impact health and well-being.
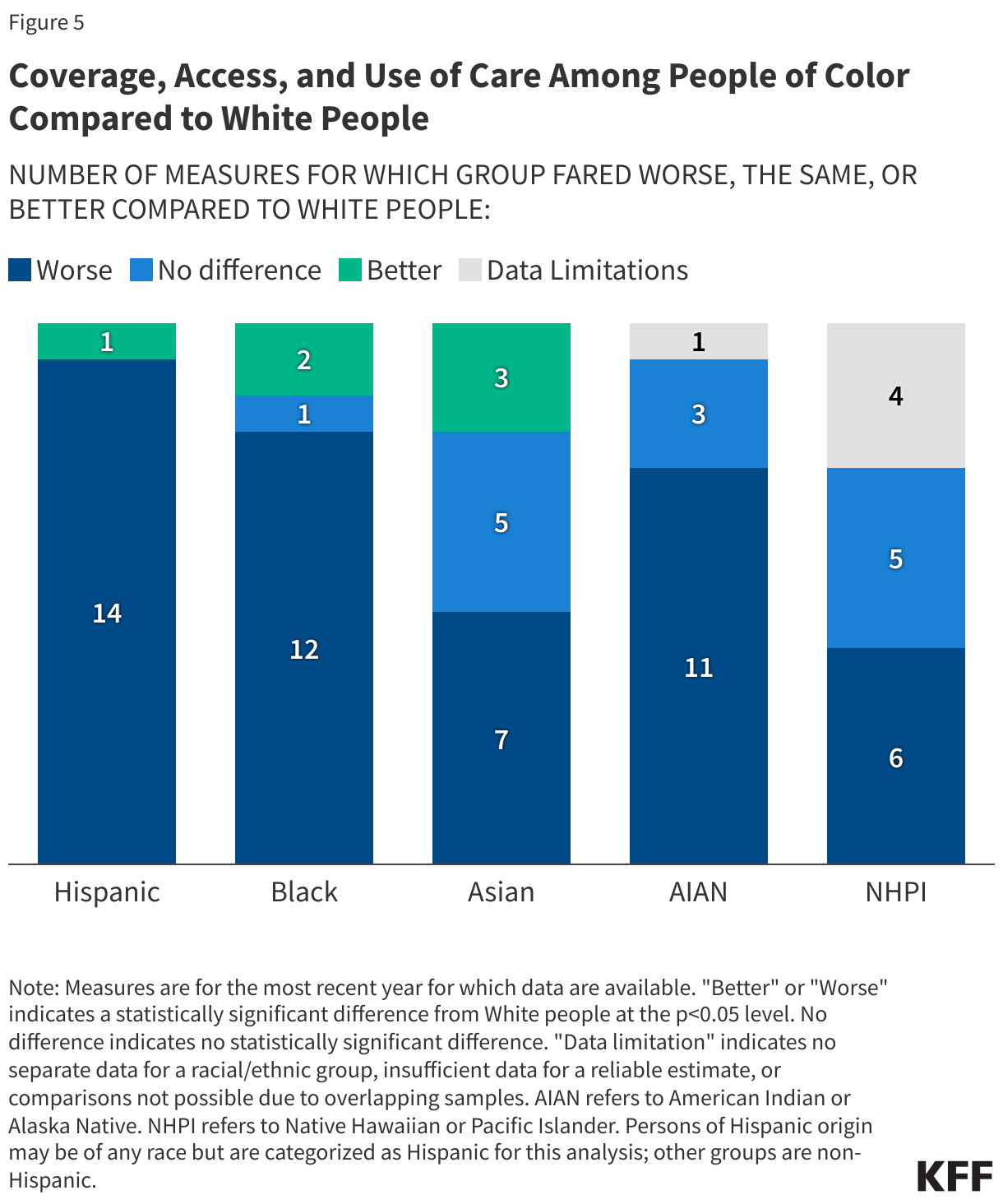
Black, Hispanic, and AIAN people fare worse compared to White people across most examined social and economic measures (Figure 29). Experiences for Asian people are more mixed relative to White people across these examined measures. NHPI people fare worse than White people for half of the measures, however, reliable or disaggregated data are missing for a number of measures.
Work Status, Family Income, and Education
While most people across racial and ethnic groups live in a family with a full-time worker, disparities persist (Figure 30). AIAN (68%), Black (74%), NHPI (79%), and Hispanic (81%) people are less likely than White people (83%) to have a full-time worker in the family. In contrast, Asian people (86%) are more likely than their White counterparts (86%) to have a full-time worker in the family.
Despite the majority of people living in a family with a full-time worker, over one in five AIAN (25%) and Black (21%) people have family incomes below the federal poverty level, over twice the share as White people (10%). Rates of poverty were also higher among Hispanic (16%) and NHPI (15%) people (Figure 31).
Black, Hispanic, AIAN, and NHPI people have lower levels of educational attainment compared to their White counterparts. Among people ages 25 and older, over two thirds (69%) of White people have completed some post-secondary education, compared to less than half (45%) of Hispanic people, just over half of AIAN (52%) and NHPI (54%) people, and about six in ten (58%) Black people (Figure 33). Asian people (75%) are more likely than White people (69%) to have completed at least some post-secondary education.
Net Worth and Homeownership
Black and Hispanic families have less wealth than White families. Wealth can be defined using net worth, a measure of the difference between a family’s assets and liabilities. The median net worth for White households is $285,000 compared to $44,900 for Black households and $61,600 for Hispanic households (Figure 33). Asian households have the highest median net worth of $536,000. Data are not available for AIAN and NHPI people.
People of color are less likely to own a home than White people (Figure 34). Nearly eight in ten (78%) White people own a home compared to 70% of Asian people, 61% of AIAN people, 56% of Hispanic people, about half of Black people (50%), and 43% of NHPI people.
Food Security, Housing Quality, and Internet Access
Hispanic, AIAN, and Black people are roughly twice as likely to experience food insecurity compared to their White counterparts (Figure 35). Asian and White people have similar rates of food insecurity (11% vs 12%, respectively).
People of color are more likely to live in crowded housing than their White counterparts (Figure 36). Among White people, 3% report living in a crowded housing arrangement, defined by the American Community Survey as having more than one person per room. In contrast, almost three in ten (28%) NHPI people, roughly one in five Hispanic (18%) and AIAN (16%) people, and about one in ten Asian (12%) and Black (8%) people report living in crowded housing. However, these differences may reflect cultural preferences for multigenerational living rather than a housing challenge.
AIAN, Black, and NHPI people are less likely to have internet access than White people (Figure 37). Higher shares of AIAN (10%) and Black (5%) people say they have no internet access compared to their White counterparts (4%). In contrast, Asian (2%) and Hispanic (3%) people are less likely to report no internet access than White people (4%).
Transportation
Black, Asian, AIAN, and Hispanic people are more likely to live in a household without access to a vehicle than White people (Figure 38). About one in eight (13%) Black people and about one in ten Asian (9%) and AIAN (9%) people live in a household without a vehicle available, followed by 7% of Hispanic people. The shares of NHPI (5%) and White (4%) people who report not having access to a vehicle in the household are similar.
Citizenship and English Proficiency
Asian, Hispanic, NHPI, and Black people include higher shares of noncitizen immigrants compared to White people. Asian and Hispanic people have the highest shares of noncitizen immigrants at 24% and 20%, respectively (Figure 39). Asian people are projected to become the largest immigrant group in the United States by 2055. Noncitizen immigrants are more likely to be uninsured than citizens and face increased barriers to accessing health care.
Asian and Hispanic people are more likely to have LEP compared to White people. Almost one in three Asian (31%) and Hispanic (28%) people report speaking English less than very well compared to 1% of White people (1%) (Figure 40). Adults with LEP are more likely to report worse health status and increased barriers in accessing health care compared to English proficient adults.
Experiences with Racism, Discrimination, and Unfair Treatment
Racism is an underlying driver of health disparities, and repeated and ongoing exposure to perceived experiences of racism and discrimination can increase risks for poor health outcomes. Research has shown that exposure to racism and discrimination can lead to negative mental health outcomes and certain negative impacts on physical health, including depression, anxiety, and hypertension.
AIAN, Black, Hispanic, and Asian adults are more likely to report certain experiences with discrimination in daily life compared with their White counterparts, with the greatest frequency reported among Black and AIAN adults. A 2023 KFF survey shows that at least half of AIAN (58%), Black (54%), and Hispanic (50%) adults, and about four in ten (42%) Asian adults say they experienced at least one type of discrimination in daily life in the past year (Figure 41). These experiences include receiving poorer service than others at restaurants or stores; people acting as if they are afraid of them or as if they aren’t smart; being threatened or harassed; or being criticized for speaking a language other than English. Data are not available for NHPI adults.
About one in five (18%) Black adults and roughly one in eight (12%) AIAN adults, followed by roughly one in ten Hispanic (11%), and Asian (10%) adults who received health care in the past three years report being treated unfairly or with disrespect by a health care provider because of their racial or ethnic background. These shares are higher than the 3% of White adults who report this (Figure 42). Overall, roughly three in ten (29%) AIAN adults and one in four (24%) Black adults say they were treated unfairly or with disrespect by a health care provider in the past three years for any reason compared with 14% of White adults.