KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Menlo Park, CA – The Henry J. Kaiser Family Foundation (KFF) announced today that the Honorable Olympia Snowe, former U.S. Senator from Maine, and the Honorable Kathleen Sebelius, former U.S. Secretary of Health and Human Services and former governor of Kansas, have been elected to its Board of Trustees.
Snowe had a longstanding career of service in public office for the state of Maine and is the first woman ever to serve in both houses of a state legislature and to serve in both houses of Congress. Elected to three terms as U.S. Senator, serving from 1995-2013, she is known for her work on budget-deficit reduction, fiscal issues, health care, women’s issues, and foreign affairs. Snowe became a member of the Maine House of Representatives in 1973, was elected to the Maine Senate three years later, and was voted into the U.S. House of Representatives in 1978. After leaving Congress, Snowe authored the book Fighting for Common Ground: How We Can Fix the Stalemate in Congress, drawing on her professional and life experiences as a policy maker. She currently is a senior fellow at the Bipartisan Policy Center and is a co-chair of its Commissions on Political Reform and on Tax Reform. In addition, Snowe serves on corporate and nonprofit boards, advisory boards, and as an advisor to Square Roots, a company focusing on maternal and child health. In 2014, Snowe established the Olympia Snowe Women’s Leadership Institute to help future generations of young women become leaders by raising their confidence and aspirations.
Sebelius served as the U.S. Secretary for Health and Human Services from 2009 to 2014, during the passage and implementation of the Affordable Care Act. Her extensive experience in public office and health care policy include election to two terms as governor of Kansas, a position she held from 2003 to 2009. She also served as Kansas’ insurance commissioner and in the state’s legislature. Secretary Sebelius is currently chief executive officer of Sebelius Resources LLC, providing strategic advice to private companies, non-profit organizations, higher education institutions, and financial investors. Sebelius serves on several boards and holds numerous advisory positions, including as a senior advisor to the Aspen Institute, where she co-chairs the Aspen Health Strategy Group.
“The Kaiser Family Foundation is delighted to have Secretary Sebelius and Senator Snowe bring their deep policy experience and passion for health care issues to our board as the country adjusts to a changing policy landscape and faces new challenges,” said Governor James E. Doyle, chairman of the board of trustees.
KFF’s board has 13 members, including its President and Chief Executive Officer Drew Altman, and former government officials and national leaders from journalism and the nonprofit sector, who serve up to two five-year terms. Additional information on KFF and its board can be found at https://www.kff.org/about-us/. Sebelius and Snowe will begin their board terms in March 2017.
This Visualizing Health Policy infographic provides a snapshot of HIV-related awareness and experiences among adults in the United States, including two demographic groups that make up a disproportionate share of people with HIV: black adults, and gay and bisexual men. Four in 10 black adults, and more than half of gay and bisexual men said they personally know someone who is HIV-positive (HIV+) or who has died of HIV/AIDS, compared with only 28% of adults in the United States overall. In 2014, only 21% of US adults were aware that consistent antiretroviral treatment can significantly reduce the risk of HIV transmission, and only 14% had heard of a new prevention strategy, preexposure prophylaxis. Awareness was only slightly higher among black adults and gay and bisexual men. Although a majority of US adults said they have been tested for HIV, only 16% reported they’ve been tested within the past 12 months; these rates were higher for black adults (39%) and gay and bisexual men (30%). More than half of gay and bisexual men said they are aware that it is recommended they be tested for HIV every 3 to 6 months, yet 56% reported that a clinician has never suggested testing.
This Visualizing Health Policy infographic provides a snapshot of HIV-related awareness and experiences among adults in the United States, including two demographic groups that make up a disproportionate share of people with HIV: black adults, and gay and bisexual men. Four in 10 black adults, and more than half of gay and bisexual men said they personally know someone who is HIV-positive (HIV+) or who has died of HIV/AIDS, compared with only 28% of adults in the United States overall. In 2014, only 21% of US adults were aware that consistent antiretroviral treatment can significantly reduce the risk of HIV transmission, and only 14% had heard of a new prevention strategy, preexposure prophylaxis. Awareness was only slightly higher among black adults and gay and bisexual men. Although a majority of US adults said they have been tested for HIV, only 16% reported they’ve been tested within the past 12 months; these rates were higher for black adults (39%) and gay and bisexual men (30%). More than half of gay and bisexual men said they are aware that it is recommended they be tested for HIV every 3 to 6 months, yet 56% reported that a clinician has never suggested testing.
To date, Kentucky has had one of the most successful ACA implementation experiences among states. Beginning in 2014, the state expanded Medicaid to low-income adults and built its own State-Based Marketplace, kynect. Research points to gains in coverage and reductions in the uninsured, increases in access and health care utilization and positive fiscal impact as a result of the Medicaid expansion.
Governor Bevin, elected in December 2015, ran on a platform to dismantle kynect and to end the Medicaid expansion. However, post-election, the Governor said he would seek a waiver to make changes to the Medicaid expansion. On June 1, Kentucky received approval from the Centers for Medicare and Medicaid Services (CMS) to move forward with plans to transition from kynect to healthcare.gov. On June 22, 2016, Governor Bevin released his proposed Section 1115 demonstration waiver proposal called Kentucky HEALTH (Helping to Engage and Achieve Long Term Health) as an alternative to the current Medicaid expansion.
The proposed Medicaid waiver, modeled largely after the waiver program in Indiana (HIP 2.0), would modify the state’s existing Medicaid expansion and make changes that would affect new enrollees as well as traditional Medicaid enrollees. CMS has indicated it may not approve additional waivers similar to Indiana in advance of an evaluation of Indiana’s program. Kentucky’s proposed waiver includes many provisions similar to those in Indiana and additional provisions not approved in other states, such as employment requirements, and graduated premiums based on length of time on the program. Governor Bevin said in a press conference when he released the waiver proposal for state comment that if the waiver is not approved he would end the expansion. This brief examines what has happened to coverage, access and utilization and the economic impact of the Medicaid expansion in Kentucky and the implications for changes going forward. A summary of the proposed waiver can be found here.
What Happened to Coverage?
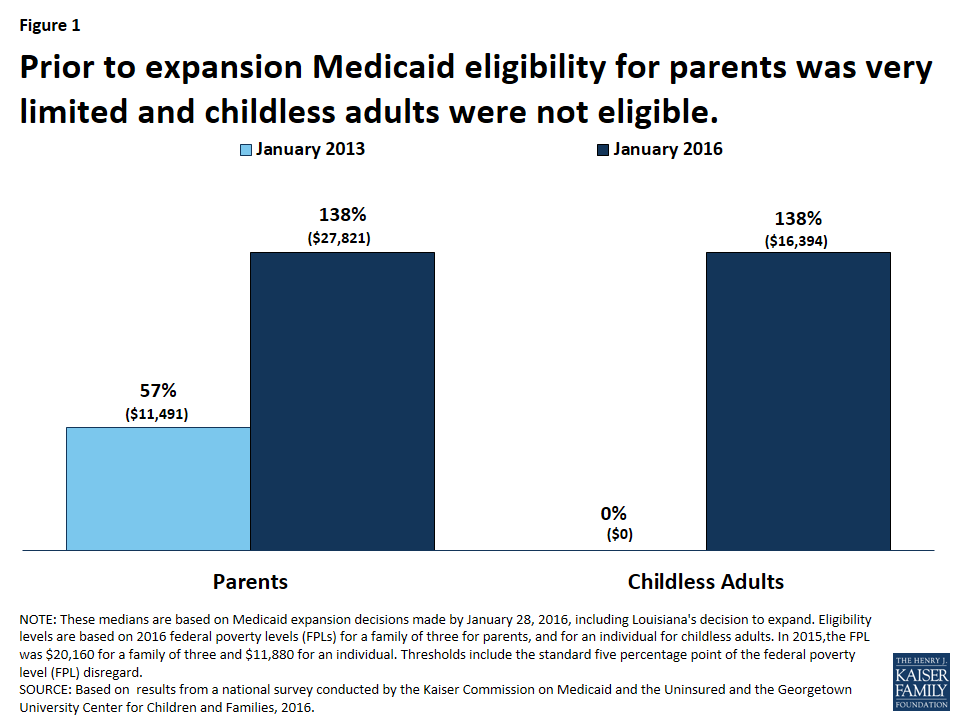
Since implementing the ACA, Kentucky’s uninsured rate for the nonelderly fell from 18.8% in 2013 to 6.8% in 2015, one of the largest reductions in the country.1 The reduction is largely attributable to changes in Medicaid eligibility and gains in Medicaid coverage. Before the implementation of the expansion, eligibility for parents was at 57% FPL ($11,491 for a family of 3 in 2016) and there was no coverage for adults without dependent children.2 Under the ACA Medicaid expansion, eligibility for adults was expanded up to 138% of poverty ($16,394 for an individual or $27,821 for a family of 3 in 2016). (Figure 1)
Figure 1: Prior to expansion Medicaid eligibility for parents was very limited and childless adults were not eligible.
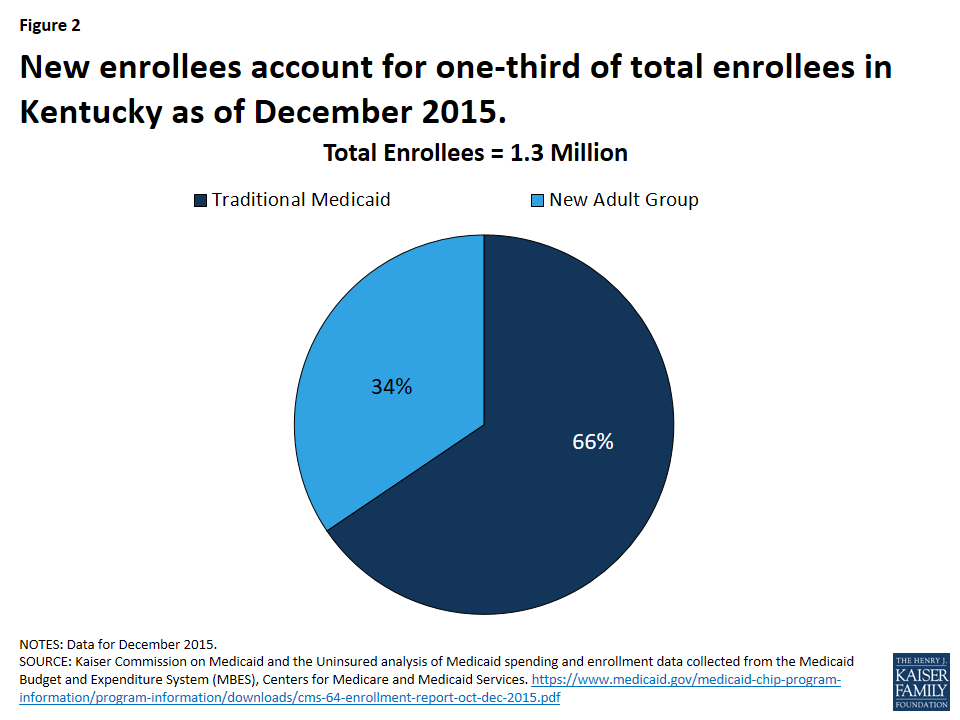
CMS data show that Medicaid enrollment in Kentucky from pre-ACA to January 2016 increased by 95% (the highest growth across all states).3 Other data show that of the 1.3 million Medicaid enrollees as of December 2015, 439,000 (or one-third) are “new enrollees” and qualify for 100% federal matching funds (Figure 2).4 Without the expansion, the large majority (more than eight in ten) of these new enrollees would have been uninsured and without a coverage pathway because their income is below poverty.
Figure 2: New enrollees account for one-third of total enrollees in Kentucky as of December 2015.
What Happened to Access and Utilization?
Research shows that the expansion in Kentucky has helped to increase access and utilization of health care services in a state with historically poor health status indicators. For example, one study shows that compared to Texas, Medicaid expansion in Kentucky was associated with significant reductions in skipping medications because of cost as well as decreases in trouble paying medical bills among low-income adults between Nov.-Dec. 2013 and Nov.-Dec. 2014.5 Another study shows that by the end of 2014, low-income Kentuckians experienced a 16 percentage point (40%) reduction in unmet medical need because of cost relative to the pre-expansion (2006-2013) period.6 Finally, another study shows that more than 300 new behavioral health providers enrolled in Kentucky Medicaid and at least 13,000 individuals with a substance use disorder received related treatment services during the first year of expansion.7
What Are the Economic Implications?
Studies point to fiscal gains associated with the Medicaid expansion. For example, one study shows state savings were realized by transitioning individuals accessing Medicaid services through pre-ACA eligibility categories to the new eligibility group (with initial 100% enhanced federal funding).8 In addition, another study shows that the expansion was estimated to have a positive cumulative fiscal impact of $819.6 million by SFY 2021.9 The same study shows that Medicaid expansion created more than 12,000 jobs in Kentucky in SFY 2014, including 5,400 health care and social service jobs. Expansion is projected to create more than 40,000 jobs in Kentucky through SFY 2021 with an average salary of about $41,000.10 Finally, Kentucky hospitals experienced a reduction of $1.15 billion in uncompensated care charges when comparing the first three quarters of CY 2013 to the same period in CY 2014.11
Looking Ahead
Kentucky has had a successful implementation of the ACA Medicaid expansion to date. Robust enrollment has resulted in significant coverage gains and reductions in the uninsured as well as increases in access to care and financial protections for families. Other studies point to net fiscal benefit from the expansion including increases in jobs, and reductions in uncompensated care for hospitals. A Kaiser Family Foundation survey of the views of Kentucky residents completed just after the Governor’s election in 2015 found that nearly three in four (72%) Kentuckians said they would prefer to keep the state’s Medicaid program as it is rather than scale it back it to cover fewer people. About two-thirds (67%) felt that the Medicaid program is working well for most low-income people in the state; this share rises to 84% among adults who are actually covered by Medicaid.12 Ending or altering the expansion as proposed in the recent demonstration waiver proposal could jeopardize coverage, access and fiscal gains achieved under the expansion to date.
Health Insurance Coverage: Early Release of Estimates from the National Health Interview Survey, 2013 and 2015↩︎
Benjamin Sommers, Robert Blendon, and E. John Orav, “Both the ‘Private Option’ And Traditional Medicaid Expansions Improved Access To Care For Low-Income Adults,” Health Affairs 35, no. 1 (January 2016): 96-105, http://content.healthaffairs.org/content/35/1/96.abstract↩︎
Deborah Bachrach, Patricia Boozang, Avi Herring, and Dori Glanz Reyneri, States Expanding Medicaid See Significant Budget Savings and Revenue Gains, (Manatt Health Solutions, prepared by the Robert Wood Johnson Foundation’s State Health Reform Assistance Network, March 2016), http://www.rwjf.org/content/dam /farm/reports/issue_briefs/2016/ rwjf419097↩︎
The number of rural hospital closures has increased significantly in recent years. This trend is expected to continue, raising questions about the impact the closures will have on rural communities’ access to health care services. To investigate the factors that contribute to rural hospital closures and the impact those closures have on access to health care in rural communities, the Kaiser Commission on Medicaid and the Uninsured and the Urban Institute conducted case studies of three hospital closures that took place in 2015: Mercy Hospital in Independence, Kansas; Parkway Regional Hospital in Fulton, Kentucky; and Marlboro Park Hospital in Bennettsville, South Carolina. Two of these hospitals were in states that did not adopt the Medicaid coverage expansion under the Affordable Care Act (ACA) (Kansas and South Carolina), while one of the hospitals was located in a Medicaid expansion state (Kentucky). Key findings include the following:
A number of factors contributed to the rural hospital closures, including aging, poor, and shrinking populations, high uninsured rates and a payer mix dominated by Medicare and Medicaid, economic challenges in the community, aging facilities, outdated payment and delivery system models, and business decisions by corporate owners/operators.
The hospital closures reduced local residents’ access to care, especially emergency care. While inpatient hospitals in these and other communities may not be sustainable, without new models of health care delivery in place, hospital closures can lead to gaps in access. The closures led to an outmigration of health care professionals and worsened pre-existing challenges around access to specialty care. Some communities were able to adapt to fill in gaps in access to primary care. Elderly and low-income individuals were more likely than others to face transportation challenges following the closures, and were thus more likely to delay or forgo needed care.
New care models may be better able to address the health care needs of rural communities. Some rural hospitals may be able to adapt and new models may be created to address changing demographics and delivery systems. Such reconfiguration may require federal support and assistance as well as regional planning efforts. A state’s decision about the Medicaid expansion has an important impact on hospital revenues and access to care, but the sustainability of rural hospitals depends on a broader set of factors.
Issue Brief
Introduction and Methods
The number of rural hospital closures has increased significantly in recent years. This trend is expected to continue, raising questions about the impact the closures will have on access to health care services in rural communities.1 To investigate the factors that contribute to rural hospital closures and the impact of those closures on access to health care in rural communities, the Kaiser Commission on Medicaid and the Uninsured and the Urban Institute conducted case studies of three hospital closures that took place in 2015: Mercy Hospital in Independence, Kansas; Parkway Regional Hospital in Fulton, Kentucky; and Marlboro Park Hospital in Bennettsville, South Carolina.
In selecting hospital closures for study, we limited ourselves to hospitals that: 1) had closed recently, 2) had not converted to another type of facility (e.g., an urgent care facility) following the closure; and 3) had been reimbursed by Medicare under the prospective payment system (PPS) through predetermined fixed reimbursement rates, not on a cost basis. We applied these criteria to enhance our understanding of the immediate impacts of complete rural hospital closures on community access to care, and to eliminate the effect of Medicare reimbursement type as a confounding factor in our analysis. Also, because we wished to examine the role of state decisions about whether or not to expand Medicaid to nonelderly adults under 138% of the federal poverty level under the Affordable Care Act (ACA), we selected two hospital closures that took place in states that did not expand Medicaid (Kansas and South Carolina) and one closure that took place in a Medicaid expansion state (Kentucky).2
For each case study, we conducted 6-8 interviews with community stakeholders, including nearby hospitals, community health centers, provider associations, health plans, public officials, and local business leaders. We also reviewed publicly-available materials related to the closures and, where available, state and regional rural health analyses and planning initiatives, and interviewed state and national rural health experts to gain perspective on these closures in the context of broader trends.
The case studies addressed the following research questions:
What factors contributed to the hospital closure?
How has the closure affected access to care?
What were the broader community effects of the closure? and
Did the state Medicaid expansion decision make a difference in the closure of the hospital or on residents’ ability to access care after the closure?
This brief addresses each of these questions and concludes by addressing the implications of a growing number of rural hospital closures for rural communities and rural health.
Background
In 1946, Congress authorized the Hill-Burton program, which provided federal funding for construction of public and nonprofit hospitals in rural communities. The program led to a significant increase in the number of rural hospitals in the country, particularly in the South. In 1983, responding to significant increases in Medicare hospital spending, Congress mandated use of fixed predetermined reimbursement rates for hospitals through the PPS. Following the adoption of PPS, many rural hospitals closed in the 1980’s and 1990’s.3 In response to growing concerns over rural health care access, CMS implemented the Medicare Rural Hospital Flexibility Program of 1997 (Flex Program), which authorized payment of inpatient and outpatient services on a “reasonable cost basis” for hospitals designated as Critical Access Hospitals (CAHs).4 To be classified a CAH, a hospital must have no more than 25 inpatient beds and must be at least 15 miles by secondary road and 35 miles by primary road from the nearest hospital; until 2006, however, states could waive the distance requirement by designating a hospital as a “necessary provider.”5 The closure trend slowed for several years following adoption of the Flex Program, but picked up again during the Great Recession of 2008-09.
There are nearly 5,000 short-term, acute care hospitals in the United States. Half of these hospitals are in urban areas and half are in rural areas. About 4 in 10 rural hospitals are located in the South.6 More than half of rural hospitals are CAHs (53.5%); smaller shares of rural hospitals are designated as Sole Community Hospitals (SCHs) (13%), Medicare Dependent Hospitals (MDHs)(8%), and Rural Referral Centers (RRCs) (11%).7 All of these designations provide enhanced or supplemental reimbursement under Medicare, using different formulas.8 Rural hospitals that do not qualify for these Medicare programs are reimbursed as standard Medicare PPS Hospitals.
In 2012-2013, rural hospitals had an average of 50 beds and a median of 25 beds. They had an average daily census of 7 patients and 321 employees, and they were 10 years old on average. Compared to urban hospitals, rural hospitals are more likely to be in counties with an elderly and poor population.9 According to The North Carolina Rural Health Research Program (NC RHRP) at the Cecil G. Sheps Center for Health Services Research, which tracks rural hospital closures, there were 72 rural hospital closures between January 2010 and April 2016, compared to 42 closures between 2005 and 2009, and since the 2008-2009 recession, the annual number of closures has increased each year.10 More than half of all rural hospital closures since 2010 were in the South and few Southern states have expanded Medicaid under the ACA.
This report focuses on three hospital closures that took place in 2015: Mercy Hospital in Independence, Kansas; Parkway Regional Hospital in Fulton, Kentucky; and Marlboro Park Hospital in Bennettsville, South Carolina. All three hospitals were privately owned. Bed size ranged from 45 to 102, and two of the hospitals had fewer than 1,000 admissions per year. Occupancy rates were also low. The nearest hospital post-closure was 12 to 15 miles away; in one community, the nearest hospital was across the state line. Table 1 shows selected basic characteristics of the three hospital closures we studied. More detailed information about the hospitals can be found in the Appendix.
Table 1: Selected characteristics of the three study hospitals
A subsidiary of Community Health Systems operated the hospital; Medical Properties Trust, a real estate trust owned the facility / For-Profit
Number of Beds
70
45
102
Occupancy
Unknown
25%
13.9% as of 2013
Employees
170-190
243 (11 physicians as of 2013)
100
Admissions
700 in 2014
995/year
Unknown
Nearest Hospital/Distance away
Tennova Healthcare-Volunteer Martin, in Martin, TN (owned by Community Health Systems) Approximately 12 miles
Jackson Purchase Medical Center (Life Point Health), in Mayfield, KYApproximately 22 miles
Wilson Medical Center, in Neodesha, KS (owned by Duke LifePoint) Approximately 14 miles
Coffeyville Regional Medical Center, in Coffeyville, KS (city-owned hospital)Approximately 20 miles
McLeod Health Cheraw, in Cheraw, SC (owned by McLeod Health)Approximately 15 miles.Scotland Memorial Hospital, in Laurinberg, NC (community- owned and -controlled, not-for-profit)Approximately 17 miles
Medicaid Expansion State
Yes
No
No
NOTES: Data regarding the number of beds, occupancy rate, number of employees, and admission rates were collected from local news outlets that reported on the respective closures, not from formal reports produced by the hospitals. Many of the media reports did not cite the original source for the data, or data were not available for all three communities. Information regarding the location of nearby hospitals is based on interviews with stakeholders and was verified with data from Google Maps.
Key Findings
What factors contribute to rural hospital closures?
Rural areas face challenging demographic, social, and economic pressures. Respondents in all three communities pointed to similar economic and demographic trends that contributed to the closures. They cited high poverty and uninsured rates in rural communities, high rates of Medicare and Medicaid coverage, and declining populations. In each community, poverty rates were higher than state and national averages and median incomes were lower, and the population was shrinking. Two of the counties where the study hospitals were located (Fulton County, Kentucky and Montgomery County, Kansas) had higher rates of elderly residents, and two counties (Fulton and Marlboro County, South Carolina) had higher rates of Black residents relative to the rates in the state overall and the U.S. (See Appendix Table 1)
Stakeholders also noted the loss of major employers, the “evaporation” of local industry (i.e., mining, textiles, manufacturing and agriculture), and the subsequent rise in unemployment and loss of employer health coverage as factors contributing to the closures. The communities’ economic difficulties were exacerbated by the recent recession. With the disappearance of jobs, many young adults have left town in search of other opportunities, leading to further population decline and to a graying population with greater health care needs.
Privately insured patients often went elsewhere for care, hurting the local hospital’s revenue base and contributing to perceived low quality of the local hospital. In all three case studies, respondents reported that, prior to the hospital closure, community residents with private insurance or other resources typically travelled to bigger, newer hospital systems outside the community, weakening the hospital’s payer mix and also reinforcing local perceptions – often based on anecdotal accounts from friends and family members — that the local hospital was of low or poor quality. The local community hospital may have been older, and due to financial struggles prior to closure, may have invested less in infrastructure improvements compared to facilities in nearby urban areas, contributing to its perceived poor quality. The fact that, even while the local hospital was operating, residents had to go elsewhere for many types of specialty care, including labor and delivery services and surgery in some cases, reinforced views that the hospital was inferior. Without privately insured patients, study hospitals were left with high rates of uninsured patients and patients with public insurance (Medicare and Medicaid), which pay lower reimbursement rates than commercial insurance that are often below costs. All these factors resulted in negative margins. With insufficient revenues to maintain their aging facilities, the hospitals declined further, adding to negative perceptions of their quality, leading in turn to continuing deterioration of their finances.
“If you have health insurance and a car, you’ll drive [out of the community] for care because a perception exists that bigger, brighter facilities offer better quality services.” – South Carolina Stakeholder
“Would-be patients from Independence chose to get their care elsewhere, which contributed to the death spiral for Mercy Hospital.” – Kansas Stakeholder
Rural hospitals built in neighboring communities under Hill-Burton now compete for limited patients, federal dollars, and health care resources. All three case study hospitals were located in close proximity to larger hospitals in nearby communities. One respondent commented: “If you were going to plan placement of hospitals now, you would implement a very different design.” Clusters of hospitals within a small geographic area are not only a barrier to CAH designation, but also result in hospitals competing for limited federal dollars, resources, providers, and patients. Along the same lines, some respondents observed that rivalries between neighboring communities, counties, and hospitals have bred competition instead of collaboration, sometimes leading to redundant health care and other services and costly inefficiencies.
Corporate business decisions, rather than assessments of local needs or planning, drove the hospital closures. In all three sites, the large health systems that owned and managed the hospitals made the decision to close them based not on community needs, but on corporate business considerations that favored other hospitals in their system over the ones they closed. Typically, there was little or no local process of consultation or public input. In both Fulton, Kentucky and Bennettsville, South Carolina, local stakeholders reported that the hospital’s owner/operator invested its resources preferentially in a neighboring community hospital that it also owned, at the expense of the closed facility. Mercy Health System invested in rebuilding its hospital in Joplin, Missouri – 75 miles from Independence – after it was destroyed by a tornado, and reportedly “lost its focus” on the smaller Mercy Hospital in Independence. Although the hospital worked with an advisory group that included community stakeholders to address the closure of Mercy Hospital and potential alternative uses of the facility, the advisory group had limited influence over the ultimate decision by Mercy Health System to close it. The group was also reportedly required to maintain confidentiality; as a result, the public felt uninformed and excluded from the process. In Kentucky, public officials from Fulton County wanted to take over the hospital and find other providers who might continue services in the area, but CHS rejected this offer, likely, to preempt competition for patients in the county. Further, CHS placed restrictions on the use of the hospital – namely, it permitted no acute care facility to operate there, an action that one respondent said “strangled” the community’s access to local health care services.
Several respondents cited the “shift from mission to margin” as a major factor in the hospital closures and in the lack of consideration or planning for the impact on the community. A number observed that local residents and public officials often lack the expertise or experience needed to negotiate with large corporate health systems and have limited understanding of the transformations taking place in health care delivery and payment systems widely.
Changes in Medicare and Medicaid payment over the past few years have had an adverse effect on rural hospitals. Decreases in Medicare reimbursement rates have exacerbated financial pressure on already struggling rural hospitals, especially those with an older patient population. In recent years, Medicare cuts arising from budget sequestration and other federal policies14 have led to lower reimbursement rates overall, while specific provisions of the ACA, such as the Readmissions Reduction Program, under which CMS reduces PPS payments to inpatient hospitals with high readmission rates, have also resulted in lower Medicare reimbursements for many hospitals.15 CAHs are often in a stronger financial position than rural PPS hospitals because they receive cost-based Medicare reimbursement, but our study hospitals either did not meet the criteria to qualify as a CAH or had declined to explore conversion options. Since 2006, it also has been more difficult to obtain a CAH designation because states can no longer waive the CAH distance requirements by identifying a hospital as a “necessary provider.”
Rural hospitals may also be adversely affected by budget-driven state policy actions, such as Medicaid rate freezes or other reductions, and by transitions to Medicaid managed care. For example, a stakeholder in Fulton, Kentucky reported that some Medicaid managed care plans were working to discourage inappropriate emergency department (ED) use by reimbursing the hospital only a small triage fee, rather than the full fee, for visits later determined to be non-emergent. Because the ED is a major access point for primary care in rural communities, the majority of patients in the ED present with more common ailments that do not require emergency care. Nevertheless, ED providers must determine if patients have a life-threatening condition and may deliver a variety of services to patients who turn out to need urgent or primary care; due to the triage fee policy, they will not be reimbursed for a significant portion of their costs for such patients.16 Because rural hospitals are generally more reliant on public payers, changes to Medicare and Medicaid reimbursement can have a more significant effect on these hospitals. An analysis of profitability of urban and rural hospitals by Medicare payment classification shows that rural PPS hospitals with 26-50 beds and Medicare Dependent Hospitals had the lowest profitability.17
Rural hospitals have not adapted to new models of payment and service delivery that emphasize preventive and primary care provided in outpatient settings. Increasingly, Medicare, Medicaid, and large private payers are implementing payment and delivery system reforms that move “from volume to value” and shift investment away from inpatient care and toward preventive and primary care and greater access to care in outpatient settings. As one South Carolina stakeholder put it, “We used to pay hospitals to keep patients in, now we pay to keep them out.” Consistently, we heard from respondents that rural hospitals have been slow to adapt to these reforms and have instead maintained their hospital-centric focus oriented toward generating inpatient admissions.
South Carolina’s Healthy Outcomes Plan (HOP) is an initiative to support hospitals proposing service delivery models to coordinate care for chronically ill, uninsured, high utilizers of emergency department (ED) services. Approximately $40 million was reportedly spent statewide, with some funding for Marlboro Park Hospital. However, it was not enough to save the hospital; one respondent described the impact of the program on rural hospitals as “like putting a finger in a dike.”
What is the impact of rural hospital closures on access to care?
The hospital closures reduced access to emergency care. In all three case studies, stakeholders emphasized that a major impact of the hospital closure was the loss of access to emergency care in the community. They pointed out that the hospitals’ EDs had also served as a safety-net for people with acute mental health or addiction treatment needs18 by stabilizing them and arranging for their transport when needed; when the hospital closed, local capacity to address these needs disappeared. Respondents cited the immediate and ongoing need to ensure emergency transportation to neighboring hospitals following the closure.
Some public investment in ambulance services may be needed in the wake of a rural hospital closure. After Mercy Hospital closed, for example, the city of Independence purchased two new ambulances and hired an additional EMS crew. Fulton, Kentucky officials responded to Parkway Regional’s closure by funding the ambulance service with city and county dollars. However, respondents also noted that there can be challenges transporting patients back home after they are taken by ambulance to another community for care and this problem can be significant for low-income patients who do not have the means or support system in place to ensure their travel home.
Many physicians and other providers left the community immediately following the rural hospital closure. Regardless of hospital closures, rural communities characteristically face difficulty recruiting and retaining providers, resulting in systemic workforce shortages. The large hospital systems in the three study communities typically employed the local physicians, so when the hospital closed, many physicians relocated to another hospital in the owner’s system or left the area. As a result, the communities were often left without key providers. In Independence, Kansas, providers began to leave Mercy Hospital even before it closed when talk of closure “was in the air,” hastening the deterioration of the already struggling hospital. Some also said that Mercy Health System made competitive offers to physicians formerly employed by the hospital to induce them to transfer to another hospital in the Mercy system, farther away from Independence. Respondents reported that physicians formerly employed by the hospital in Bennettsville, South Carolina were barred from entering into agreements with other hospitals in the area and were relocated to CHS’ Martin, Tennessee facility following the closure. In all three study sites, respondents cited the outmigration of providers in the wake of the hospital closure as a significant problem, especially given the challenges of recruiting providers to rural areas.
Because hospital emergency departments are a major source of primary care in rural areas, closures can have a significant impact on access to primary care, but some communities can fill these gaps. Respondents in all three study sites reported that most visits to the hospital ED were for urgent care or primary care because access to such care in community-based outpatient settings was limited; “true emergencies” made up only a small percentage of all ED visits. One South Carolina respondent referred to a “culture of overutilization” of rural EDs. Stakeholders from Kansas estimated that as many as 90% of ED visits to Mercy Hospital were for non-emergencies.
In two of the communities we studied (Independence, Kansas and Bennettsville, South Carolina), some stakeholders described a relatively smooth transition to community-based primary care following the closure. In both cases, federally qualified health centers (FQHCs) in or near the community were able to expand their provision of primary care. In Independence, office-based primary care is available in the community, while in Bennettsville, more people have to travel to obtain primary care since the closure. Some respondents commented that, following the closure of the hospital in Independence, nearby hospital systems opened competing primary care clinics in the community, leading to a fragmented health system. However, others noted that increased provider and health system interest in serving their community, often as a means to expand their market share, improved access to primary care.
At the time of our interviews, access to primary care remained more challenging in Fulton, Kentucky, where there was no nearby FQHC. Respondents reported that access to care is affected by ongoing competition between the two main health systems in the area, CHS and LifePoint. The border between Kentucky and Tennessee runs through the Fulton community and, following the closure, CHS moved some providers and staff to its Martin, Tennessee facility and relocated its outpatient services from Fulton to a new clinic across the state border in South Fulton, Tennessee, where at least some Medicaid patients are not eligible to receive care. LifePoint is trying to establish clinics in Fulton County but CHS placed a restriction on the Parkway Regional facility to prevent it from being used as a primary care hospital or operating in an acute capacity.
The hospital closures also exacerbated gaps in access to specialty care. Rural hospitals in small communities cannot afford to offer the range of specialty services available in hospitals in larger communities, and rural residents routinely travel for certain types of specialty care, particularly for complex medical needs. But respondents reported that pre-existing difficulties in accessing specialty care increased following the closures. In many cases, specialists who had visited the local hospital on a regular basis to provide outpatient visits were no longer available to see patients locally after the hospital closed. With the closure, local residents also lost their access point for referrals to subspecialists. Several respondents commented that many people now forgo lab work and diagnostic imaging rather than travel to another community for the services. Problems with access to obstetric care, diagnostic testing, laboratory tests, and mental health care – services that had often been provided at the hospital before its closure but were no longer available locally – were a consistent theme. Unmet need for mental health and substance use disorder treatment, a significant issue before the hospital closures, has also intensified. Respondents across all three communities reported that longer travel time and distance exacerbate tendencies to delay or forgo care, particularly among elderly and low-income individuals.
What are the other effects of rural hospital closures on communities?
Hospital closures result in job losses and have other ripple effects in the surrounding community. A hospital closure can eliminate a hundred or more jobs immediately, a significant loss in communities with small populations. In some cases, the local hospital is one of the largest employers in the community. Some health care providers and other hospital employees move away following a closure; others remain but commute elsewhere for work. The loss of jobs and residents has a negative impact on the tax base in the community, shrinking available resources for schools and other public services, potentially impacting jobs in the public sector as well.
Hospital closures can make it more challenging for rural communities to attract employers. The loss of a hospital makes it more difficult for rural communities to recruit new industries and employers to the area. Some businesses require, as a condition of locating in an area, that their employees have access to a hospital ED in close proximity. Thus, a hospital closure can compound the very same economic strains that contributed to the closure in the first place. Some respondents noted that the impact of the hospital closure on the local economy was more significant than its impact on access to care. The challenge, according to one expert, raises issues beyond health policy: “How can we make sure rural communities can be left financially viable without a hospital?”
How do state Medicaid expansion decisions affect rural hospitals and access to care?
Medicaid expansion increases access to care in rural communities.19 In Fulton, many uninsured adults gained coverage when Kentucky implemented the Medicaid expansion, giving them access to providers and services they were previously unable to afford. Respondents reported that Medicaid coverage of non-emergency medical transportation is very important in rural communities and even more so in the event of a local hospital closure, because residents more often have to travel to get care. Respondents in Kansas and South Carolina reported that the tendency of uninsured residents in rural communities to forgo preventive care and to delay treatment until their health conditions worsen can be exacerbated by the loss of a local hospital, and they said that a decision by their state to expand Medicaid would have increased access to needed care for the low-income uninsured population.
However, Medicaid expansion alone cannot overcome the financial challenges facing rural hospitals. Respondents in all three case studies expressed the opinion that although Medicaid expansion can bring increased revenues into struggling hospitals, it is only one of many factors that impact hospitals’ financial sustainability. Kentucky respondents pointed out that the state’s Medicaid expansion may have delayed Parkway Regional Hospital’s closure, but that since the Medicaid expansion, Parkway Regional and three other rural hospitals in the state have closed. In Kansas, respondents likewise cited the lack of Medicaid expansion as one of many factors that contributed to Mercy Hospital’s closure – one person described the hospital’s demise as “death by a thousand cuts.”20 The theme that emerged in all three case studies is that what caused the hospital closure was the confluence of difficult rural demographic and economic trends, the failure of the hospital or health system to adapt to changing health care payment and delivery systems, aging facilities and challenging payer mixes. Stakeholders across the board said they believed that increased financing through Medicaid expansion could help other at-risk rural hospitals, but not alone overcome these fundamental challenges.
A recent study found that while rural hospitals were showing declines in charity care as a result of the ACA, the net financial impact was less clear because of bad debt from high-deductible plans as well as “shortfalls” between payments and costs of care in Medicare and Medicaid.21 The study also noted concern about upcoming cuts to Medicaid Disproportionate Share payments.
What do increasing hospital closures imply for the future of rural health care delivery and access?
Rural communities could benefit from new health care delivery models that can provide access to care. Several stakeholders emphasized that new health care delivery models are necessary to address rural health needs. They discussed various strategies to meet the need for more primary and preventive care, effective referral systems for specialty care, and alternative access to emergency services when a hospital closes. They also emphasized the need for reforms to permit increased use of telehealth services. They suggested that an appropriate model would lie somewhere between a CAH and an FQHC; such models, they noted, would require changes in federal Medicare reimbursement policy and/or changes in health care facility state licensure rules. Several leading rural models are summarized in the table below. In addition, the federal government has funded several rural health demonstration projects to test out new models of care.22 (See box about Rural Health Transformation Models)
More investment in transportation could mitigate the impact of rural hospital closures. Road systems were good in areas surrounding our study communities and, in all three sites, there was at least one neighboring hospital within 15 miles. But even in these communities, respondents stressed the need for more reliable transportation systems to facilitate access to health care services. Many rural communities do not have public transportation systems, so patients must have a car or someone willing to share their car or drive them, and money for gas to travel to seek medical care. Travel is an issue particularly for elderly people, who often cannot drive. One respondent emphasized that rural health policy needs to address the social determinants of health as well.
The investment of additional resources to support community needs assessments and regional planning could help further efforts to ensure access to care in rural communities. Despite the widespread movement away from hospital-centric health care delivery elsewhere, many rural communities continue to rely on the local hospital as the locus of care. Rural communities frequently lack the resources and infrastructure to evaluate community needs and develop a plan for access to care post-hospital closure. When there is no plan for the future, the announcement of a hospital closure can lead to chaos and divisions in a community. Regional planning efforts and technical assistance could help to educate and engage local residents, support assessments of community health care needs, improve the ability of communities to negotiate with large health systems, and promote integrated systems of primary care, referral centers for specialty care, and rational allocation of health care resources overall. Regional planning in areas where large hospital systems are present has the potential to bring the advantages of these systems’ resources, health information systems, and capacity to invest in facilities, recruit providers, develop specialty referral systems, and implement telehealth initiatives, to rural communities. With such planning, these communities might be able to demonstrate to prospective new employers that a strong health care system is in place, even if there is no hospital in the local community.
Rural Health Transformation Models
Current State Initiatives
The Kansas Hospital Association is promoting “Primary Health Centers” to shift small rural hospitals away from a focus on admissions to more outpatient and transitional services. They are proposing two alternative models, both of which would be open 365 days a year, but one for 12 hours/day and the other 24 hours/day. Such a model will require changes in state licensing requirements to authorize this new provider type and changes in Medicare reimbursement policies.23
The Oregon Rural Health Reform Initiative is an effort to sustain rural hospitals financially by transitioning them away from a cost-based reimbursement model. Instead, rates at these rural hospitals will be negotiated with local coordinated care organizations, under the oversight of the Oregon Health Authority (OHA). Currently, OHA is working to determine which hospitals will remain financially viable should they shift to a coordinated care payment model, and which hospitals should continue to operate with cost-based reimbursement.24
National Initiatives
The Medicare Payment Advisory Commission (MedPAC) Proposal offers two possible models designed to preserve access to health services in rural areas while eliminating the financial burden of maintaining an acute inpatient care facility. In the first model, struggling hospitals would maintain their ED 24/7 and would also continue to provide outpatient services. Hospitals would be reimbursed by a PPS rate per service and would also receive a fixed grant to help offset standby costs. The second option involves hospitals transitioning to a primary care clinic or FQHC-like model that would be open between 8 and 12 hours per day, along with ambulance services that would be available at all times. These hospitals would also be reimbursed by a PPS rate per service and would receive a fixed grant to help fund the “ambulance standby capacity” as well as any other uncompensated care costs.25
The REACH Act (Rural Emergency Acute Care Hospital Act), introduced by Senators Charles Grassley (R-IA) and Cory Gardner (R-CO), would create a new Medicare payment designation called a Rural Emergency Hospital (REH), to sustain emergency care in rural communities. The new designation is aimed at addressing the difficulty that CAHs may have in achieving occupancy rates high enough to keep their inpatient beds, and thus the hospitals themselves, open. REHs would provide only 24/7 emergency care, observation care, and outpatient services (which could include telehealth services), as well as ambulance services to transport patients who need a higher level or care or inpatient admission to larger regional medical centers; REHs would not operate any acute-care inpatient beds themselves. CAHs and other small rural hospitals (<50 beds) that meet these criteria would be eligible for the designation. The idea is that these hospitals would likely be more financially viable without an inpatient center and could instead focus solely on stabilizing and transporting patients to larger regional medical centers, while continuing to receive the benefit of higher Medicare reimbursement rates.26
The Save Rural Hospitals Act introduced by Representative Same Graves (R-MO) would reverse sequester cuts made to CAHs and small rural hospitals, and also seek to preserve or increase federal payments for low-volume and Medicare-dependent hospitals. Among other provisions, the Graves proposal delays penalties for small rural hospitals that have failed to transfer to an electronic health record system, and also increases Medicare payments for ground ambulance services in rural areas.27
Conclusion
The number of rural hospital closures has increased significantly in recent years. This trend is expected to continue, raising questions about the impact the closures will have on rural communities’ access to health care services. Both the examination of rural hospital closures in three communities as well as interviews with national experts show that a number of factors contribute to rural hospital closures, including demographics (aging, poor, and declining populations), hospital finances (high uninsured rates and high shares of public paying patients), and overall changes in how care is delivered. This research also revealed that the hospital closures reduced local residents’ access to care (especially emergency care), led to an outmigration of health care professionals, and worsened pre-existing challenges in obtaining access to specialty care. Although some communities were able to adapt to fill in gaps in primary care post-closure, elderly and low-income individuals were more likely to face transportation challenges and thus more likely to delay or forgo needed care. The experience of study hospitals, stakeholder interviews, and other research show that a state’s decision about the Medicaid expansion has an important impact on hospital revenues and access to care, but the sustainability of rural hospitals depends on a broader set of factors. Looking ahead, new models of health care delivery, along with new models of payment and financing, may be better able than current admissions- and volume-driven systems to support the needs of rural communities. Such reconfiguration may require federal support and assistance as well as regional planning efforts.
This issue brief was prepared by Jane Wishner and Patricia Solleveld from the Urban Institute and Julia Paradise, Robin Rudowitz and Larisa Antonisse from the Kaiser Family Foundation’s Commission on Medicaid and the Uninsured (KCMU). The authors thank John Holahan from the Urban Institute for his comments on drafts of this brief. They also express their appreciation to individuals who were interviewed for this report. Their expertise and insights were invaluable to this project.
Appendix
Description of Selected Hospitals
Marlboro Park Hospital – Bennettsville, South Carolina
Marlboro Park Hospital stopped admitting patients on April 25, 2015 and transferred all its remaining patients to nearby Chesterfield General Hospital in Cheraw, South Carolina, approximately 15 miles away.28 Both hospitals were owned by a real estate trust and had been operated by Community Health Systems (CHS), which announced in 2014 that it would not renew the leases for either hospital when they expired on April 30, 2015. McLeod Health Systems, a South Carolina system, assumed operation of Chesterfield General Hospital and renamed it McLeod Health Cheraw, but it declined to operate Marlboro Park. According to the South Carolina Department of Health and Human Services, Marlboro Park Hospital lost nearly $35 million between 2009 and 2013 – more than any other hospital in South Carolina, while Chesterfield generated an $8.5 million profit during those same years. Currently, some residents of Bennettsville receive care at McLeod Health Cheraw, while others travel to one of the two hospitals in Florence, South Carolina (approximately 40 miles away by car) and Scotland Memorial Hospital in Laurinberg, North Carolina (approximately 17 miles away by car).
Mercy Hospital – Independence, Kansas
Mercy Hospital, part of the Mercy Health System, began a phased closure on October 10, 2015. In 2014, the hospital formed a task force to consider an affiliation with the Coffeyville Regional Medical Center, but those discussions ended after the hospitals were unable to reach an agreement. The nearest hospitals are now 16 minutes away in Neodesha and 20 miles away in Coffeyville (the Coffeyville hospital is now the only hospital in Montgomery County).
Parkway Regional Hospital – Fulton, Kentucky
After serving one of the poorest counties in western Kentucky for over two decades, Parkway Regional Hospital closed its emergency department and 70-bed inpatient hospital in Fulton, Kentucky in March, 2015. Two nearby hospitals in Union City and Martin, Tennessee competed with Parkway Regional for many of the same patients.29 Fulton residents who had private insurance or could afford the cost typically left Fulton to seek care, primarily at Tennova Healthcare – Volunteer Martin, a 100-bed hospital only 12 miles away in Martin, Tennessee. Community Health Systems (CHS), the owner of Parkway Regional, also operates the hospital in Martin and promoted use of that Tennessee facility, including for specialty care, both before and after the closure of Parkway Regional. The closest Kentucky hospital is Jackson Purchase Medical Center (operated by LifePoint Health) in Mayfield, Kentucky – 22 miles from the town of Fulton. Some Fulton County residents received care at Jackson Purchase before the closure, including women who went there for labor and delivery services.
Appendix Table 1: Characteristics of Study Communities Compared to State and U.S. Overall, 2014
Table 1: Characteristics of Select Communities Compared to State and U.S. Overall, 2014
U.S Overall
Kentucky
Fulton County, KY
Population
318,857,056
4,413,457
6,265
Percent Change in Population (2010-2014)
3.3%
1.7%
-8.4%
Age
Under 18
23.1%
22.9%
21.0%
Over 65
14.5%
14.8%
19.4%
Race/ethnicity
White, single race
77.4%
88.3%
72.4%
Black, single race
13.2%
8.2%
24.3%
Hispanic or Latino
17.4%
3.4%
1.5%
Poverty Rate
14.8%
19.1%
31.2%
Median Household Income (2010-2014)
$53,482
$43,342
$32,948
National
South Carolina
Marlboro County, SC
Population
318,857,056
4,832,482
27,924
Percent Change in Population (2010-2014)
3.3%
4.5%
-3.5%
Age
Under 18
23.1%
22.4%
20.7%
Over 65
14.5%
15.8%
15.2%
Race/ethnicity
White, single race,
77.4%
68.3%
42.1%
Black, single race
13.2%
27.8%
51.0%
Hispanic or Latino
17.4%
5.4%
3.2%
Poverty Rate
14.8%
18.0%
31.4%
Median Household Income (2010-2014)
$53,482
$45,033
$28,765
National
Kansas
Montgomery County, KS
Population
318,857,056
2,904,021
34,065
Percent Change in Population (2010-2014)
3.3%
1.8%
-4.0%
Age
Under 18
23.1%
24.9%
23.9%
Over 65
14.5%
14.3%
18.1%
Race/ethnicity
White, single race
77.4%
86.8%
85.2%
Black, single race
13.2%
6.3%
5.8%
Hispanic or Latino
17.4%
11.4%
6.3%
Poverty Rate
14.8%
13.6%
18.0%
Median Household Income (2010-2014)
$53,482
$51,872
$40,716
SOURCE: All estimates are from the Census Bureau’s 2014 QuickFacts. QuickFacts provides statistics for all states and counties and for cities and towns with a population of 5,000 or more. http://www.census.gov/quickfacts/table/PST045215/00
Ibid. Rural Referral Centers (RRCs) may also be classified as Medicare Dependent Hospitals (MDHs) or Sole Community Hospitals (SCHs). The percentages given for MDHs and SCHs refer to hospitals that have only those designations and are not also RRCs. As explained by Freeman, Thompson, et al., “[t]hese payment programs [CAHs, MDHs, SCHs and RRCs] recognize the challenges of providing care in rural settings and provide enhanced or supplemental reimbursement. Qualifications for these programs are complex and may include locations, hospital size, staffing, network agreements, patient demographics including insurance, and patient referral patterns.” ↩︎
The North Carolina Rural Health Research Program defines a rural hospital as “any short-term, general acute, non-federal hospital” that is either: (a) not located in a metropolitan county; (b) located in a Rural-Urban Commuting Area Code (RUCA) type 4 or higher; or (c) a Critical Access Hospital. For a list of the hospitals and more information about the project, see http://www.shepscenter.unc.edu/programs-projects/rural-health/rural-hospital-closures/↩︎
While our interviews did not address what type of mental health and substance use incidents led people to the emergency departments of these hospitals, rural communities are facing significant challenges with the current opioid epidemic. See Toliver, Z. The Opioid Epidemic: Testing the Limits of Rural Healthcare. (The Rural Monitor, Rural Health Information Hub, May 18, 2016). https://www.ruralhealthinfo.org/rural-monitor/opioid-epidemic/↩︎
All three of our case studies involved hospitals that were located close to a state border. The ability of Medicaid patients to access care across state lines may depend on state rules and Medicaid managed care contracts and networks even if a provider in another state is the closest provider. ↩︎
MENLO PARK, Calif., – At a time of growing dialogue about transgender people and issues, the impact of HIV on the community has been largely absent. Transgender women are among those at highest risk for HIV today. The CDC estimates that one in four trans women in the U.S. is living with HIV, and among Black trans women it is one in two.
In response to these overwhelming statistics and the vulnerability of trans women, Greater Than AIDS is launching a new video series that gives voice to transgender women to share their own narrative about HIV, both the impact and response that is needed.
Produced by the Kaiser Family Foundation and the UCSF Center of Excellence in Transgender Health, with funding from ViiV Healthcare’s Positive Action Programme, Empowered: Trans Women & HIV confronts the social stigma facing many transgender women and promotes actions to improve health and well-being.
“We’ve come a long way. We don’t have to live in the shadows anymore, but we still have more work to do. We are not yet where we need to be when it comes to HIV and its impact on trans women,” said JoAnne Keatley, MSW, Director, UCSF Center of Excellence for Transgender Health, who appears in and advised on the campaign. “With this video series, we take a huge step forward as a community in bringing these issues into the light.”
Anchored by an intimate and inspiring conversation, a diverse group of trans women, including some living with HIV and others who are not, share challenging moments of diagnosis, disclosure, discrimination, and the loss of close friends, as well as triumphs of finding gender-affirming health care providers, learning about PrEP and transitioning safely while on HIV treatment.
“This campaign is a wake-up call to the health care community about the need for gender-affirming care and services when it comes to addressing the high rates of HIV among trans women,” said Tina Hoff, Senior Vice President, Media Partnerships & Health Communications, Kaiser Family Foundation. “Preventing and treating HIV should not stand in the way of living as one’s true authentic self.”
“The campaign supports trans women in a way that’s meaningful to them and makes sure those important issues connected to their well-being, including HIV, can be explained and discussed candidly. As a company, we are proud to support this innovative programme which gives voice to trans women, as an important part of our commitment to all people at risk or affected by HIV.” said Michael Joyner, Director, Positive Action for MSM and Transgender Programme.
The campaign will be featured at the upcoming International AIDS Conference in Durban, South Africa (July 18-22), which for the first time includes a Trans pre-conference (July 17).
Greater Than AIDS is a leading public information response focused on the U.S. HIV/AIDS epidemic from the Kaiser Family Foundation. Through targeted media campaigns and community outreach, Greater Than AIDS and its partners work to increase knowledge and fight stigma, while promoting direct actions to reduce the spread of HIV.
About Kaiser Family Foundation
The Kaiser Family Foundation, a leader in health policy analysis, health journalism and communication, is dedicated to filling the need for trusted, independent information on the major health issues facing our nation and its people. The Foundation is a non-profit private operating foundation based in Menlo Park, California.
About UCSF Center of Excellence for Transgender Health
The Center of Excellence for Transgender Health works to improve the overall health and well-being of transgender individuals by developing and implementing programs in response to community-identified needs. The CoE combines the unique strengths and resources of a nationally renowned training and capacity-building institution, the Pacific AIDS Education and Training Center (PAETC), and an internationally recognized leader in HIV prevention research, the Center for AIDS Prevention Studies (CAPS), both of which are housed at the University of California San Francisco.
About ViiV Healthcare’s Positive Action Programme
Positive Action works with those communities most vulnerable to HIV disease, including youth, girls and women, sex workers, gay men, men who have sex with men (MSM), transgender people, injecting drug users (IDU), the homeless and the incarcerated. Our projects range across education, prevention, care and treatment-related activity such as treatment literacy and community/clinical engagement.
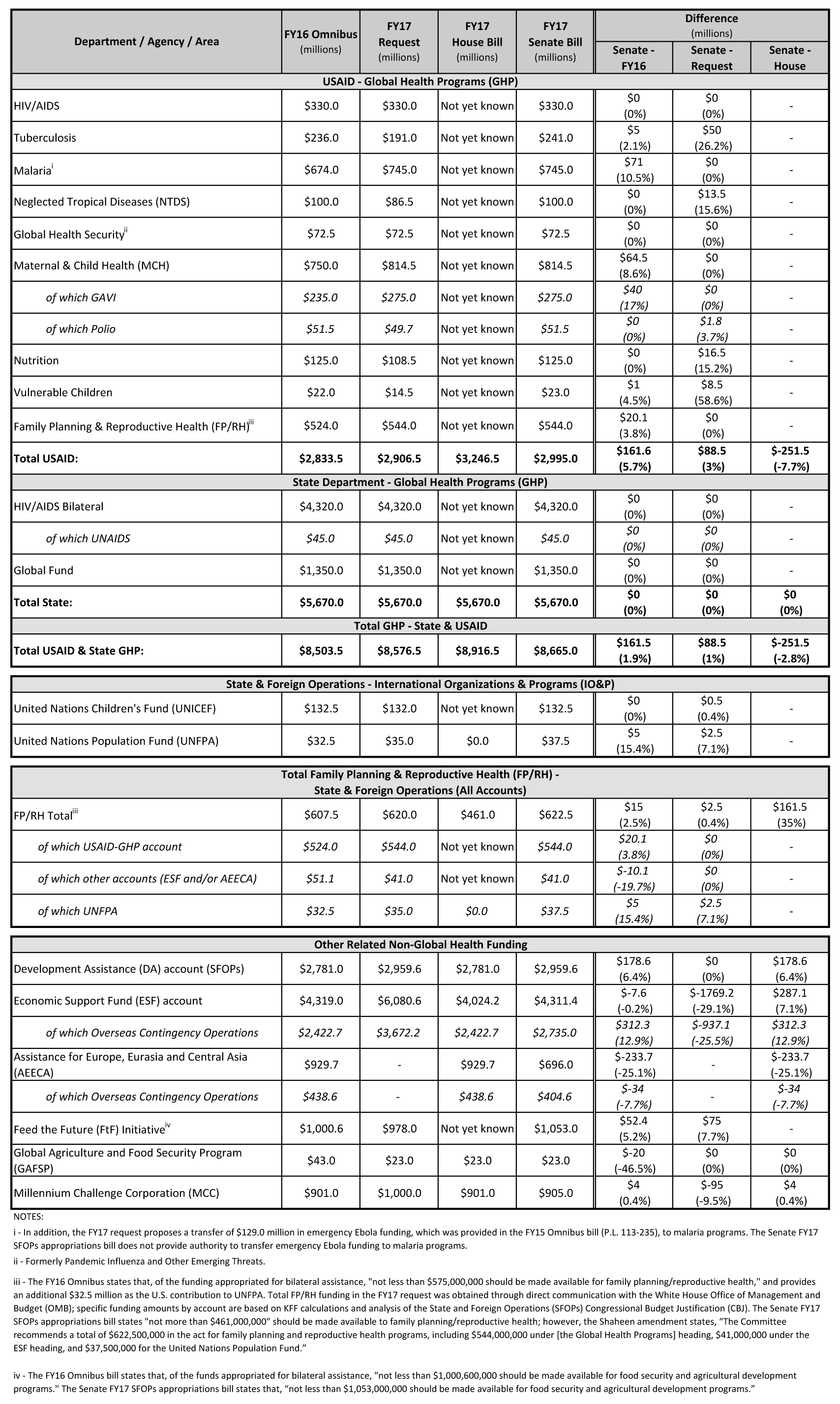
The Senate Appropriations Committee approved the FY 2017 State and Foreign Operations Appropriations bill on June 29, 2016, which includes funding for U.S. global health programs at the U.S. Agency for International Development (USAID) and the State Department (see table below) comprising a significant portion of U.S. funding for global health (total funding for global health is not currently known as some funding provided through USAID, HHS, and DoD is not yet available).
A press release from the committee states that funding in the bill for global health would total $8.67 billion, which is $89 million (1%) above the President’s request and $162 million (2%) above the FY 2016 enacted level, but $252 million below (-3%) the House SFOPs appropriations bill .
Funding for bilateral HIV programs as part of the President’s Emergency Plan for AIDS Relief (PEPFAR) matches the President’s request as does funding for the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), maternal and child health (MCH), family planning and reproductive health (FP/RH), global health security, and malaria (although, the Senate bill does not provide authorization to transfer emergency Ebola funding to malaria programs as was included in the President’s request). Funding for tuberculosis, neglected tropical diseases (NTDs), nutrition, and vulnerable children would increase compared to the President’s request.
The tables below compare U.S. global health funding in the FY 2017 State and Foreign Operations Appropriations bill to the FY 2016 enacted levels and the President’s FY 2017 Budget Request.
Majorities Across Party Lines Support Investing More Money in Zika Research and Preventing the Virus’ Spread
Two Thirds of Republicans Want Congress to Repeal the Affordable Care Act, but They Are Divided on Whether to Replace It with a GOP-Sponsored Alternative
Democrats More Favorable to ACA in June, Leading to 44% Unfavorable, 42% Favorable Overall Split
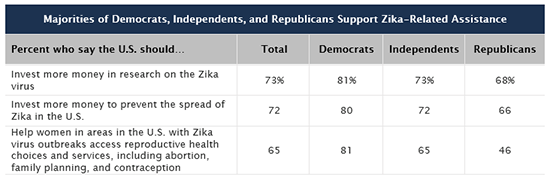
Majorities of the public say the United States should invest more money in Zika research and in preventing its spread in this country, the latest Kaiser Health Tracking Poll finds. More than seven in 10 people, including majorities of Democrats, Republicans, and independents, say they support investing in Zika research and to prevent its spread.
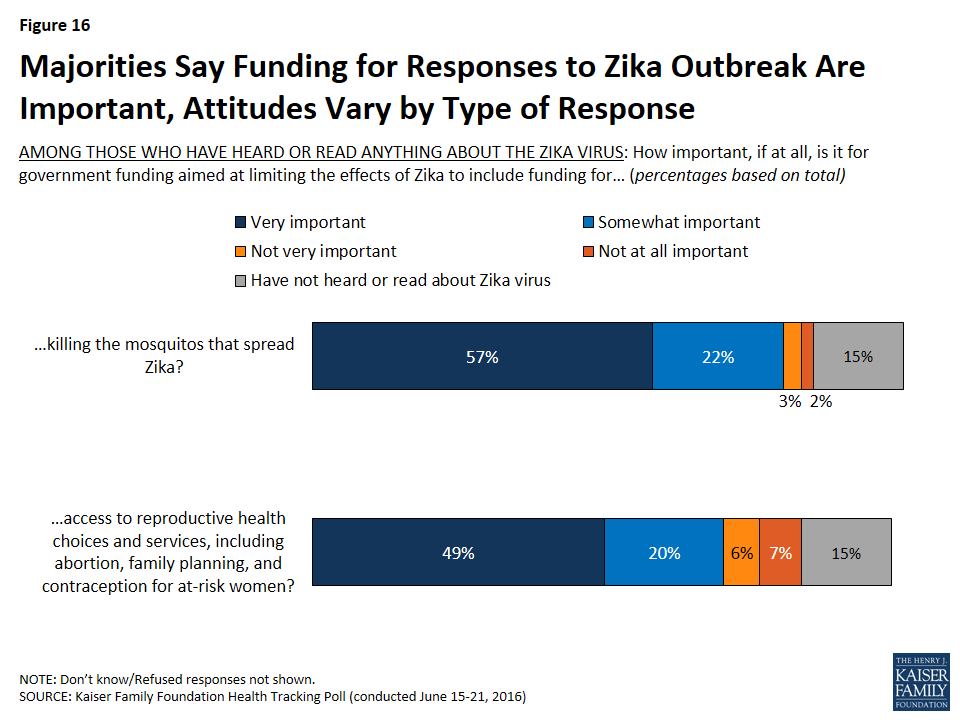
About two thirds of the public also support helping women in Zika-affected areas in the U.S. with reproductive health choices and services, which can be important because the virus can be sexually transmitted and has been linked to severe birth defects in babies born to infected mothers. This includes majorities of Democrats and independents, and nearly half of Republicans.
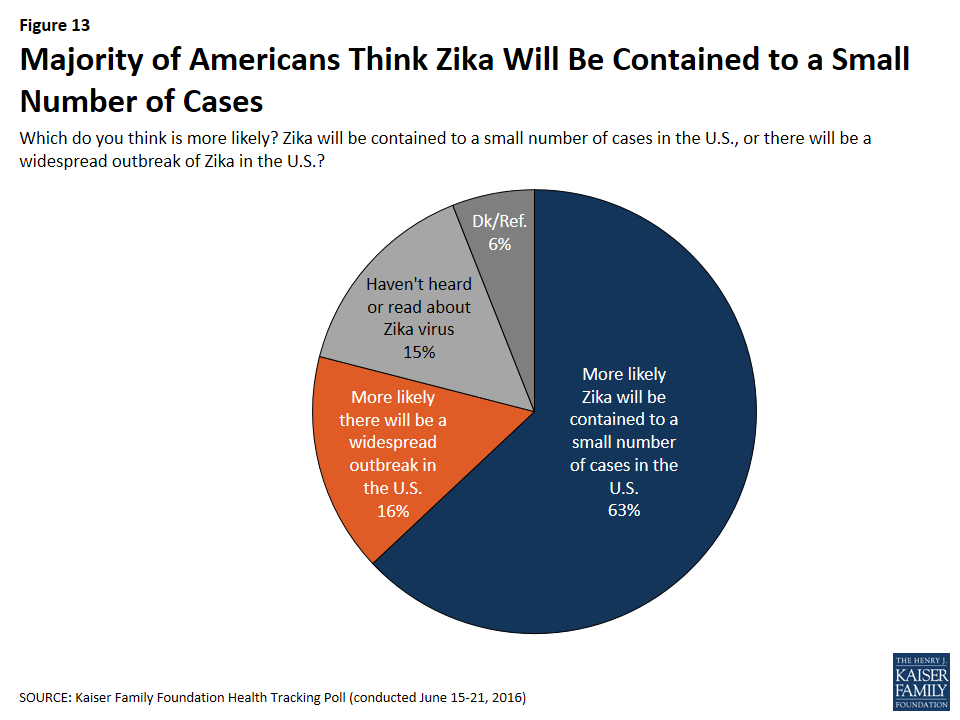
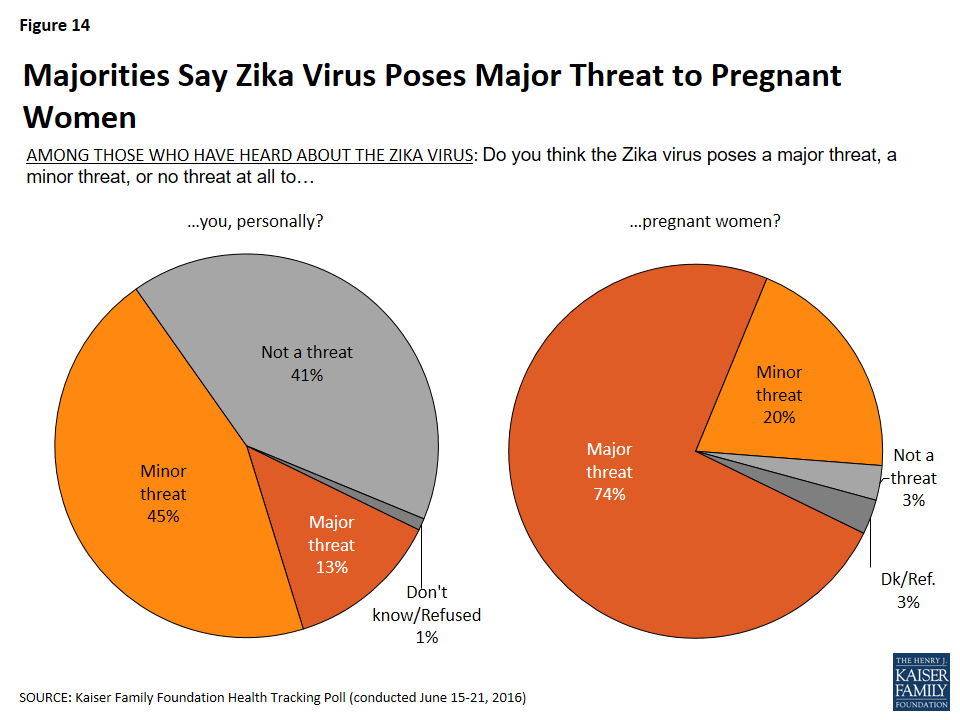
The poll finds most Americans (85%) have read or heard about the Zika virus. Of this group, relatively few (13%) say that the Zika virus poses a major threat to them personally, while three in four (74%) say the Zika virus poses a major threat to pregnant women.
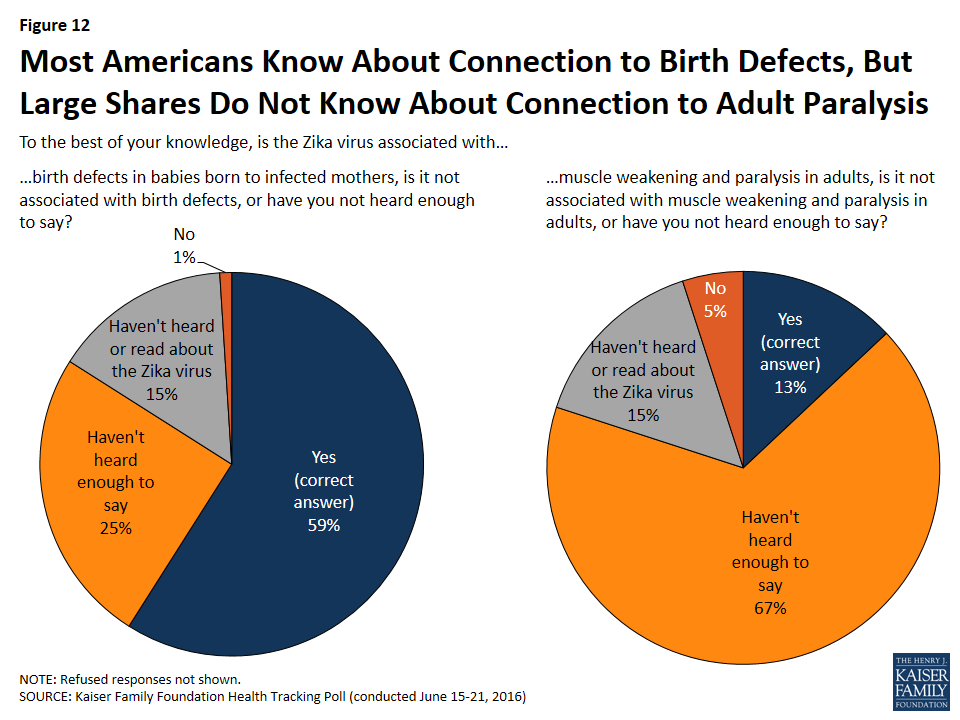
These perceptions may reflect the public’s uneven awareness about the virus. While about six in 10 (59%) correctly say that the Zika virus is associated with birth defects in babies born to infected mothers, far fewer (13%) know the virus is associated with muscle weakening and paralysis in adults, and only half are aware the virus can be sexually transmitted.
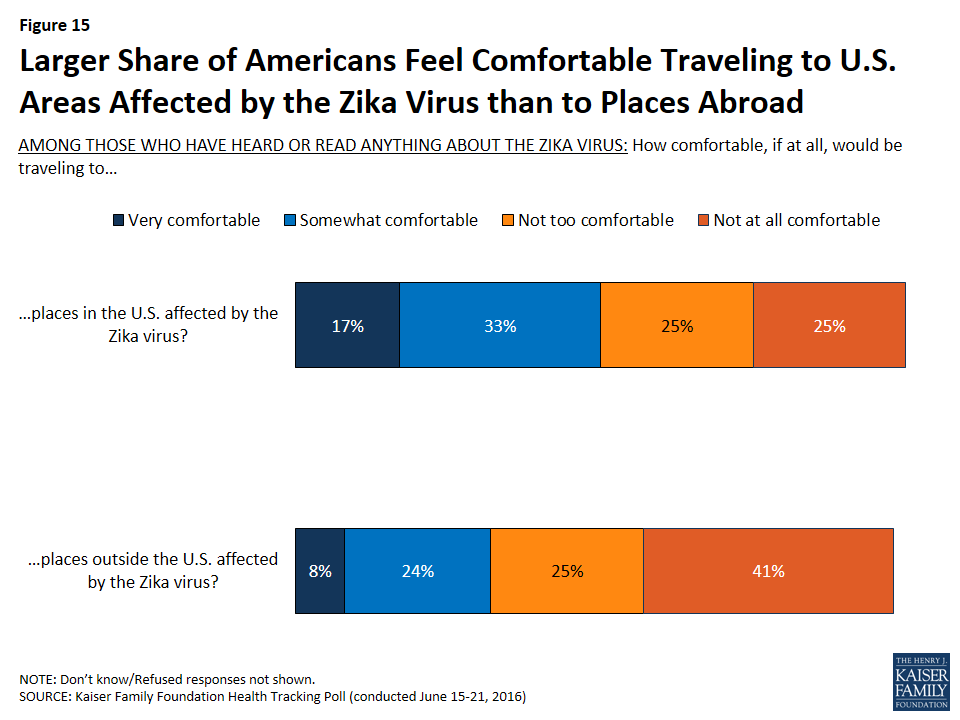
With the virus already widespread in Latin America and the Caribbean, including Rio where the 2016 Summer Olympics will be held, the survey finds that one third of the public (32%) says they would be comfortable traveling to Zika-infected areas outside the U.S.
On the Affordable Care Act (ACA), Democrats moved towards more positive views as the presidential primary season ended, with 71 percent of Democrats reporting a favorable view in June compared to 63 percent in April, and a smaller share holding unfavorable views (16% vs. 25%). As a result, the public this month is almost evenly divided in its overall view of the law, with 44 percent holding unfavorable views and 42 percent holding favorable ones
The public is also split on what they want Congress to do next with the law. About as many people say they want the entire law repealed (33%) or scaled back (11%) as say they want the law expanded (28%) or implemented as is (17%). There are huge partisan divisions on this question, with two thirds of Republicans (66%) wanting to repeal the law entirely, and nearly half of Democrats wanting to expand it (48%).
Those who favor repeal are divided about whether it should be replaced with a Republican-sponsored alternative. This is also true for Republicans, with about three in 10 Republicans (29%) saying that they would like to see the law repealed and then replaced with a Republican alternative, and one quarter saying they would like to see it repealed and not replaced (25%).
The poll also explores how people experience health care costs, including premiums, deductibles, and drug costs.
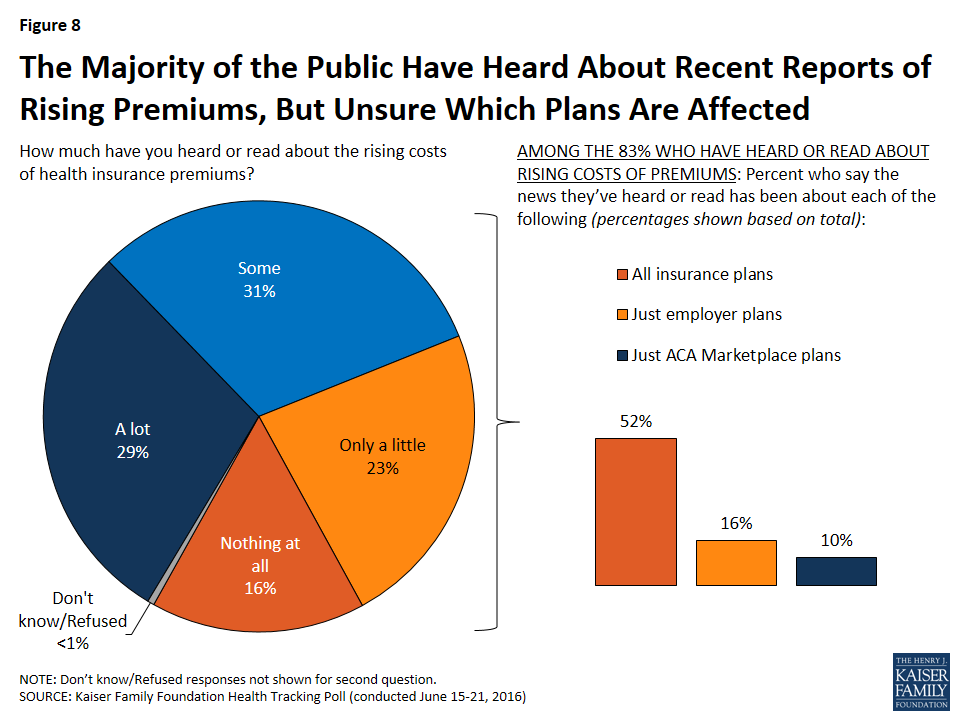
Large majorities of the public say they have heard or read news about the rising costs of health insurance premiums. However, while those reports have mostly been about marketplace premiums, people are uncertain about who and which plans are affected. Half (52%) say the reports have been about all insurance plans, 16 percent say the reports have been about just employer-sponsored plans, and one in ten (10%) say the news has only been about ACA marketplace plans.
Designed and analyzed by public opinion researchers at the Kaiser Family Foundation, the poll was conducted from June 15-21 among a nationally representative random digit dial telephone sample of 1,201 adults. Interviews were conducted in English and Spanish by landline (420) and cell phone (781). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
Current attitudes about the ACA are divided, with 44 percent expressing an unfavorable opinion and 42 percent reporting a favorable opinion; 16 percent of Democrats report an unfavorable opinion, down from 25 percent in April.
Increases in the amount people pay for their health insurance premiums tops health care costs concerns; premiums and deductibles are the biggest financial burdens.
A majority of Americans are following the news about rising health insurance premiums, but the public doesn’t differentiate reports about ACA marketplace premiums from private insurance premiums overall.
While the majority of Americans have heard about the Zika virus, only about one in ten (13 percent) know about the impact the virus can have on adults and only half are aware the virus can be sexually transmitted.
There is widespread support for Zika-related assistance including funding for research, funding for preventing the spread of Zika, and helping women in areas in the U.S. with Zika virus outbreaks access reproductive health choices and services, including abortion, family planning, and contraception.
The Current News and Political Environment
The June Kaiser Health Tracking Poll examines the role of the major health policy news stories in the current news and political environment. In addition, it provides an in-depth analysis of two of the biggest health policy stories: the Zika virus outbreak and the rising costs of ACA health insurance premiums.
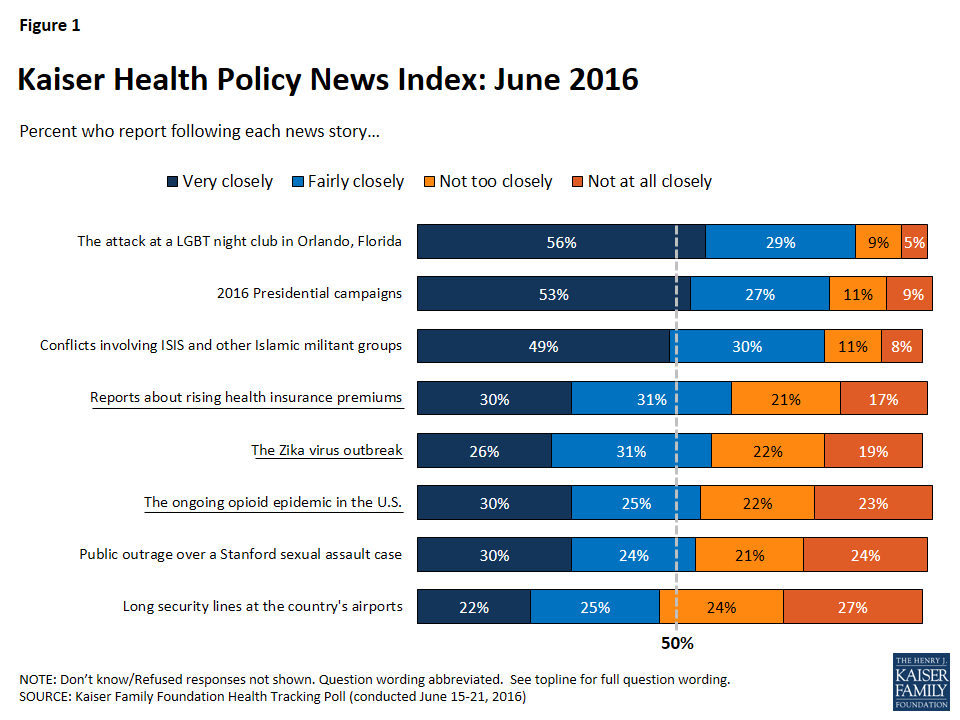
Kaiser Health Policy News Index: June 2016
This month’s tracking poll finds a large majority of Americans closely following news stories about the attack at a LGBT night club in Orlando, Florida (85 percent), the 2016 presidential campaigns (80 percent), and conflicts involving ISIS and other Islamic militant groups (79 percent). The top health stories during the month of June, both closely followed by about six in ten Americans, are the rising costs of health insurance premiums (61 percent) and the Zika virus outbreak (57 percent). In addition, 55 percent of Americans report following news about the ongoing opioid epidemic closely, similar to the share who report closely following outrage over the sentencing in a Stanford sexual assault case (54 percent). Finally, during the summer travel season, nearly half of Americans report closely following news about the long security lines at the country’s airports (47 percent).
Figure 1: Kaiser Health Policy News Index: June 2016
Rising Health Insurance Premiums and the Impact of Health Care Costs on Families
Over the past month, one of the major health policy stories involves reports that health insurance premiums under the Affordable Care Act (ACA) may be increasing in 2017. This month’s tracking survey examines overall perceptions of the 2010 health care law and the impact that the rising costs may have on health care consumers.
The ACA and Health Care Costs
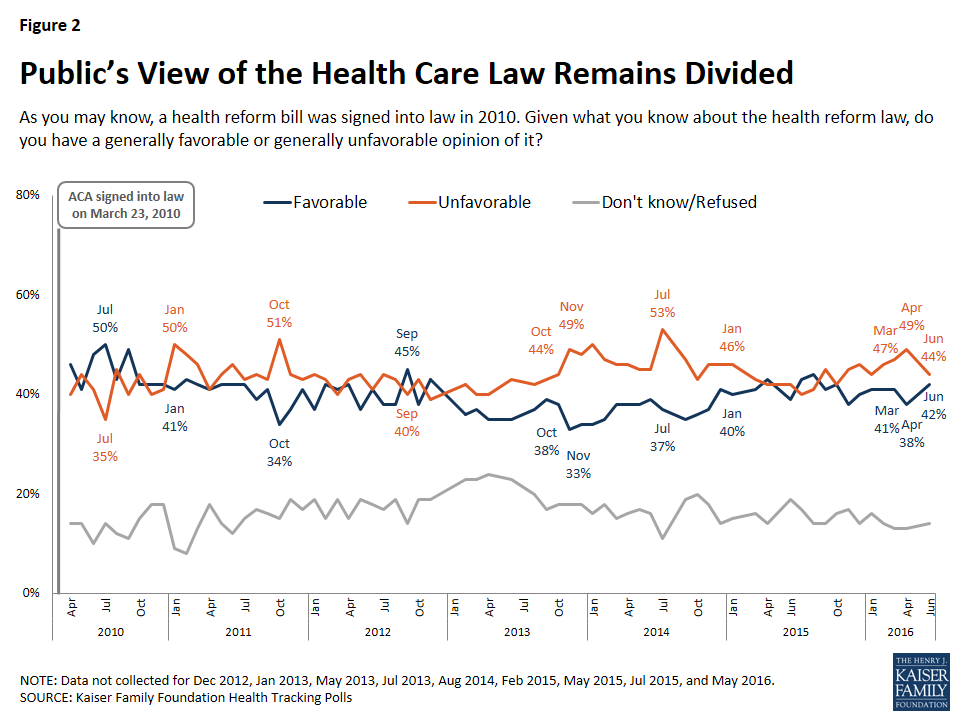
With rising health care costs on the minds of Americans, this month’s poll finds divided public opinion of the Affordable Care Act. The gap between favorable and unfavorable opinions narrowed nine percentage points between April and June, with the share of the public with an unfavorable opinion decreasing slightly from 49 to 44 percent and the share with a favorable opinion increasing slightly from 38 to 42 percent.
Since April, there has been a slight shift in favorability among Democrats, while attitudes among Republicans and independents have remained largely stable. Seven in ten Democrats (71 percent) now report a favorable opinion of the law, up from 63 percent in April. In addition, the most recent survey finds that 16 percent of Democrats report an unfavorable opinion, down from 25 percent in April.
Figure 2: Public’s View of the Health Care Law Remains Divided
Next Steps for the ACA
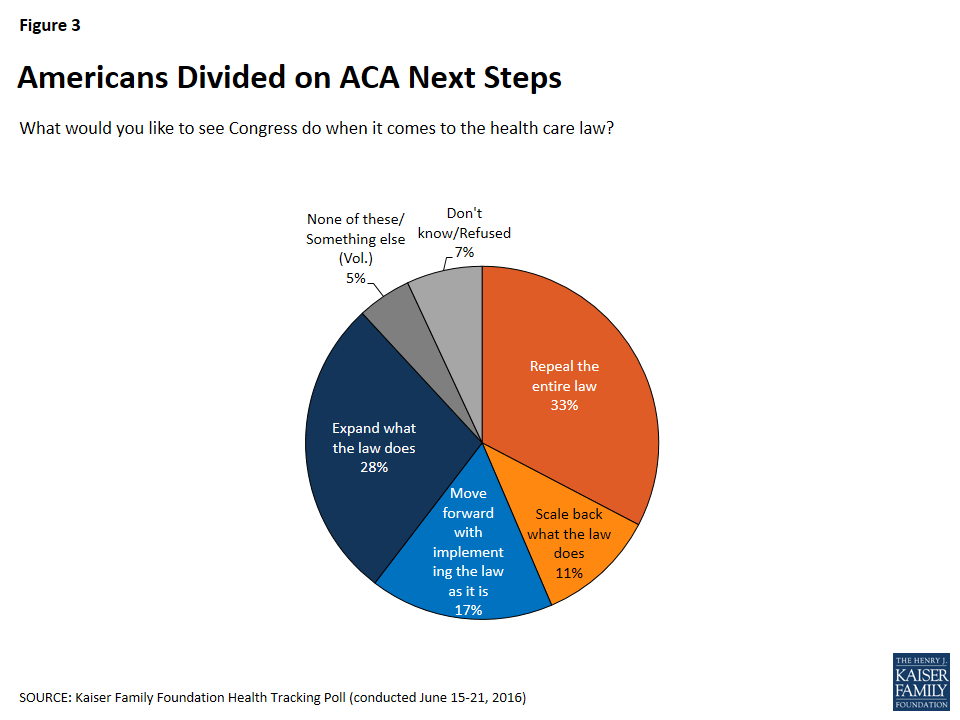
On June 22nd, House Republicans unveiled a conservative alternative to the Affordable Care Act.1 Overall, 33 percent of Americans want the law repealed, three in ten (28 percent) want to expand what the law does, one in five (17 percent) want to move forward with implementing the law as is, and about one in ten (11 percent) want to scale back what the law does.
Figure 3: Americans Divided on ACA Next Steps
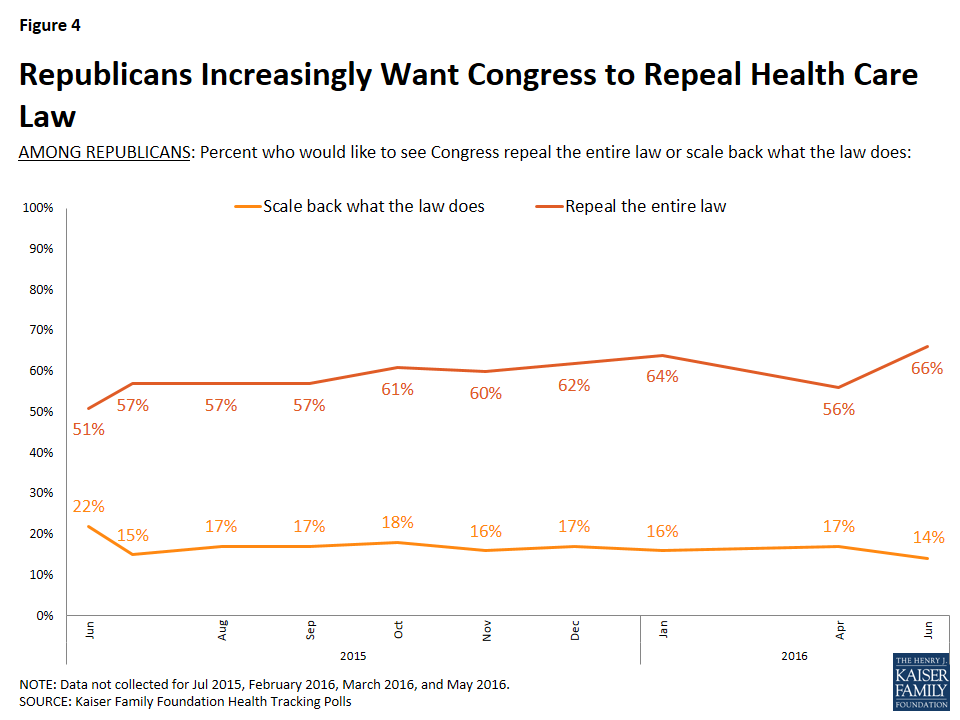
Two-thirds of Republicans would like to see Congress repeal the entire 2010 health care law, up from 51 percent, 12 months ago. In contrast, this month’s poll finds that half of Democrats (48 percent) say they’d like to see Congress expand what the law does.
Figure 4: Republicans Increasingly Want Congress to Repeal Health Care Law
However, Republicans who want to see the law repealed are split on whether there should be a Republican-sponsored replacement for the law or not, with about three in ten Republicans reporting that they would like to see the law repealed and then replaced with a Republican alternative (29 percent) and one-quarter saying they would like to see it repealed and not replaced (25 percent).
Figure 5: Republicans Who Want ACA Repealed Split On Whether It Should Be Replaced With Republican-Sponsored Alternative
Health Insurance Premiums
Among the insured, similar shares — about one in five — say the greatest financial burden of their own health care costs are the deductibles they pay before their insurance kicks in (21 percent) and their health insurance premiums (20 percent). One in ten say the cost of prescription drugs is the greatest financial burden (12 percent), 6 percent say it is doctor visits, and 31 percent say that paying for health care and health insurance is not a financial burden.
Figure 6: Financial Burden Of Health Care Costs Among Insured
Overall, nearly nine in ten (88 percent) Americans say they are concerned about increases in the amount people pay for their health insurance premiums. This is followed closely by the percent who are concerned about increases in the costs of deductibles (85 percent), increases in what the nation as whole spends on health care (83 percent), and increases in prescription drug costs (82 percent). Fewer but still large majorities of insured Americans are concerned about increases in spending on government health insurance programs (74 percent) and increases in the amount employers pay for their employees’ premiums (71 percent).
Figure 7: Health Insurance Premiums Top Concerns Among Health Care Costs
Recent News About Rising Costs of ACA Marketplace Premiums
Despite the fact that 83 percent of the public say they have heard or read recent news about rising costs of health insurance premiums, individuals are uncertain about who and which plans are affected. Half of individuals (52 percent) say the reports have been about all insurance plans, 16 percent say the reports have been about just employer-sponsored plans, and one in ten say the news has only been about ACA Marketplace plans.
Figure 8: The Majority of the Public Have Heard About Recent Reports of Rising Premiums, But Unsure Which Plans Are Affected
The Zika Virus Outbreak
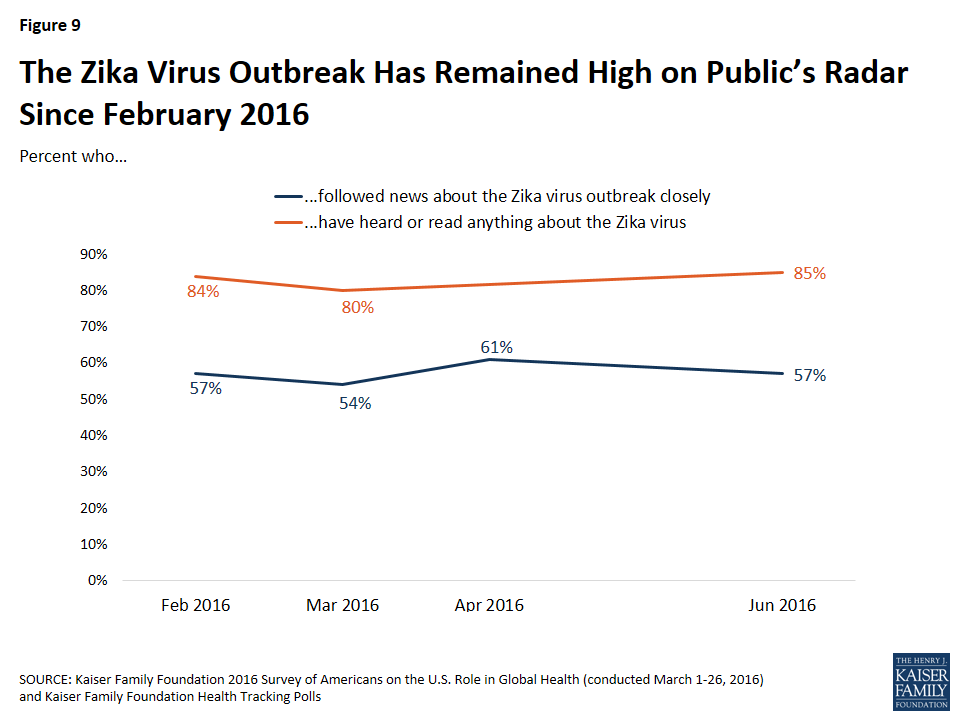
Due to ongoing developments about the potential threats of the Zika virus, concerns over the 2016 Summer Olympics, and congressional debate over funding allocation to limit the effects of the virus in the United States, the Zika virus outbreak was one of the most reported health policy stories during the month of June. The Zika virus outbreak has remained on the public’s radar since earlier this year,2 with more than half of Americans consistently reporting that they are closely following news about Zika and a large majority regularly saying they have heard or read about it.
Figure 9: The Zika Virus Outbreak Has Remained High on Public’s Radar Since February 2016
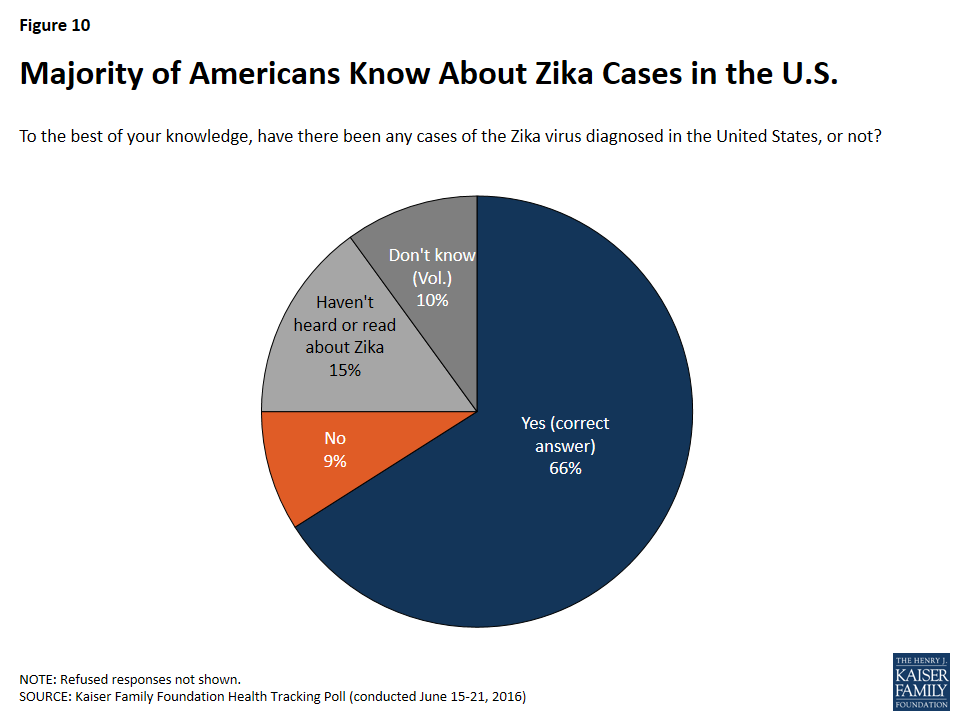
According to the Centers for Disease Control and Prevention (CDC),3 there have been over 750 confirmed cases of the Zika virus across 45 states and Puerto Rico since January 2015. The June tracking survey finds that two-thirds of Americans are aware there have been cases of the Zika virus diagnosed in the U.S.
Figure 10: Majority of Americans Know About Zika Cases in the U.S.
Overall Knowledge on Transmission of the Virus and Potential Impacts
There are mixed results when examining the public’s awareness of the ways the virus spreads and its potential effects. Eight in ten Americans are aware that the Zika virus can be spread through a bite of an infected mosquito (79 percent) and are aware that it does not appear to be spread through shaking hands with an infected person (79 percent). However, fewer – half (49 percent) – are aware that a person can become infected by having sex with someone who is infected.
Figure 11: Vast Majorities of Americans Knowledgeable About Spread of Zika, Fewer When it Comes to Sexual Transmission
Americans are more likely to be aware of the connection between the Zika virus and birth defects than the potential impacts of the virus on adults. Six in ten Americans are aware that the Zika virus is associated with birth defects in babies born to infected mothers (59 percent), with one-fourth reporting that they haven’t heard enough to say, 15 percent reporting they haven’t heard or read about the virus, and one percent saying the virus is not associated with birth defects. Only one in ten Americans are aware that the Zika virus is associated with muscle weakening and paralysis in adults (13 percent), while two-thirds haven’t heard enough to say (67 percent), 15 percent haven’t heard or read about the virus, and 5 percent say the virus is not associated with muscle weakening and paralysis in adults.
Figure 12: Most Americans Know About Connection to Birth Defects, But Large Shares Do Not Know About Connection to Adult Paralysis
Most Americans Do Not See The Zika Virus as a Personal Health Threat
Most Americans aren’t too concerned in general about Zika in the U.S., although there are some concerns about the threat the virus poses to pregnant women. Overall, the majority of Americans (63 percent) think Zika will be contained to a small number of cases in the U.S. rather than a widespread outbreak (16 percent), and of those who have heard or read anything about the virus, only 13 percent say they think the Zika virus poses a major threat to them personally, while almost equal shares say it poses a minor threat (45 percent) or not a threat at all (41 percent).
Figure 13: Majority of Americans Think Zika Will Be Contained to a Small Number of Cases
Despite this, three-fourths of Americans who have heard or read anything about the virus say the Zika virus poses a major threat to pregnant women (74 percent), with an additional 20 percent who say it poses a minor threat and only 3 percent who believe it does not pose a threat.
Figure 14: Majorities Say Zika Virus Poses Major Threat to Pregnant Women
Hispanics More Likely to Perceive the Zika Virus as a Threat
The perceived personal threat posed by the virus differs dramatically by ethnicity, with almost one-third of Hispanic individuals who have heard or read anything about the virus saying the Zika virus poses a major threat to them personally, compared to about one in five Blacks (21 percent) and only 7 percent of whites. Hispanics are also more likely to report being worried about the potential effects of the Zika virus. More than half of Hispanics who have heard or read anything about the virus say they are worried that they or someone in their family will be affected by the virus, 43 percent are worried the U.S. will see a large number of Zika-related cases, and one-third are worried that the upcoming Summer Olympics will lead to an increase in Zika-related cases. Across all of these measures, a larger share of Hispanics report being “very worried” than Blacks (36 percent, 27 percent, and 24 percent, respectively) and whites (10 percent, 16 percent, and 19 percent, respectively).
Table 1: Hispanics Are More Worried about the Zika Virus than Non-Hispanics
Among those who have heard or read anything about the virus, the percent who say:
Total
Hispanic
Black/Non-Hispanic
White/Non-Hispanic
They are very worried that they or someone in their family will be affected by the Zika virus
20%
52%
36%
10%
They are very worried that the upcoming Summer Olympics will cause an increase in the number of cases of the Zika virus
22
33
24
19
They are very worried that the U.S. will see a large number of cases of the Zika virus
21
43
27
16
The Zika virus poses a major threat to them personally
13
31
21
7
While Zika mainly threatens areas in the U.S. with warmer climates, there are only slight regional differences in overall concerns about the virus. However, there are differences based on whether an individual says there are a lot of mosquitos in their area during the summer. Slightly larger shares of individuals who say they live in areas with a lot of mosquitos report being worried about potential effects of the virus on themselves or their family members than individuals living in areas without a lot of mosquitos, 40 percent and 34 percent, respectively.
Figure 15: Larger Share of Americans Feel Comfortable Traveling to U.S. Areas Affected by the Zika Virus than to Places Abroad
The Impact of the Zika Virus on Travel Plans
Half of Americans who have heard or read anything about Zika say they would feel comfortable traveling to places in the U.S. affected by the Zika virus, with 17 percent saying they feel “very comfortable” and one-third saying they feel “somewhat comfortable.” This compares to one-third of Americans who would feel comfortable traveling to places outside the U.S. affected by the Zika virus – 8 percent say they are “very comfortable” and 24 percent say they are “somewhat comfortable.” In fact, four in ten Americans say they are “not at all comfortable” traveling to places outside the U.S. affected by the Zika virus (41 percent).
Widespread Support for Funding Aimed at Limiting the Effects of Zika
With legislation that would provide additional funding to combat the Zika virus stalled in Congress, the majority of Americans say it is important for government funding aimed at limiting the effects of Zika to include funding for both killing the mosquitos that spread the virus and access to reproductive health services for at-risk women. Nearly six in ten Americans it is “very important” to include funding for killing the mosquitos that spread Zika (57 percent), with an additional 22 percent saying it is “somewhat important.” Only 5 percent say it is “not very” or “not at all” important. In addition, a smaller share but still half of Americans say it is “very important” to include funding for access to reproductive services for at-risk women (49 percent), with an additional 20 percent saying it is “somewhat important.”
Figure 16: Majorities Say Funding for Responses to Zika Outbreak Are Important, Attitudes Vary by Type of Response
There are partisan differences in support for Zika-related funding, with Democrats and independents reporting higher levels of support than Republicans. Majorities of Democrats and independents say the U.S. should invest more money in research on the Zika virus, invest more money to prevent the spread of Zika, and help women in areas in the U.S. with Zika virus outbreaks access reproductive health services. It is worth noting that two-thirds of Republicans support investing more money in research on the virus and investing more money on preventing the spread of Zika in the U.S., but slightly less than half support helping women in areas in the U.S. with outbreaks of the virus access reproductive health services.
Table 2: Majorities of Democrats, Independents, and Republicans Support Zika-Related Assistance
Percent who say the U.S. should…
Total
Democrats
Independents
Republicans
Invest more money in research on the Zika virus
73%
81%
73%
68%
Invest more money to prevent the spread of Zika in the U.S.
72
80
72
66
Help women in areas in the U.S. with Zika virus outbreaks access reproductive health choices and services, including abortion, family planning, and contraception
65
81
65
46
Methodology
This Kaiser Health Tracking Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted June 15-21, 2016, among a nationally representative random digit dial telephone sample of 1,201 adults ages 18 and older, living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Computer-assisted telephone interviews conducted by landline (420) and cell phone (781, including 447 who had no landline telephone) were carried out in English and Spanish by Princeton Data Source under the direction of Princeton Survey Research Associates International (PSRAI). Both the random digit dial landline and cell phone samples were provided by Survey Sampling International, LLC. For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2014 American Community Survey (ACS) on sex, age, education, race, Hispanic origin, and region along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the January-June 2015 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.