Medicare Advantage Insurers Deny Prior Authorization Requests for Post Acute Care at Substantially Higher Rates Than the Overall Denial Rate
Prior authorization practices by health insurers have come under scrutiny in recent years, in part spurred by the public sentiment that delays and denials of care are a problem. According to KFF polling, about seven in ten insured adults say prior authorization is a burden. New evidence from the Office of Inspector General (OIG) within the Department of Health and Human Services documents the high rate of denials of prior authorization requests for certain post-acute care services in Medicare Advantage plans, which now enroll more than half of all Medicare beneficiaries.
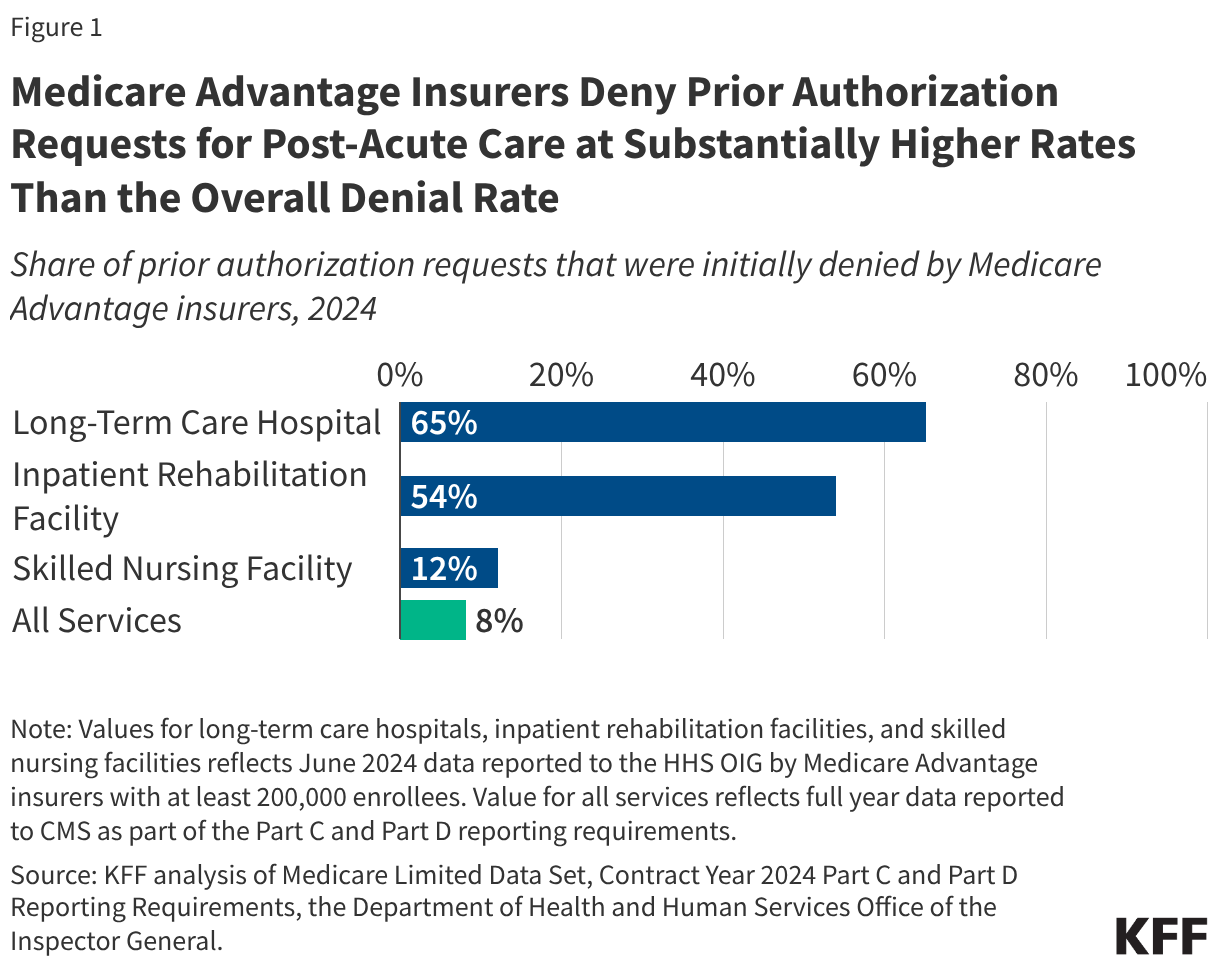
The OIG recently published two reports finding that Medicare Advantage insurers deny more than half of all prior authorization requests for the most expensive types of post-acute care, including 65% of requests for stays in long-term care hospitals (LTCHs) and 54% of requests for stays in inpatient rehabilitation facilities (IRFs), as well as 12% of requests for stays in skilled nursing facilities (SNFs). These denial rates are higher, and in the case of LTCHs and IRFs substantially higher, than the overall Medicare Advantage prior authorization denial rate found by KFF in previous analysis of less than 8% for all services (Figure 1). The OIG also found substantial variation across insurers, highlighting the heterogeneous experience Medicare Advantage enrollees could face depending on the private insurer that administers their Medicare benefits.
Insurers use prior authorization to reduce the use of unnecessary or low-value care and to restrain costs. KFF analysis shows that virtually all Medicare Advantage enrollees are in a plan that requires prior authorization for at least some services – most often, high-cost services. For example, in 2026, 95% of Medicare Advantage enrollees are in a plan that requires prior authorization for skilled nursing facility stays. According to the Medicare Payment Advisory Commission (MedPAC), the average Medicare payment in 2023 for traditional Medicare beneficiaries was $43,000 per LTCH stay, $24,000 per IRF stay, and $16,000 per SNF stay.
In 2024, insurers made nearly 53 million prior authorization determinations for Medicare Advantage enrollees. In contrast, prior authorization is rarely used in traditional Medicare (notwithstanding a new Innovation Center model testing the use of AI tools to conduct prior authorization for a limited set of services in traditional Medicare). The new OIG findings suggest the burden of delays and denials from the use of prior authorization is greater for Medicare Advantage enrollees with higher health needs and in more fragile condition. LTCHs generally treat patients with multiple serious conditions, providing services such as respiratory therapy, head trauma treatment, and pain management over the course of hospital stays that extend more than 25 days, on average. IRFs provide intensive rehabilitation services, including for people recovering from strokes or brain injuries. The initial denial of the prior authorization request meant that the requested post-acute care was delayed between 5 and 6 days, on average. In addition to having potential health implications for enrollees seeking post-acute care, the delay could mean higher out-of-pocket spending for the associated hospital stay, because many Medicare Advantage enrollees face daily cost-sharing requirements for hospital stays.
Additionally, the OIG found that when denials were appealed – which happened for 36% of LTCH denials, 31% of IRF denials, and 18% of SNF denials – the requested service was ultimately approved much of the time for LTCHs (36%) and IRFs (43%), and virtually all of the time for SNFs (95%). The extremely high rate of overturning the initial decision upon appeal for SNFs raises questions about whether this care is being routinely inappropriately denied. At the same time, if insurers anticipate that only a relatively small number of initial denials will be appealed, the high overturn rate could reflect a determination by insurers that reversing an initial denial is preferable to having the appeal continue to the next stage. At that point, an independent review entity (IRE) would hear the case, and if the IRE disagrees with the Medicare Advantage insurer’s initial determination to deny a service, that would have a negative impact on a plan’s star ratings.
The findings in the OIG reports are consistent with a previous Senate investigation that found the largest Medicare Advantage insurers denied prior authorization requests for post-acute care at substantially higher rates than other services between 2019 and 2022. Together, these reports underscore the value of having service level data on the use of prior authorization in Medicare Advantage. However, detailed data on the use of prior authorization and denial rates by type of service in Medicare Advantage are not yet required to be reported and therefore not routinely available. The lack of detailed data on prior authorization requests, denials, and appeals has made it difficult to understand the impact on people seeking care and to assess whether initiatives, such as the pledge taken by several private insurers last summer to improve the prior authorization process, are leading to meaningful change. CMS introduced a pilot program to collect more detailed data at the plan and service level this year and anticipates requiring this information beginning in 2027. Nevertheless, it will be several years before those data are available.