Medical Frailty and Medicaid Work Requirements: Challenges for People with HIV
On June 1, 2026, the Centers for Medicare and Medicaid Services (CMS) issued an interim final rule providing states with guidance for implementing Medicaid “community engagement” or Medicaid work requirements as part of the 2025 federal budget reconciliation law. The law requires states to condition Medicaid eligibility for enrollees with coverage through the Affordable Care Act (ACA) expansion or under certain waivers on meeting these requirements or qualifying for an exclusion, including one related to being “medically frail or otherwise” having “a special medical need.” In defining medical frailty, the rule introduces a two-part test, requiring an enrollee to both have a qualifying condition and demonstrate that the condition impairs their ability to fulfill the community engagement requirement, differing from stakeholders’ expectations. Early on, and as with Nebraska’s early implementation, states believed they would be able to exclude people based on presence of a condition alone and several states planned to exclude all people with HIV.
On June 29, 2026, twenty-four (24) states and two (2) state governors sued CMS in Massachusetts District Court challenging aspects of the regulation, including its requirement that to qualify for the medical frailty exclusion an enrollee’s condition must significantly impair their ability to comply with community engagement requirements. Among other arguments, the plaintiff states claim this additional requirement is contrary to the reconciliation law (H.R.1) and that “H.R. 1’s broad statutory exclusions exist for good reason. People with disabilities, patients in the middle of cancer treatment, or those struggling with another serious or complex health condition, shouldn’t be at risk of losing the care that helps maintain their health.” Whether the court grants their request to enjoin and vacate the challenged provisions, including the medical frailty two-part test, is yet to be seen.
In the meantime, because Medicaid is the primary source of insurance coverage for people with HIV, this new requirement and state implementation decisions, will have a significant impact on this population’s access to Medicaid going forward and could affect the nation’s efforts to address HIV.
This analysis reviews the implications of the rule’s definition of medical frailty for people with HIV. (For a broad overview of medical frailty, definition of terms, and the impact of the regulation beyond HIV, see this KFF analysis.)
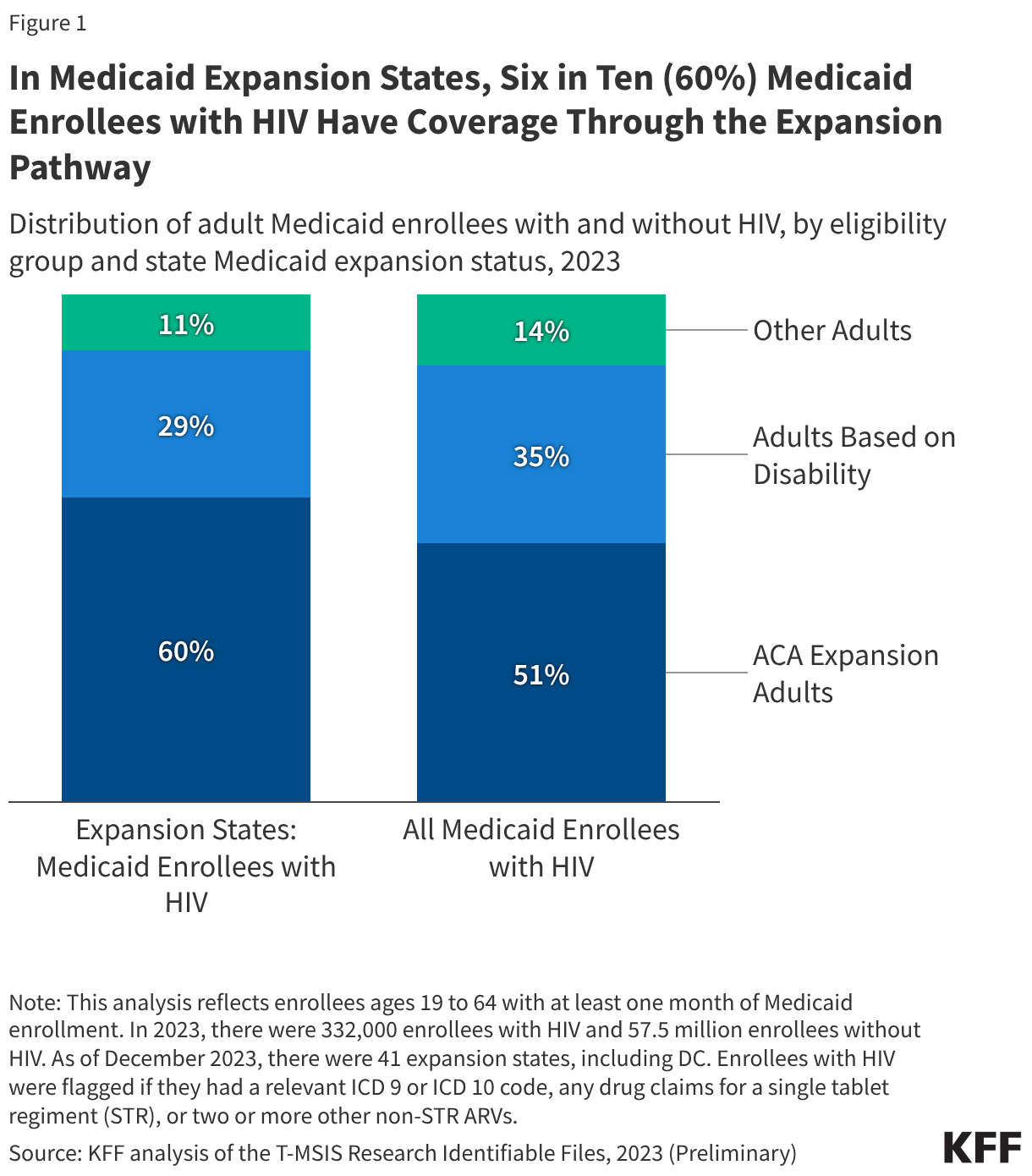
Medicaid expansion is the most common pathway for Medicaid coverage for people with HIV, so many with HIV will be subject to new work / community engagement requirements. Medicaid is the largest source of insurance coverage for people with HIV and plays a larger role in covering adults with HIV than adults without HIV. Nationwide, nearly half (46%) of people with HIV had coverage through the Medicaid program in 2023. In states that have expanded their Medicaid programs, Medicaid expansion is the primary pathway to coverage for people with HIV. In 2023, 60% of adults under age 65 with HIV in expansion states had coverage through the expansion pathway and would be subject to work requirements (see Figure 1). Before states expanded Medicaid programs under the ACA, many people with HIV did not have access to affordable coverage until they had an advanced condition to qualify through a permanent disability pathway and many were uninsured, despite coverage and access to care having the potential to stave disability off in the first place.
The approach to determining medical frailty specified in the rule will make it more difficult for individuals with HIV to obtain a medical frailty exclusion from work requirements. The rule imposes a two-part test that defines as medically frail an individual who is blind or disabled; has a substance use disorder; has a “disabling” mental disorder; has a physical, intellectual, or developmental disability that limits the ability to perform one or more activities of daily living (ADL); or has a “serious or complex” medical condition and whose condition impairs their ability to fulfill the community engagement requirements (including but not limited to work). While the rule includes HIV/AIDS as one of 19 example conditions that would be reasonable for states to consider as a serious or complex medical condition, it further specifies, using HIV as an example, that, “Individuals with HIV/AIDS are medically frail if they are determined to have a serious or complex medical condition that significantly impairs the individual's ability to comply with the community engagement requirement, which is less likely to be the case if the acuity of their condition is not severe.” Access to antiretroviral medication, including through Medicaid, is necessary to manage HIV and prevent immune system dysfunction, illness, and ultimately death. To the extent people with HIV lose access to Medicaid due to work requirements, including failure to navigate reporting rules, they may develop more severe conditions.
People with HIV whose condition is well managed may qualify as medically frail if they have another medical condition that limits their ability to work. Nearly three-quarters (73%) of people with HIV enrolled in Medicaid have chronic conditions (other than HIV), compared with four in ten (42%) of those without HIV. Alternatively, people with HIV may qualify as medically frail under one of the other categories. Notably, people with HIV are more likely than other Medicaid enrollees to have an SUD or mental health condition. Nearly, one-quarter (23%) of people with HIV had an SUD diagnosis compared to 8% of Medicaid enrollees without HIV and over one-third (36%) of Medicaid enrollees with HIV had a mental health condition diagnosis, some of which may be considered “disabling,” compared to 16% of Medicaid enrollees without HIV. People with HIV also experience high rates of disability--half (50%) of likely Medicaid expansion enrollees with HIV have a disability, including a functional disability (e.g. difficulty climbing stairs, dressing oneself, etc.) or an AIDS (stage III HIV) diagnosis.
The rule requires states to use claims and encounter data to identify individuals who may be medically frail, but does not provide guidance on how to assess whether a condition limits an individual’s ability to meet the community engagement requirements. States will be required to maintain an auditable list of medically frail conditions (in the form of diagnosis codes) that could include HIV. States will have discretion over the creation of this list and may include only some codes for each condition. For example, Nebraska’s list of ICD-10 codes released before the state implemented work requirements on May 1, 2026 only included one of several codes for HIV which would not capture all enrollees with HIV. The rule also makes clear that diagnoses alone cannot be used to determine medical frailty because of the need to assess whether the condition impairs the ability to work or engage in community service. This additional requirement will limit the ability to verify medical frailty on an automated, or ex parte, basis and will require states to use other verification methods.
The regulation offers examples of the types of providers that states could use to verify medical frailty including a range of clinicians. CMS’s inclusion of “clinical social workers” on this list could be especially meaningful for people with HIV given that many get care through clinics with integrated social and support services whose staff help with insurance navigation. However, the administrative burden on treating providers is likely to be significant
For people with HIV, the reliance on data sharing, confirmation from treating providers, and health screeners and self-attestation to verify medical frailty exclusion status may raise unique privacy issues and barriers due to stigma:
- Data sharing: Some states are exploring using a data-sharing process between the state Medicaid and state public health/HIV office which could help them identify enrollees without HIV related claims histories, including those new to Medicaid. Some states already have a data sharing agreement in place. However, this public health data is highly sensitive, and some have raised concerns about data privacy and security related to HIV status.
- Provider documentation. As noted, the rule permits states to accept documentation of qualifying conditions and medical frailty from providers. However, the requirement to assess and report the severity of patients’ conditions and the impact on their ability to meet the work requirements may raise ethical concerns for these providers, particularly given the emphasis in HIV care on care engagement for both the patient’s and public health.
- Health screeners and self-attestation. The rule encourages states to use health screeners at application and renewal to identify individuals who may be medically frail, which could include people with HIV. Separately, though its use will be more limited starting in January 2028, most states will also likely allow self-attestation when existing data sources are insufficient to document a qualifying condition and the inability to work. However, the stigma associated with HIV may discourage individuals from disclosing their condition and how it impacts their life.
Coverage loss for people with HIV could negatively impact individual health, public health, and place an increased burden on already stretched HIV programs. Given the new requirements in the regulation, a blanket exclusion for people with HIV will not be possible which will mean a greater staff burden (at the state Medicaid agency and in clinics), higher costs, and potentially wide scale churn, disenrollment, or coverage rejections for those with HIV. While earlier KFF research found that one-third (33%) of likely expansion enrollees with HIV were working at least 20 hours per week and another 4% had dependents at home, the need to document work compliance or medical frailty status, could challenge coverage retention for people with HIV which could lead to disruptions in care and treatment and subsequently increased risk of morbidity, mortality, and HIV transmission. Such a scenario also runs counter to federal goals in the Administration’s Ending the HIV Epidemic Initiative and the Ryan White Program Moving Forward (formerly Ryan White Program 2030) vision. Indeed, four in ten new HIV transmissions are associated with someone who is aware of their HIV status but not in care. Treatment interruptions can also lead to antiretroviral resistance, making future treatment and care more complex. Additionally, if people with HIV lose Medicaid coverage some may turn to the federal Ryan White Program. This comes at a time when state Ryan White Programs across the country are facing budget crises due to a range of factors and coverage losses due to work requirements represent an additional challenge for programs to weather.