The Medical Frailty Exemption from Medicaid Work Requirements: Key Issues to Watch for in Upcoming CMS Guidance
For the latest analysis on the medical frailty exemption and key takeaways from the published interim rule, see our updated brief.
The 2025 reconciliation law requires states to condition Medicaid eligibility for adults in the Affordable Care Act (ACA) Medicaid expansion group and enrollees in partial expansion waiver programs (Georgia and Wisconsin) on meeting work requirements starting January 1, 2027 or sooner at state option. The law specifies mandatory exemptions, including individuals who are “medically frail.” To ease the burden on individuals, the law directs states to use available information “where possible” to verify compliance with Medicaid work activities or exemption status, without requiring additional documentation from individuals. Given the abbreviated implementation timeline, states are moving forward with key decisions over how to implement the medical frailty exemption even as they wait for formal guidance from the Centers for Medicaid and Medicare Services (CMS), which is required to issue an interim final rule by June 1, 2026. This brief describes early state plans to operationalize the medical frailty exemption and identifies key issues that they are facing and may be answered in the forthcoming guidance.
What is the Medical Frailty Exemption?
The reconciliation law requires states to exempt from work requirements an individual who is “medically frail or otherwise has special medical needs.” The law specifies this includes individuals who are blind or disabled; have a physical, intellectual, or developmental disability that limits their ability to perform one or more activities of daily living (ADL); have a substance use disorder or a “disabling” mental disorder; and those with “serious or complex” medical conditions. This definition closely aligns with an existing federal medical frailty definition that CMS uses for states choosing to set “alternative benefit plans” that differ from the traditional Medicaid benefit package. In that context, CMS used the definition as a minimum standard for medical frailty but allows states flexibility to define medical frailty beyond the statutory and regulatory definitions. To identify individuals who are medically frail, CMS noted in the 2013 final rule that it expected states to use Medicaid claims data and encouraged them to use self-attestation and health screeners for applicants and new enrollees where the state does not have information on their current health status or historic encounter data.
How do States Plan to Operationalize the Medical Frailty Exemption?
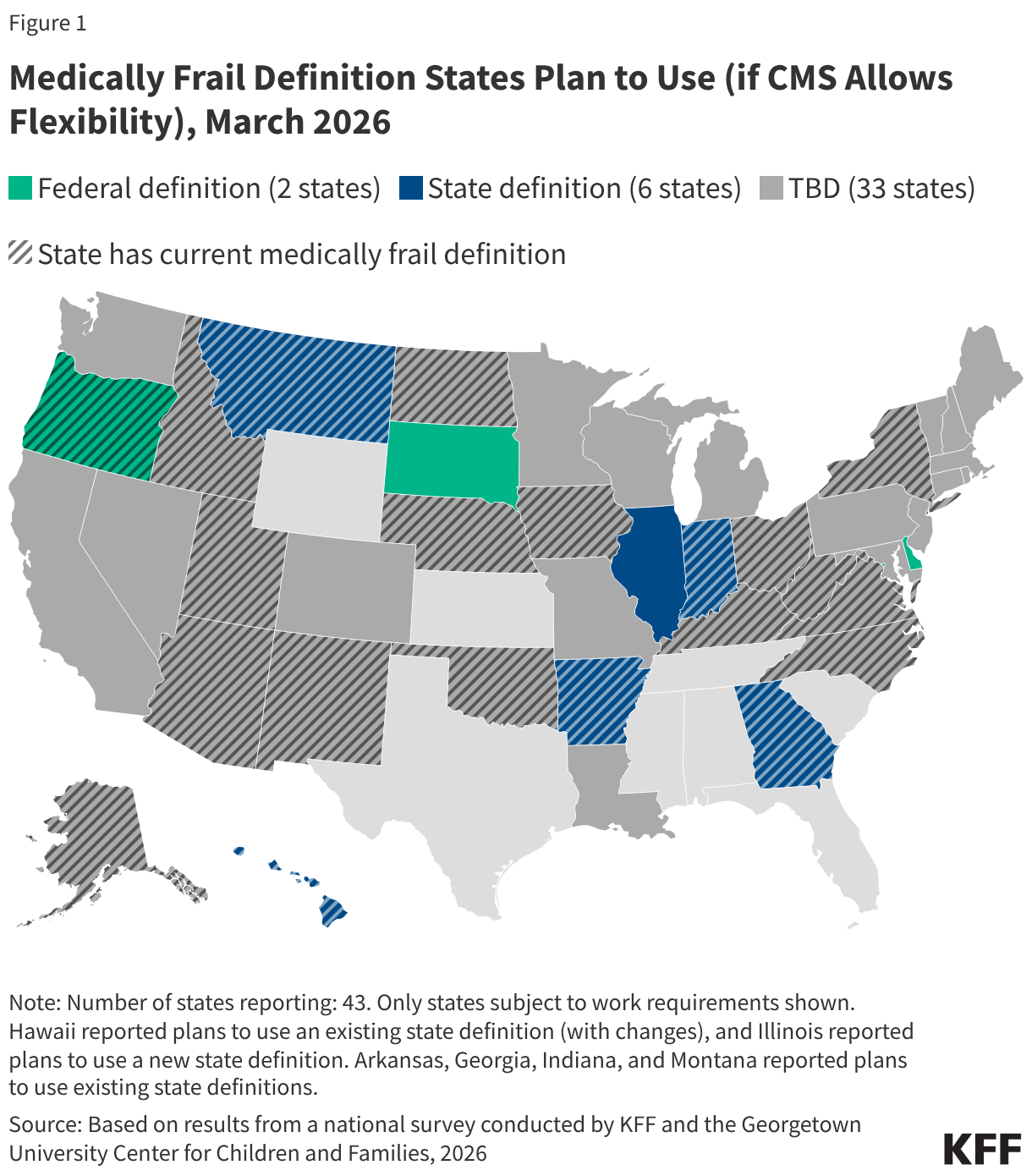
Most states have not yet finalized a medical frailty definition, likely reflecting ongoing uncertainty over how much flexibility states will have as they await June CMS guidance. In a recent KFF survey (fielded January-March 2026), about half of states (22) subject to work requirements report having a current state medical frailty definition, though it is unclear whether these definitions align with the medical frailty provisions in the reconciliation law (Figure 1). Most of these definitions were not developed with work requirements in mind and may need to be updated to reflect the new federal requirements. Thirty-three states indicated they had not yet determined what definition they plan to use at the time the survey was fielded. If states are given flexibility by CMS to define who is medically frail and exempt from work requirements, six states would prefer to use a state definition (either an existing definition or a new definition,) while four states would use a federal definition.
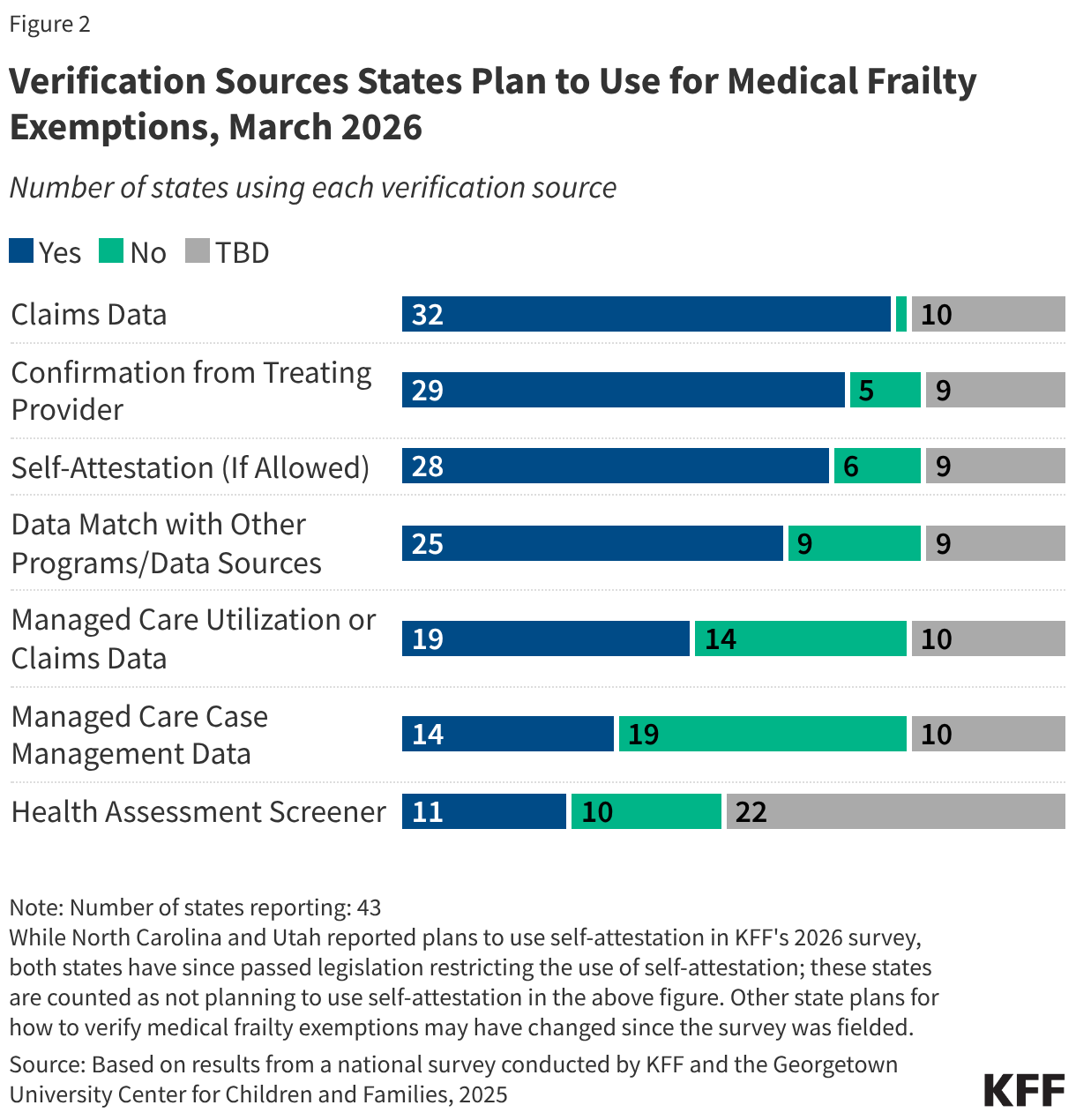
States plan to use a variety of methods to verify medical frailty status, including using data to automate the process where possible. Most states reported plans to use Medicaid claims data (32) to verify medical frailty exemption status, while Georgia indicated it would not use claims data, and the remaining ten states had not yet made a decision at the time of the survey. New applicants and recent enrollees may not have claims data on file, requiring states to use other forms of verification. All 32 states reporting plans to use claims data also reported plans to use other sources, such as data from other programs (e.g., enrollment in a behavioral health managed care plan or HCBS program), managed care utilization or claims data, and/or managed care case management data. Twenty-nine states said they will seek confirmation from a treating provider. Many states are developing health assessment screeners to collect information to identify medical exemptions, and 11 states said they will use the health screeners to verify medically frail status. Most states (30) also reported wanting to allow applicants and enrollees to self-attest to their medically frail status if verification data are not available and self-attestation is permitted by CMS. However, some states reported they do not plan to accept self-attestation (AR, HI, IN, MT) or have since passed legislation barring the use of self-attestation (NC and UT).
Nebraska, which became the first state to implement new work requirements on May 1, 2026, has released resources outlining how it will process medically frail exemptions, as well as an index of diagnosis and procedure codes. Examples of conditions covered in the thousands of codes include types of cancer, HIV, diabetes, heart disease, and certain types of mental health conditions and substance use disorders, among others. For existing enrollees, Nebraska is reviewing medical claims data prior to renewal and will auto-exempt an individual if indicated based on diagnosis/procedure codes. If Nebraska cannot determine medical frailty through claims data or other data sources, existing enrollees will need to submit a self-declaration form. Not all individuals will be able to be auto-exempted due to limitations of claims data such as:
- A lack of data on file for new applicants and recent enrollees;
- A lack of data on file due to providers not consistently coding or not using the codes identified by the state;
- Selected diagnoses and procedures potentially not being comprehensive of all individuals with target conditions or not capturing functional limitations;
- A lack of claims within the look-back period despite an individual having an exempted chronic condition or disability; and
- Delays between clinical care and claims presenting.
The state also intends to use the self-declaration form to identify medically frail exemption status for new applicants. The self-declaration form requires individuals to provide a description of their health condition, the contact information of their treating provider, and a note if services were provided while enrolled in Medicaid. No additional documentation is required at this time (e.g., a note from a provider or other proof of a condition). Nebraska indicates that it plans to move from self-declaration to more automated verification methods consistent with federal guidance over time, and plans to continue to review and update the index of ICD-10, CPT, and HCPCS codes as federal direction is clarified.
Early insights from other states highlight the variety of ways states are planning to use multiple sources of information to identify medical frailty. For example:
- California plans to automatically exempt individuals who are eligible for certain programs (e.g., home care—also known as home- and community-based services or HCBS) and has been exploring more timely data sources such as managed care plan care management systems in conjunction with evaluating which diagnostic codes could be used to establish medical frailty.
- Pennsylvania has outlined a plan to first check health care claims, followed by information from electronic health records exchanged through regional health information organizations, managed care organization (MCO) health assessments and case management information, and finally information provided by the applicant. Pennsylvania explains its approach is designed with data limitations in mind, and aims to reduce paperwork burden and streamline the process for beneficiaries.
- South Dakota has shared early plans to use clinical code lists and a medically frail health screener. Indicating lingering uncertainty on CMS’s stance regarding self-attestation, the state notes it may have to use physician attestation at renewal if screeners cannot be repeated and claims data is still not available.
- Several states also have reported that they would be interested in adding new categories such as homelessness to the medical frailty category but understand from communications with CMS that states may not have flexibility to do so.
How Will the CMS Guidance Address Key Issues and Potential Implications?
Although states are moving forward with operationalizing the medical frailty exemption, the interim final rule that CMS is required to release by June 1, 2026, is expected to address key issues related to defining and verifying medical frailty. Because of the time required to make system changes, states have been moving forward with implementing work requirements based on informal communication and guidance CMS has shared. Any significant changes to that informal guidance could require states to change course and could have implications for states’ readiness to implement work requirements as well as the costs associated with implementation. Key issues that may be addressed in the guidance, and that states report waiting on, include:
Defining Medical Frailty
- Defining medical frailty. CMS may provide a federal definition of medical frailty in the guidance. The law suggests the need for a Secretary-provided definition in its list of exemptions by including anyone “who is medically frail or otherwise has special medical needs (as defined by the Secretary).” It is not clear if CMS will rely on the existing definition or develop a new definition that more directly relates to work requirements. The statute includes people who are both medically frail and those with “serious or complex medical conditions,” which includes people with significant medical needs that may or may not limit their ability to engage in qualifying activities. For these individuals maintaining access to health coverage protects against serious health consequences if treatment is interrupted and may enable them to work.
- State flexibility to define medical frailty. Whatever federal definition CMS establishes, another important consideration is whether the definition serves as a minimum standard that states can use or expand on or whether CMS will require states to use the federal definition with little or no flexibility to interpret how it will be applied. For example, CMS may specify a set of diagnoses codes for states to use in their claims data analysis, but the effect of that list will depend greatly on whether states are allowed to add additional codes to CMS’ list. This may be particularly relevant in states that use state-specific diagnosis or treatment codes in their Medicaid billing systems.
- Identifying people with functional limitations and mental health conditions. As noted, the law required people “with a physical, intellectual or developmental disability that significantly impairs their ability to perform 1 or more activities of daily living” be exempted. Guidance may provide additional insight into how states are expected to capture functional limitations in medical frailty definitions, as it may prove more difficult to identify these individuals using claims data. While there is a diagnostic code that could help to capture this, it is generally underutilized, with one barrier being a lack of financial incentive. More comprehensively identifying enrollees with these functional disabilities may require technical assistance for states and providers (i.e. in terms of utilizing different codes). Guidance may also provide clarity on identifying individuals with mental health conditions who may also be difficult to identify using claims data, as well as provide clarity on the exact diagnoses that would qualify.
Verifying Medical Frailty
- Data sources for verifying medical frailty. States will likely be expected to use claims data to automate identification of medically frail individuals. The guidance may provide information on other data sources states can use or would be expected to use, such as electronic health records, MCO health assessments and case management information, and pharmacy data. States may also be required to use SNAP data and other program data, such as HCBS enrollment or enrollment in a behavioral health managed care program, to identify medically frail individuals. Accessing some of these data sources may raise privacy concerns that the guidance may or may not address.
- Data look-back. The guidance may also specify the length of time states are permitted to look back to identify individuals with qualifying conditions when using data or verification from providers, including whether there are different look-back periods permitted at application versus renewal. The length of the look-back period will affect how many individuals are captured under the medically frail exemption (longer look-back periods are likely to pick up more people who may qualify as medically frail).
- Exemption re-verification. The legislation does not currently clarify how frequently medical frailty exemptions may last before states are expected to re-verify individuals’ exemption status. States may need to reverify exemption status at every renewal, or states may be able to create an internal flag and/or permanently exempt some people if their health condition or disability status is unlikely to change.
- Self-attestation. It is unclear if states will be permitted to accept self-attestation or if they will be prohibited from using it (altogether or in certain circumstances). Some state officials have noted the limitations of existing data sources, particularly claims data, for identifying new applicants who are medically frail as well as enrollees at their first renewal. Self-attestation could be subject to CMS audits, and guidance may outline under what circumstances states are expected to use self-attestation (e.g., only initial application, at renewal). If self-attestation is permitted, questions remain whether attestation alone will suffice or whether enrollees will be required to also provide supplemental information (e.g. provider sign-off, clinical or pharmacy records, etc.).
- Health screeners. States may look to use health screeners at application and renewal, especially in the absence of self-attestation. States may have flexibility to create their own health screeners, or there may be a federal template.
- Confirmation from providers. When using provider verification, the guidance may specify any requirements, including what information must be collected and whether providers will be required to assess whether an individual’s condition limits their ability to work. Relying on provider confirmation could increase administrative burden (on the clinical workforce, individuals, and states), particularly for providers that treat large shares of Medicaid patients, and, depending on the information requested, could raise ethical concerns among providers.
- Exemption hierarchy. When individuals qualify under multiple exemptions or when they would qualify for a medical frailty exemption but also are engaged in qualifying work activities, states will need to develop standards for how to operationalize which status is prioritized (e.g., checking exemption status and work status in a specified order, choosing to use whichever is longer lasting), especially if certain conditions will have longer exemption periods. The guidance may establish a hierarchy for states to follow or may give states the ability to set their own hierarchies.