Are the Tradeoffs from Prior Authorization Worth It?
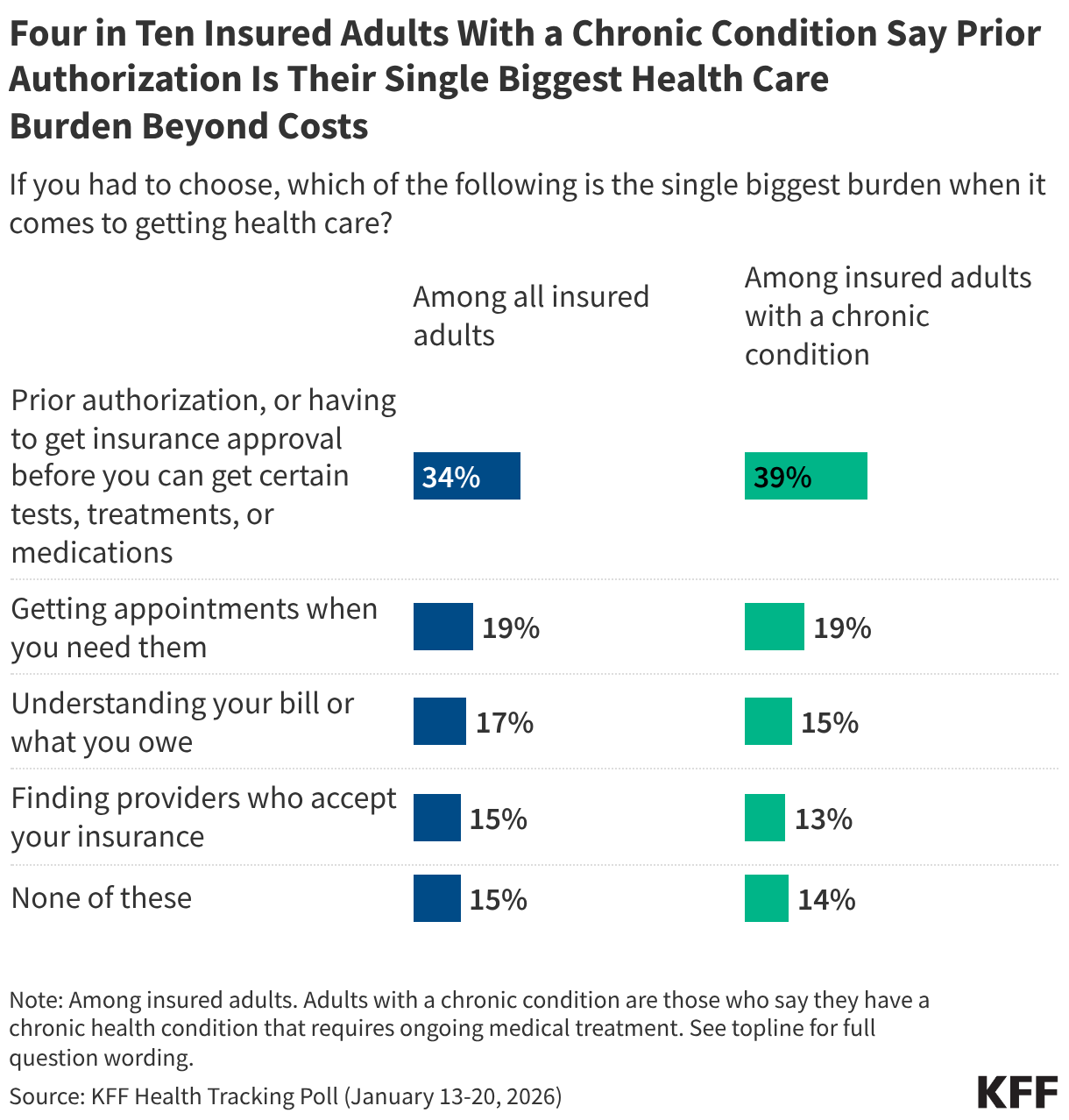
Costs are the health care problem that most worry the American people. But nothing makes American health care consumers more frustrated using the health system than prior authorization review. I know because they told us that, ranking prior authorization review far ahead of any other problems they have getting care and navigating the health care system, including getting appointments and understanding their bills. Four in 10 people with chronic conditions say it’s their single biggest burden getting health care.
Take Medicare Advantage plans as a case in point. In 2024, they did 53 million prior authorization reviews, almost two per enrollee, turning down 7% of them. You know what it can take to get approvals. Often, countless phone calls and messages in apps to your insurance company and doctor’s office, ending up in some cases with a “peer-to-peer” review between the doctor and the insurance company (are they “peers” in this relationship?). Stress. Delay. Sometimes hours on the phone or days waiting for a call back. And sometimes, the result is an approval only to discover that the venue is denied or out of network, or the quantity of a drug the patient has taken for years requires a separate annual prior approval. The problem isn’t limited to Medicare Advantage, it’s common throughout the insurance system, except for traditional Medicare (more on that below).
Health professionals also dislike prior authorization, especially specialists who order more expensive tests and procedures and have to run the gauntlet of the prior authorization process to get them approved. Their administrative staff does battle daily with insurance company staff over them. More and more, provider AIs and insurance company AIs try to outmaneuver one another over reviews. Everyone thinks they are holy in this tug of war: the doctors who see the insurance companies as greedy profiteers trespassing on their professional judgment, and the insurers who see themselves as the line of defense against doctors who often don’t follow guidelines for best practices or have a financial stake in doing more in a fee-for-service system.
There is some disagreement about whether prior authorization review reduces costs for payers and protects quality by denying unnecessary services or shifting care to equally effective, lower-cost services, or whether it increases costs and leads to adverse outcomes over time by delaying or denying needed care, and studies are available to support either claim. This is not the place for a literature review, except to say prior authorization can and does do both. There should be no debate, however, that it adds to the complexity of our health system, frustrates patients and providers, and drives up administrative costs.
The assumption has been that we are stuck with this. Payers have few tools to control costs in our system, and prior authorization is one of them. But with such profound public angst about it, it’s time to ask if it’s worth the tradeoffs.
Current efforts to change prior authorization review focus on incremental reforms aimed at making it less onerous. States have introduced a range of reforms to streamline prior authorization review, exempting physicians with good track records from review, suspending prior authorization for ongoing care for some people with chronic conditions, requiring that physicians double-check reviews made by insurance company AIs, and more. The Trump administration has joined the fray, too, announcing a voluntary effort with big health insurance companies to speed up and simplify prior authorization review, including reforms that promise to cut back on what is reviewed and how often. We should begin to see how real this voluntary effort is this year.
The bigger question, though, is: could we get rid of prior authorization entirely? I can’t think of anything that would be more politically popular for a candidate planning a midterm or 2028 platform on health, although debate about whether premiums would rise, fueled by insurers, could reduce enthusiasm somewhat.
One approach I used to discuss with my friend, the late Uwe Reinhardt, the great health economist and a frequent critic of insurance companies, was to take prior authorization review out of the hands of insurance companies altogether, setting up independent nonprofit physician-led organizations to take over the job. That would remove the incentive insurance companies have in the current system to put profits over patients. It is, however, trading one big and already established corporate bureaucracy for an entirely new nonprofit one that would have to be constructed and funded across the country (I assume it could be funded mostly by a tithe on health plans much like ACA Marketplaces are).
As health policy historians among us will know, we tried something like that years ago and while it didn’t operate as prior authorization does today, the experience was instructive. It was called the Professional Standards Review Organization (PSRO) Program, and it was administered by CMS (then HCFA) through its Health Standards and Quality Bureau. PSROs—physician-led nonprofit organizations across the country funded by Congress—attempted to control costs by reviewing hospital admissions and hospital stays, with a negative determination resulting in denial of reimbursement by Medicare or Medicaid. Eventually, the program was deemed to cost more than it saved and was repealed in 1982, when the focus shifted generally from costs to quality in a more anti-regulatory environment.
Another approach would be to follow traditional Medicare, which doesn’t do prior authorization review except in very limited cases. Insurers will be quick to argue that premiums will rise even more without prior authorization review. They may be right, even if it also drives up costs for the health system in the long run by delaying and denying some needed care and adding administrative costs. One study by Milliman, which I discussed in an earlier column, calculated the ranges for potential premium increases. It’s also possible that prior authorization has a deterrent effect on physicians and hospitals just by being there, which no one has calculated.
But it’s non-trivial that traditional Medicare has operated almost entirely without prior authorization review. Only recently did the Trump administration—some would say counter intuitively with prior authorization now so unpopular—decide to experiment with introducing it through a demonstration project called WISeR, the Wasteful and Inappropriate Service Reduction Model, to test out prior authorization for selected services in six states. WISeR reviews, perhaps surprisingly given public distrust, are mostly to be driven by AI, which is considered a virtue by its proponents.
Medicare was able to get by without prior authorization largely by paying providers considerably less than private insurance pays them, rather than by reviewing every procedure, test, or prescription to try to manage costs. It suggests a Medicare-like approach as one option: eliminate prior authorization review in return for a reduction in payments to providers (say 2%, for the sake of illustration). In effect, it would constitute a bargain, trading modestly lower payments for greater professional autonomy and lower administrative costs for physicians. It could be tried on a voluntary basis by a big self- insured employer, through a public program or systemwide. I am not sure if providers would welcome the deal or not. The burdens of prior authorization review do not fall equally on all practices and providers. I do know that, depending on which kinds of physicians are surveyed, between a third and half of physicians say they would not enter medicine if they had it to do over again, largely because of the perceived loss of professional autonomy. Hospitals would mainly benefit from reduced administrative costs and could have less interest. The idea would not be simple to implement.
Any move away from fee-for-service payment could also diminish the need for prior authorization review by reducing the incentive to provide more services. In integrated systems like Kaiser Permanente (no connection to KFF), doctors on salary don’t have a financial incentive to provide more care and the medical group they are part of makes the judgments about evidence-based care.
Every health policy change has tradeoffs. There are only so many tools payers have now to throw at health care costs, and prior authorization is one of them. But in a health system plagued as much by complexity as high costs, it is now public enemy number one for health care consumers, especially consumers who become patients and need a lot of care. The serious question we are not asking is whether the benefits it has for short-term cost control for insurers and their clients are worth the costs to patients and health professionals in an already labyrinthian health care system?
So, the big question: with all the tradeoffs, would you get rid of prior authorization review, or stick with the path we are on now, incrementally trying to make it slightly better?
