A Snapshot of Mental Health and Access to Care Among Nonelderly Adults in California
The COVID-19 pandemic has coincided with worsening mental health across the country, and California is no exception. For this data note, we analyzed data from the California Health Interview Survey (CHIS), which asks noninstitutionalized adults detailed questions on mental health and substance use, to further examine the impact of the pandemic on mental health in the state.
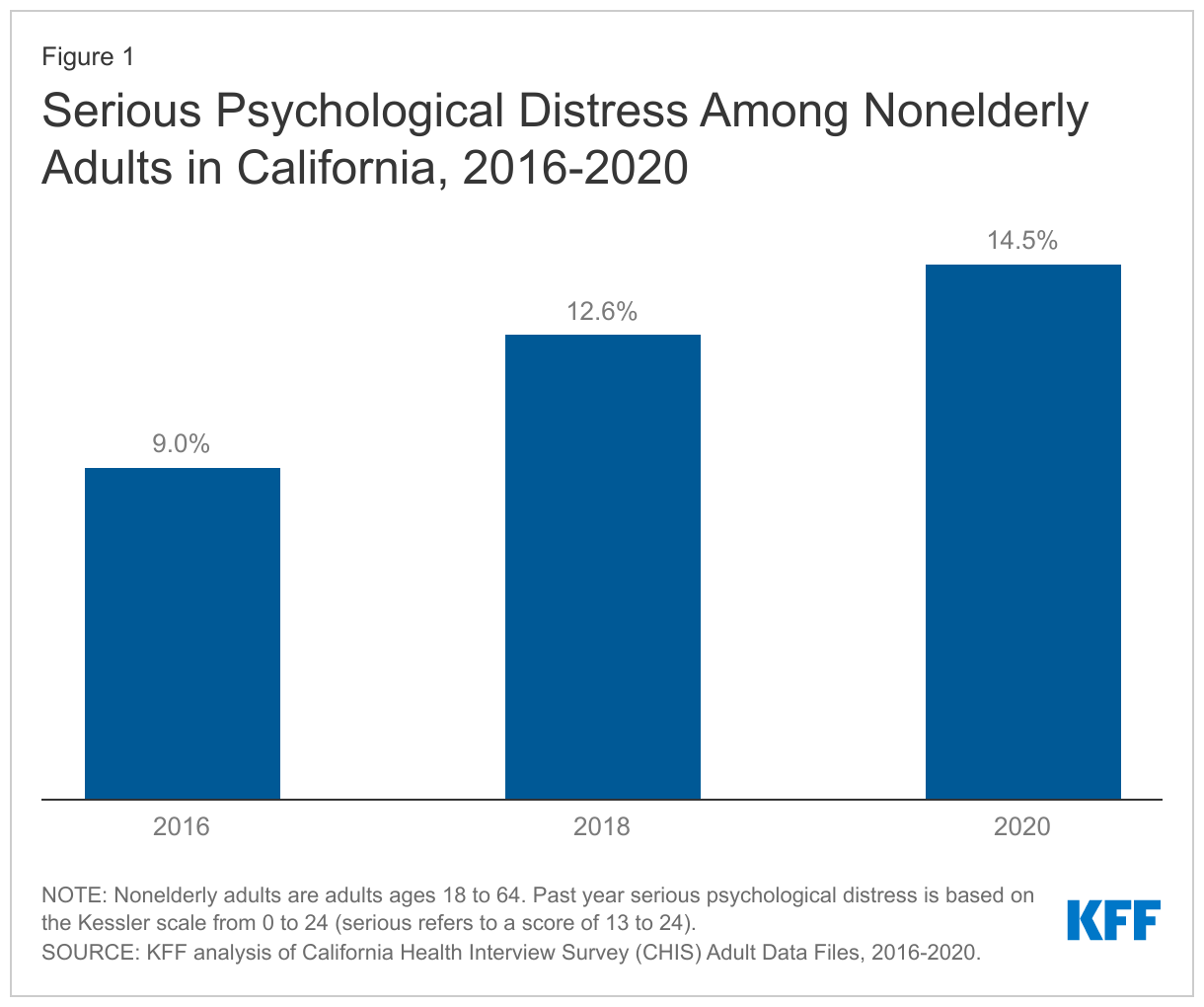
The pandemic comes on the heels of an already worsening mental health and substance use crisis in California. As shown in Figure 1, a growing share of nonelderly adults have reported past year serious psychological distress over time in California, up from 9% in 2016 to 15% in 2020. Substance use issues have also worsened – drug overdose deaths increased over 40% from 2019 to 2020 in California.
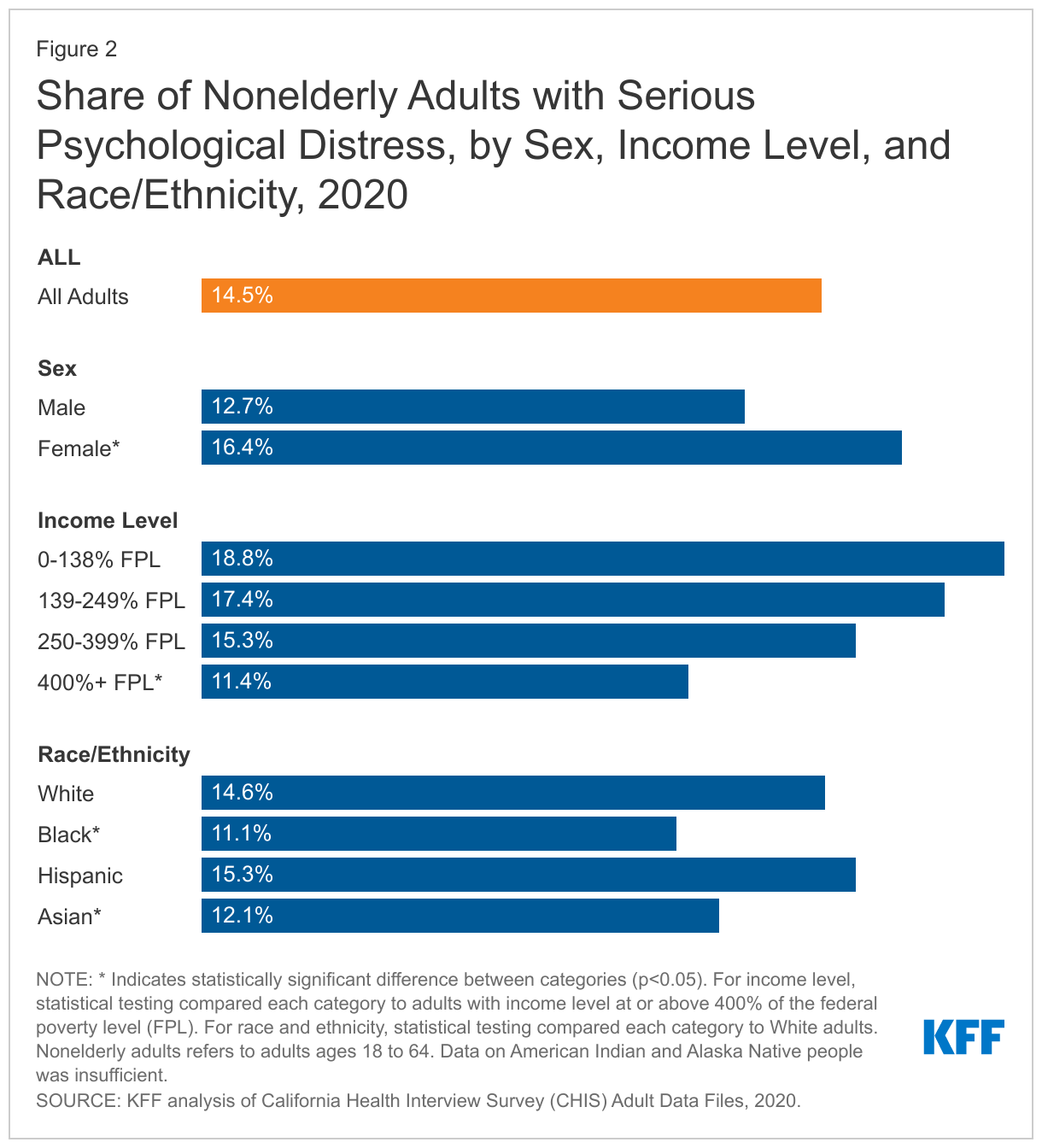
During the pandemic, serious psychological distress was more pronounced among some communities, including women and low-income adults in California. As shown in Figure 2, women in California (16%) were more likely than men (13%) to experience serious psychological distress in 2020. In general, women have more often reported poor mental health compared to their male counterparts both before and during the pandemic. In California, lower-income adults were more likely to experience serious psychological distress (19% for incomes between 0 and 138% FPL; 17% for incomes between 139 and 249% FPL; and 15% for incomes between 250 and 399% FPL) than high-income adults (11%) in 2020 (Figure 2). A recent survey of nonelderly adult Californians who saw a health care provider in the past year also found that low-income individuals were more likely than higher-income individuals to report worsening mental health during the pandemic.1 Separately, compared to White adults in California (15%), some communities of color – including Asian (12%) and Black (11%) adults – were less likely to report experiencing serious psychological distress in 2020 (Figure 2). Serious psychological distress among Hispanic adults (15%) was similar to White adults (Figure 2). Other KFF analyses found that, nationally, mental health and substance use concerns have been exacerbated among many people of color throughout the pandemic. Research has also shown that stigma – including stereotypes and discrimination – around mental health concerns is more pronounced among communities of color, perhaps affecting self-reporting of mental health and access to care. Additionally, a survey of adults in California found that among nonelderly individuals with mental health needs, people of color were less likely than White people to receive care.
In 2020, poor mental health outcomes among nonelderly adults varied greatly across counties in California. As shown in the map below, the share of nonelderly adults with past year serious psychological distress ranged from 9% to 28% across counties in 2020; highest in some Central Valley counties (Colusa/Glenn/Tehama, 28.3%; Butte, 26.9%; Merced, 24.2%) and lowest in Bay Area counties (San Francisco, 9.1%; Marin, 9.5%; Contra Costa, 9.6%). The share of nonelderly adults who ever had thoughts of suicide ranged from 8% to 34% across counties in 2020; highest in northern counties (Del Norte/Lassen/Modoc/Plumas/Sierra/Siskiyou, 34.3%; Butte, 29.7%; Mendocino, 29.2%) and lowest in some southern and eastern counties (El Dorado, 8.1%; Imperial, 8.8%; Placer, 9.3%).

Nearly nine in ten nonelderly adults in California have insurance coverage to help them access and cover the cost of health care, including mental health services. In recent years and in response to the pandemic, the state has introduced several policy measures to increase access to mental health and substance use services; many of these efforts leverage insurance coverage through Medi-Cal (the state’s Medicaid program), which covers 20% of nonelderly adults, or private coverage, which covers 67%.
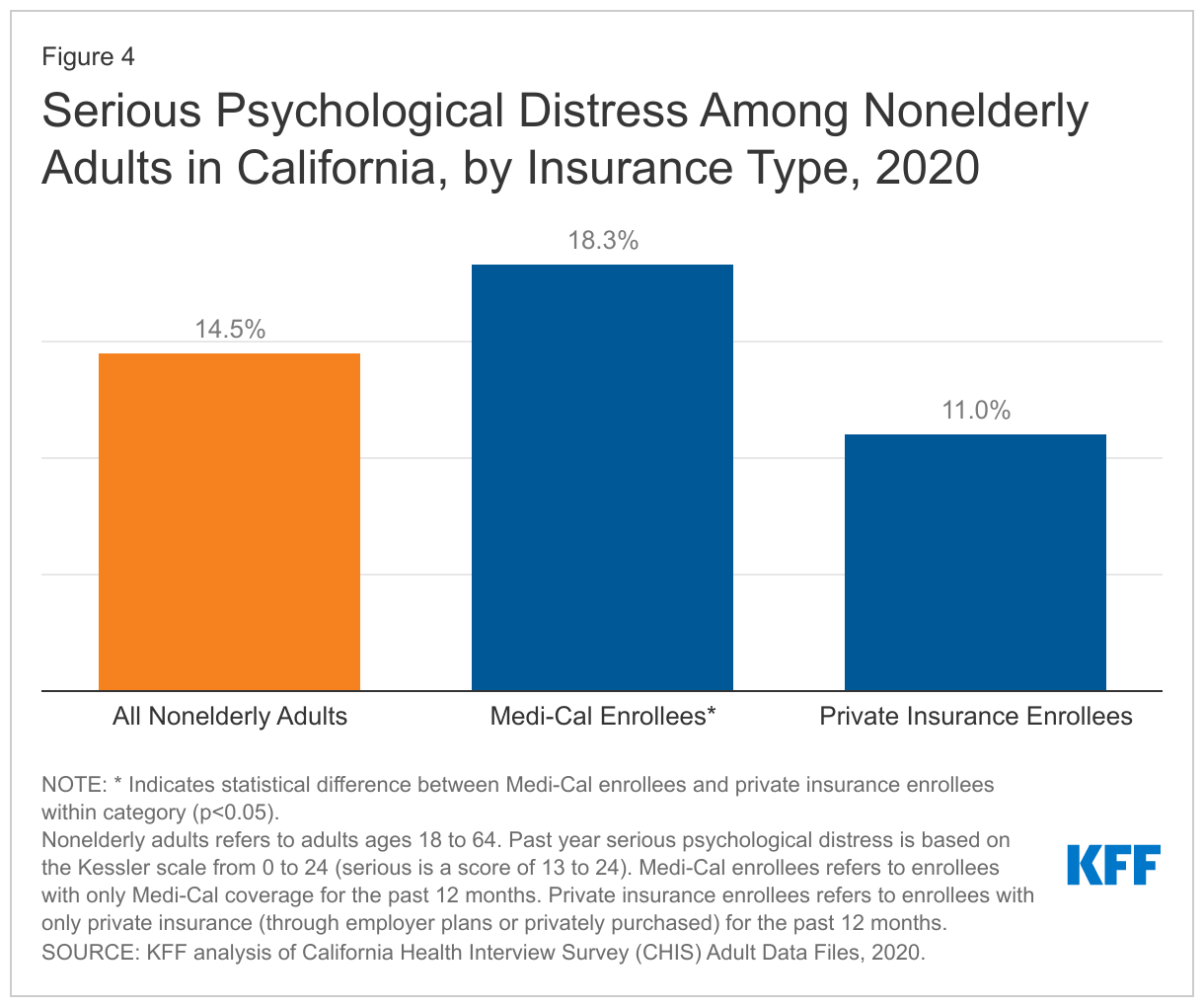
Across insurance types, large shares of nonelderly adults reported poor mental health outcomes in 2020. Medi-Cal enrollees were significantly more likely than private insurance enrollees to experience past year serious psychological distress in 2020 (18% vs. 11%, respectively) (Figure 4), perhaps reflecting Medi-Cal coverage of many people with disabling health conditions including serious mental illness and/or many low-income individuals who may be more likely to report poor mental health. Many nonelderly adults also reported thoughts of suicide in 2020: 14% among Medi-Cal enrollees and 13% among private insurance enrollees (data was not statistically different).
Many insured adults in California reported barriers to care for mental health and substance use services in 2020. Twenty four percent of nonelderly adults in California reported needing help for mental health or substance use issues in the past year (Table 1).2 Among nonelderly adults with mental health or substance use needs, the share who received treatment in the past year was similar across plan type (60% of Medi-Cal enrollees and 55% of private insurance enrollees) (Table 1). Medi-Cal enrollees who received treatment reported a higher average number of visits to a professional in the past year compared to their privately insured counterparts (18 visits vs. 11 visits).
Many Medi-Cal (40%) and private insurance (45%) enrollees with mental health or substance use needs did not receive treatment. Large shares of insured adults who did not receive treatment cited concerns about costs (54% of Medi-Cal enrollees and 49% of private insurance enrollees) and difficulties scheduling an appointment (30% of Medi-Cal enrollees and 20% of private insurance enrollees) as barriers. With the pandemic and accompanying economic recession, many adults have faced financial hardship and have had difficulty paying for usual expenses. This may be linked to the high shares of adults citing concerns over costs as a barrier for accessing mental health or substance use treatment – even for Medi-Cal enrollees, who have very low or no out-of-pocket costs for these services. Scheduling difficulties as a barrier to accessing mental health or substance use services may reflect an insufficient availability of providers.
| Table 1: Among Nonelderly Adults with Any Mental Health or Substance Use Needs, Access and Utilization of Services in the Past Year, by Insurance Type, 2020 | |||
| All Nonelderly Adults | Medi-Cal Enrollees | Private Insurance Enrollees | |
| Share of Nonelderly Adults with Mental Health or Substance Use Needs | 24.3% | 23.2% | 23.8% |
| Share that Received Treatment | 53.8% | 59.6% | 54.8% |
Average Number of Visits to a Professional | 13 | 18* | 11* |
| Share that Did Not Receive Treatment | 46.2% | 40.4% | 45.2% |
Did Not Receive Care Due to Concerns About Costs^ | 57.2% | 53.9% | 49.1% |
Did Not Receive Care Due to Difficulty Scheduling an Appointment^ | 23.0% | 30.2% | 19.9% |
| *Indicates statistically significant difference between Medi-Cal and private insurance enrollees.^Respondents were able to select from multiple reasons regarding not accessing needed mental health or substance use services.NOTES: Nonelderly adults refers to adults ages 18 to 64. Medi-Cal enrollees refers to enrollees with only Medi-Cal coverage for the past 12 months. Private insurance enrollees refers to enrollees with only private insurance (through employer plans or privately purchased) for the past 12 months.SOURCE: KFF analysis of California Health Interview Survey (CHIS) Adult Data Files, 2020. | |||
The pandemic highlights issues with accessing mental health and substance use care across California. California continues to face shortages of mental health providers. In light of pandemic-related precautions and restrictions, accessing services for health care, including mental health or substance use care, has been challenging nationally. In response, measures, including the temporary public health emergency, have allowed many providers to offer care through telehealth. Across the state of California, access to mental health care can also vary greatly. Specifically, for Medi-Cal enrollees, access can vary widely from county to county and navigating care can be particularly challenging for enrollees with co-occurring serious mental health and physical health needs.
In response to mental health and substance use needs in California during the pandemic, several policy actions were taken to increase and standardize access to care. Senate Bill 855 addresses gaps in existing mental health parity laws by requiring insurers to expand coverage to a broader range of mental health and substance use disorders (apart from Medi-Cal). Assembly Bill 2265 will allow for funds from the Mental Health Services Act, typically reserved for mental health services only, to be used for substance use services as well among people with co-occurring mental health and substance use issues. Additionally, through Senate Bill 803, Medi-Cal mental health and substance use services will expand to include peer support specialists. In California’s recent state budget proposal, funds were allocated for dyadic care – allowing for behavioral health services for parents to be incorporated into pediatric health care visits among Medi-Cal beneficiaries. California’s renewal applications for Section 1115 and 1915(b) waivers, known as California Advancing and Innovating Medi-Cal (CalAIM), were also recently approved. CalAIM builds on the state’s Medi-Cal 2020 Whole Person Care pilot program to coordinate and integrate physical health, behavioral health, and social services for Medicaid enrollees with complex needs. In addition to transitioning these services to the state’s managed care system, CalAIM includes behavioral health initiatives to address the division of services between county-level mental health plans and managed care plans, and to standardize access to services for enrollees with serious mental health needs. Private insurers have also taken steps to address mental health and substance use care. Nationally, some plans expanded coverage to include mental health or substance use services accessed through telehealth and many employer sponsored plans made changes such as waiving or reducing cost-sharing and increasing coverage for out-of-network services. Separately, California has taken steps to fund the statewide launch of 988, a mental health crisis hotline.
Looking ahead, further research on access to care and utilization of mental health services will be informative as state policymakers, administrators, and health care providers continue to discuss how to address mental health and substance use needs among Californians.
This work was supported in part by Well Being Trust. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
This analysis uses the 2020 California Health Interview Survey (CHIS) Adult Data Files, which surveys noninstitutionalized individuals. We narrowed our analysis to nonelderly adults, ages 18 to 64. In 2019, CHIS conducted a redesign of the survey. The redesign affected representation of different groups in the sample frame. Therefore, some demographic level data are not reported in this analysis; for example, demographic breakouts by type of insurance is excluded.
- This survey from California Health Care Foundation used both a probability-based sample and nonprobability sample of nonelderly adults (age 18–64) in California. ↩︎
- All respondents of the California Health Interview Survey were asked whether they felt they needed help for a mental or emotional or alcohol or drug problem in the past year. ↩︎