KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
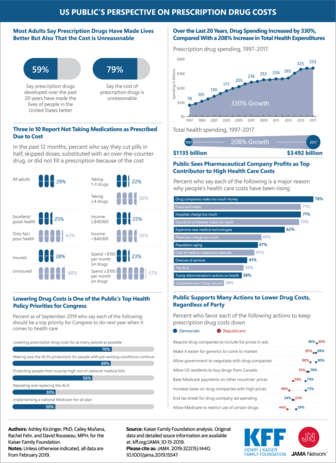
This Visualizing Health Policy infographic examines public opinion on prescription drug costs in the United States (US). Over the past 20 years, US drug spending has increased by 330% compared to a 208% increase in total US health expenditures. A Large majority (78%) of the public see drug company profits as the top contributor to higher health care spending. Lowering drug costs is the public’s top health policy priority for the US Congress. While most adults (59%) say prescription drugs have made their lives better, many (79%) also say the cost is unreasonable. Three in 10 report they have not taken medications as prescribed in the past year because of the cost. Across political affiliation, the public supports many actions to lower drug costs. Requiring drug companies to include list prices in ads, making it easier for generics to come to market, and allowing the government to negotiate with drug companies were among the most popular strategies.
On August 14, 2019, the Trump administration published a final rule to broaden the programs the federal government will consider in public charge determinations to include Medicaid coverage for non-pregnant adults and certain previously excluded nutrition and housing programs. To learn about the possible early effects of the public charge rule and other immigration policies on patients at community health centers, this brief draws on interviews and survey data to capture health center directors’ and staff’s perceptions of changes in coverage and service use among their patients who are immigrants. Key findings include:
Health centers reported that, in recent months, immigrant patients have declined to enroll or reenroll themselves and/or their children in Medicaid for fear of public charge. At some health centers interviewed, these changes were widespread with many patients dropping Medicaid while at others, the changes were occurring among only a small number of patients. Respondents noted those dropping Medicaid include immigrants not subject to the public charge rule, such as pregnant women.
Health center respondents reported patients are confused about the new rule and are afraid to provide identifying information. Patients are not sure which programs the new rules apply to and who is subject to them. Respondents also noted immigrant patients are hesitant to provide any identifying information that could jeopardize their status.
According to respondents, the public charge rule is creating a “chilling” effect, leading to decreased enrollment in other programs not subject to public charge. Health centers reported that in addition to declining to sign up for Medicaid, patients are also not signing up for WIC and other state and local food assistance programs which are not subject to the public charge rule.
About half of health centers reported a drop in utilization by immigrant patients, especially among pregnant women. They noted declines in use of services by patients with chronic conditions, such as diabetes and HIV, and those needing preventive care. Health centers expressed particular concerns regarding pregnant women, who they say are initiating prenatal care later in pregnancy and are attending fewer prenatal care visits due to fears around public charge.
Health centers are training staff to answer questions on public charge and are working to ensure access to care for their patients. Some respondents said they are now providing home visits and free medication delivery to ensure their patients continue to get care.
Issue Brief
Introduction
Since taking office, the Trump Administration has implemented a range of policy changes focused on enhancing immigration enforcement and limiting immigration. Most recently, on August 14, 2019, the administration published a final rule to change “public charge” policies that govern how the use of public benefits may affect individuals’ ability to enter the U.S. or adjust to legal permanent resident (LPR) status (i.e., obtain a “green card”). The rule, which was proposed in October 2018, broadens the programs that the federal government will consider in public charge determinations to include previously excluded health, nutrition, and housing programs, including Medicaid coverage for non-pregnant adults for a wide range of health care needs. The rule will likely lead to decreased enrollment in Medicaid, CHIP, and other programs broadly among immigrant families, beyond individuals directly impacted by the rule. Prior to this final rule, there were growing reports of individuals disenrolling or choosing not to enroll themselves or their children in Medicaid and CHIP due to growing fears and uncertainty stemming from the shifting immigration policy environment.1 The final rule was scheduled to go into effect on October 15, 2019, but on October 11th a nationwide preliminary injunction was issued, blocking implementation.
Community health centers are often on the front lines of policy changes affecting Medicaid coverage. They serve a diverse, predominantly low-income patient population, including low-income immigrants in many communities, and nearly three-quarters of health center patients are covered by Medicaid or are uninsured. Given their role serving immigrant families, the experiences of health centers and their patients can provide early insight into the potential effects the public charge rule and other immigration policies are having on health coverage and use of services by immigrant patients.
To learn about these possible early effects, this brief draws on interviews and survey data to capture health center directors’ and staff’s perceptions of changes in coverage and service use among patients who are immigrants. It relies on interviews with 16 directors and senior staff at health centers in four states—California, Massachusetts, Missouri, and New York– conducted in September 2019, after the final public charge rule was issued. The interviews asked about perceived trends in health coverage of immigrant patients and their families as well as changes in utilization of health care and social services. It also includes results from the 2019 KFF/George Washington University Community Health Center Survey about perceived changes in Medicaid enrollment and health care use among immigrant patients and their families. The survey of staff from 511 health centers was fielded from May through July 2019, after the administration had released the proposed rule to make changes to public charge policy but prior to it being finalized.
Key Findings
Changes in Medicaid Enrollment
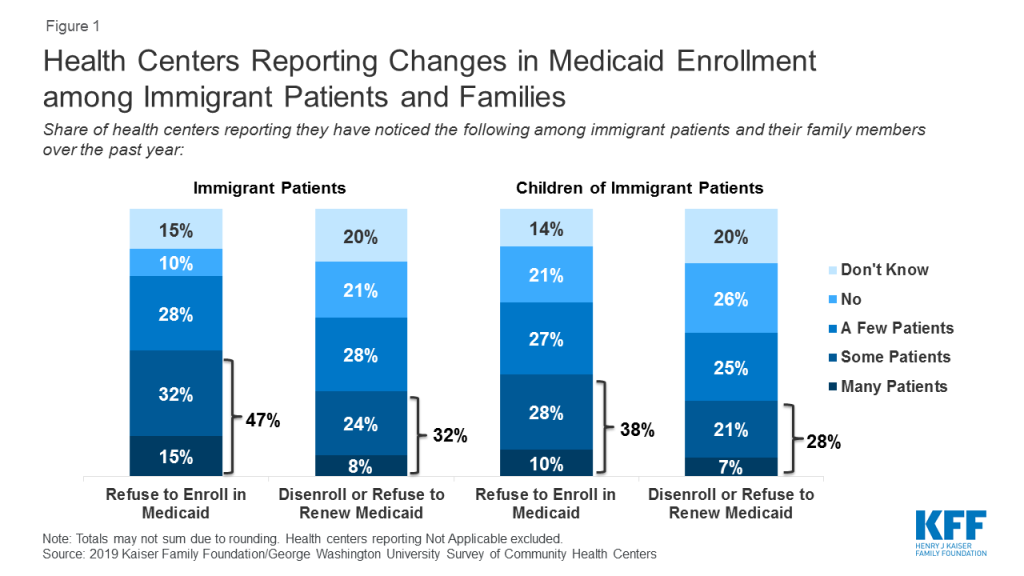
Based on findings from the health center survey, nearly half (47%) of health centers reported that many or some immigrant patients declined to enroll themselves in Medicaid in the past year (Figure 1). In addition, nearly one-third (32%) said that many or some immigrant patients disenrolled from or declined to renew Medicaid coverage. Health centers also report enrollment declines among children in immigrant families. More than a third of (38%) health centers reported that many or some immigrant patients were declining to enroll their children in Medicaid over the past year, while nearly three in ten (28%) reported many or some immigrant patients were disenrolling or deciding not to renew Medicaid coverage for their children.
Figure 1: Health Centers Reporting Changes in Medicaid Enrollment among Immigrant Patients and Families
Follow-up interviews with health center staff are consistent with these survey findings of declining Medicaid enrollment among immigrant patients and their families. Staff at all health centers reported that, in recent months, immigrant patients have declined to enroll or reenroll themselves and/or their children in Medicaid. Health centers do not collect data on immigration status of patients, so these observations (as well as the survey results) are based on health centers’ perceptions of who they believe to be immigrant families using available information. Immigrant families generally view health center staff as a trusted resource, and in turn, are willing to discuss their immigration status with these staff and clinicians. In addition, enrollment staff who assist patient in applying for Medicaid and other coverage have access to this information as part of the application process. At some health centers interviewed, these changes were widespread with many patients dropping Medicaid while at others, the changes were occurring among only a small number of patients. Health center directors at two health centers cited shifts in their payer mix data, with the share of uninsured health center patients increasing, as possible evidence of these changes. Others cited data and information reported by frontline enrollment staff. Even health center directors who noted few patients at their health centers were dropping coverage recounted conversations they had with patients who declined to enroll in Medicaid. Health centers serving smaller shares of immigrant patients were more likely to report that only a few patients were choosing not enroll in Medicaid.
Our patient navigation team which is multilingual and multiethnic used to work with upwards of 10 people a day to get them signed up for coverage… men, women, children, etc. Now they’re down to 2 to 3 clients a day if they’re lucky. (Health Center CEO, MO)
Our insurance companies… we have Healthfirst at all of our sites to enroll folks. And they’re seeing that folks aren’t re-enrolling. They’re actually coming up to our sites to do a public charge information session for all the folks because they’re seeing disenrollments. (Health Center President, NY)
We had one lady who came in and she said, ‘I’m going to apply for my children because they are citizens, but I’m not, so I am not going to apply.’ (Intake/Outreach Supervisor, MA)
According to health center interview respondents, immigrant patients are confused by the new rules and many are receiving misinformation. All respondents reported confusion among their immigrant patients over new the new rules. They said patients are asking questions of health center staff and noted that many patients are not sure which programs the new rules apply to and who is subject to them. Based on reports from patients and their own conversations with advocates and the legal community, several health center directors noted that some of the confusion stems from some immigration lawyers advising clients to avoid all public programs and services out of an abundance of caution. At the same time, they also said rumors and misinformation spread quickly through communities. For example, a health center director in California recounted how misinformation was quickly spread through WeChat, a social media and messaging app which is commonly used in the predominantly Asian immigrant community served by the health center.
What we have heard from our staff on the front line, the folks who interface with our patients around the enrollment, they are hearing that people are afraid around disclosing more information about their families who would not even be impacted, but because there’s a lot of misinformation out in the community… they’re not clear in terms of how that’s going to impact them. (Health Center Compliance Officer, CA)
Health center respondents reported that immigrant patients are increasingly afraid to disclose personal information. Interview respondents across all health centers reported that some immigrant patients have become reluctant to disclose any personal information out of fear that the health center would share that information with authorities. This information is necessary not only to assess eligibility for Medicaid and other federal programs, but also for state and local social services programs. According to respondents, the fear stems from multiple sources—fear of deportation among immigrants who lack legal status and fear that sharing any information could jeopardize their or a family member’s efforts to obtain a green card or citizenship.
The reason provided is fear and uncertainty related to immigration and customs enforcement agents potentially showing up and carting them away as they enter or leave the building or the federal government getting the information they provide us. (Health Center President, MO)
People are not generally going to feel comfortable providing their name and information, so we’re going to be thoughtful about how we collect that information from our patients, so that we’re not also making them afraid to give information about their own status – we’ll serve them regardless. (Health Center CEO, CA)
Health center interview respondents reported that the patients disenrolling or declining to enroll in Medicaid are a broader group of immigrants than those targeted by the public charge rule. Health center respondents reported that some patients declining to enroll in Medicaid already have Lawful Permanent Status (LPR), and therefore would not be subject to the new public charge rule. They noted these decisions may stem from fear that the patients will lose their current lawful status or that they may be barred from applying for citizenship if they receive any services. Another explanation offered is that these patients are concerned that they will jeopardize the safety or status of a family member. Respondents also reported that patients have expressed concerns that enrolling their children in these programs, even if their children were born in the United States, may jeopardize their status or the status of family members. In addition, although pregnant women are categorically eligible for Medicaid and would be unaffected by public charge if they enroll in Medicaid, health center respondents reported that pregnant women are declining to enroll in Medicaid or disenrolling, in some cases out of fear of risking future opportunities for residency or citizenship.
Approximately 10% of those foreign born women who were pregnant will tell us they do not intend to, they do not want to apply for Medicaid… because they are afraid. Their fears range from being deported, to future opportunities for residency or citizenship. It’s a wide range of things they are afraid of, but ultimately it’s jeopardizing their status. (Health Center Vice President, MO)
Fear of public charge implications extends beyond Medicaid to other health and social service programs, including some that are not included in the public charge rule. In addition to helping patients enroll in Medicaid and other health coverage programs, most health centers also assist patients with enrollment in a range of social service programs, including food and housing assistance programs, job training programs, and education programs. Based on this enrollment assistance experience, some interview respondents reported immigrants are avoiding housing and food assistance programs. While the public charge rule includes some housing assistance programs and the Supplemental Nutrition Assistance Program (SNAP), it does not include other key nutrition programs such as WIC and school lunch. A major concern among respondents was data suggesting that immigrant pregnant women are refusing WIC services. Several respondents noted that their WIC caseloads are down and attributed the trend to public charge fears. Respondents in California and Missouri also noted that immigrant patients are declining to enroll in or accept referrals for state and local food assistance programs, even though these programs are not subject to public charge. A health center serving New York City reported that patients with HIV or AIDS are hesitating to enroll in or are disenrolling from the city-run HIV/AIDS Services Administration (HASA) program out of fear that the program’s services fall under the public charge rule.
We began to see a decline in people coming in for their basic health screenings, for nutrition services. Even if they were hungry, they were not telling us, so we had to change. As we saw the WIC numbers [decline]… we started asking questions as part of their visit. (Health Center President, MA)
Changes in Health Care utilization
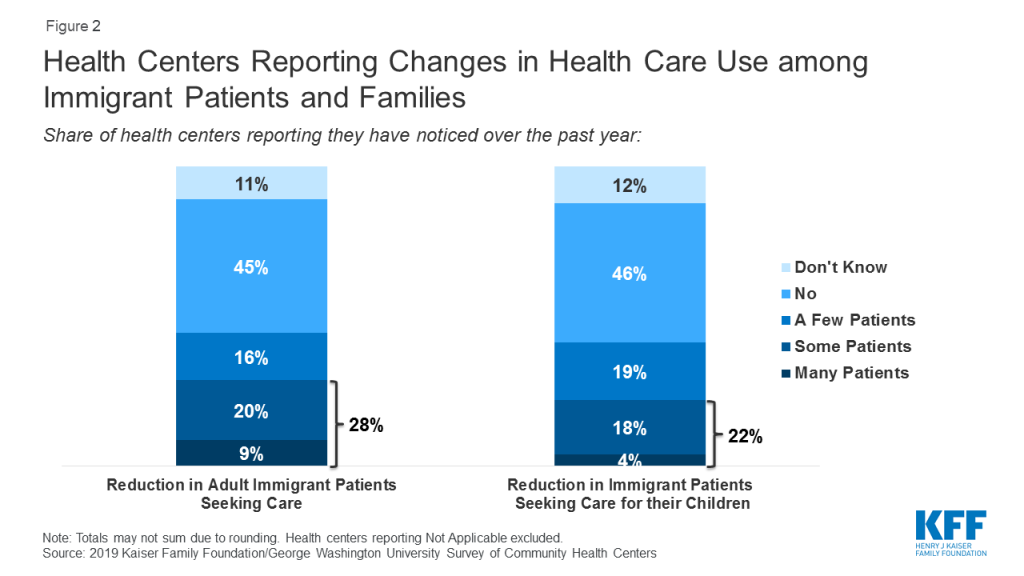
According to the survey, nearly three in ten (28%) health centers reported declines among many or some adult immigrant patients in seeking health care in the past year. Over one in five (22%) reported reductions in health care use among some or many children in immigrant families (Figure 2).
Figure 2: Health Centers Reporting Changes in Health Care Use among Immigrant Patients and Families
The findings from the interviews were consistent with findings from the health center survey about changing utilization among immigrant patients and their families. For example, health center directors in Massachusetts and Missouri described significant drops in utilization as evidenced by an increase in appointment cancellations and no shows by immigrant patients. Another health center director noted that, while their patient base remains strong, patient encounters have declined, so much so that their clinicians are working at only about 80% capacity. At the same time, other health center directors in Massachusetts and Missouri have observed little change in service use by their immigrant patients. A health center director in California said, while they are seeing utilization changes, it is too early to attribute those changes solely to the public charge rule and that other factors, including increased ICE enforcement activities, may be playing a role.
We are extremely worried about the trend we’ve noticed over the last 6-8 months, which is that people are afraid to keep their appointments, to sign up for appointments, to come into the buildings or the various clinical sites and fill out basic paperwork, or even provide their address or ID or other personal information. (Health Center President, MO)
Our overall number of patients we serve remains pretty steady. Our actual encounters have gone down… In the past, say 5 years ago, you couldn’t get an appointment because we were so packed. Now, I would say the majority doctors are 80 percent full. (Health Center President, CA)
Health center interview respondents reported that pregnant women are delaying prenatal care or seeking care less frequently. Nearly all respondents that provide obstetric care noted that immigrant pregnant women are initiating prenatal care later in their pregnancies. They indicated that efforts to educate pregnant women often are insufficient to overcome fears about enrollment and that many women continue to decline to enroll in Medicaid or access care even after being told they are exempt from the public charge rule. Respondents expressed particular concerns about the potential consequences of this trend on health outcomes, noting that it was eroding years of work and progress to encourage pregnant women to access prenatal care early in their pregnancies.
We have a seen a decline in our pregnant visits… insured or otherwise. When we drill down and actually talk to them – “Why did you wait until your sixth month to come in?” they say ,”Oh because I’m afraid.” (Health Center CEO, NY)
Health center directors reported that some of their patients with chronic conditions are foregoing care and others are not getting preventive care. In particular, respondents whose programs offer group sessions for diabetes patients noted a drop in participation in their Spanish-language group sessions. A health center in New York reported a decline in the use of PrEP among their immigrant patients at risk for exposure to HIV. Respondents also suggested that fear of using services may prevent patients with acute care needs from getting care. One respondent pointed out that, during the height of the flu season last winter, visits at an urgent care clinic in California dropped significantly and coincided with rumors related to the public charge rule spreading on social media.
One of the central tenets of diabetes care for example is that, in addition to managing the person’s medical condition, we do group education sessions for them to teach them how to shop healthy, eat healthy… that is critical to the health status outcomes to the diabetes patients. We have seen a steady drop in attendance and participation (Health Center CEO, MO)
This action [public charge] totally undermines the work that we’re trying to do around managing population health. I think when you’re really going to see it is around flu season. (Health Center CEO, CA)
Effects on health center patients, staff and operations
Health center interview respondents reported their staff are observing increased rates of anxiety and stress-related conditions among their immigrant patients. As a result, behavioral health counselors are getting more requests for counseling and therapy. Respondents also expressed significant worries about the effects on children, describing their pediatric patients as being traumatized by what is happening to their families and in their communities.
The children are terrified… One pediatrician relayed his conversation with a 7-year-old when the mother went outside to take a phone call. The child said, “Can you give something to my mother because she’s afraid all the time. She doesn’t want to let me out…” (Health Center CEO, NY)
Several respondents said they were implementing new protocols and services to ensure the highest need patients continue to receive care despite growing fears. A health center director in Massachusetts reported that case managers will contact the highest risk patients and will arrange for home visits and free delivery of medications if patients are too afraid to come to the clinic. A health center in New York serving a large migrant community sends staff out to farms in rural areas to deliver babies and treat injuries for patients who will not come to the health center or other providers out of fear of jeopardizing their ability to continue working in the US.
They had a person that was severely injured on the farm and they could not get him to go to the hospital because of the fear of going out there… (Health Center President, NY)
Nearly all health center interview respondents said they are training staff, starting with frontline staff, but working through the organization to include clinicians and others, to ensure they understand the new rules and can respond accurately to patient questions. Respondents operating large programs noted the difficulty associated with training all staff and worried about patients potentially getting conflicting information from different staff, which could possibly lead to an erosion of trust between the patient and the health center. At the same time, several respondents voiced concerns over the effect of the challenging environment facing immigrants on their staff, many of whom are immigrants themselves and live in the communities served by the health centers.
We can’t get information out fast enough to alleviate the fears. Just getting our own staff trained to understand all the nuances of this, it’s incredibly difficult. (Health Center President, CA)
Giving staff lists on what public benefits are impacted, frequently asked questions so they can orient both the patients and they can orient themselves on what they can tell our patients and not continue the fear and chill factor that we’re seeing. We’re also going to do trainings with our HSF folks, the frontline level staff so they feel comfortable responding to these questions. (Health Center Compliance Officer, CA)
Several health center interview respondents reported the decline in patients covered by Medicaid combined with an increase in the number of uninsured patients and an overall drop in patient visits has led to revenue losses. For some, the revenue declines have been manageable, but two respondents reported experiencing operating losses this year that they attribute to immigration policies. A respondent in Missouri noted that as patients drop Medicaid and move onto the sliding fee scale, they often struggle to make those payments, increasing financial pressures on the families and on the health center. Respondents were clear in noting that not all of these effects are attributable solely to the public charge and that there are multiple factors.
Because of what’s going on and the reluctance of people to sign up for Medicaid even when they are fully eligible… they are switching to self-pay. That means that percentage of self-pay is going up. That hits our bottom line. If the [percentage of] self-pay comes up to 50 percent, you know your health center is suffering financially… We’re not making enough to pay our own bills. (Health Center CEO, MO)
My revenue is down so significantly because… the lack of reenrollment for Medicaid benefits and uptick in uninsured visits is one-to-one. What we realized is that … patients are coming in, but they’re not coming in and using their Medicaid benefits. (Health Center CEO, NY)
Conclusion
Consistent with other recent research, these findings reporting the perceptions and experiences of community health centers suggest that shifting immigration policies are leading to decreased participation in Medicaid among some immigrant families and their children who use services at community health centers. Health center directors and staff reported that declines in Medicaid coverage are occurring broadly among immigrant patients and their children, beyond those targeted by the public charge rule and including those who are explicitly exempt, such as pregnant women. These findings also indicate that growing fear and uncertainty among immigrant families in response to shifting immigration policy are contributing to declines in health care use among some immigrant patients and their families, including among pregnant women. Decreased coverage and declines in health care use could have a negative impact on the health and well-being of families and children, and will likely have longer-term consequences. Moreover, these changes carry the potential for broader, community-wide implications as decreases in coverage increase financial strain on health centers, thereby adding to challenges to providing care.
Methods
The findings in this brief are based on structured phone interviews with health center directors and senior staff conducted by Kaiser Family Foundation in four states: California, Massachusetts, Missouri, and New York. In total, we conducted interviews with 16 health centers across the four states—two each in California, Massachusetts, and Missouri, and ten in New York. Health centers were selected to represent a mix of characteristics, including location in urban vs. rural areas, size, and share of immigrant patients served. The health centers’ patient populations ranged in size from 15,000 – 91,000 total patients and estimates of immigrant patients served ranged from 10% to over 80%. The interviews were conducted in September 2019.
The brief also reports findings from the 2019 Kaiser Family Foundation/George Washington University Survey of Community Health Centers. The survey was designed and analyzed by researchers at KFF and GWU, and conducted by the Geiger Gibson Program in Community Health Policy at GWU. It was fielded from May to July 2019 and was emailed to 1,342 CEOs of federally funded health centers in the 50 states and the District of Columbia identified in the 2017 Uniform Data System. The response rate was 38%, with 511 responses from 49 states and DC.
Additional support for the survey was provided by the RCHN Community Health Foundation as part of its ongoing research collaborative with the Geiger Gibson Program.
2019 Survey of Community Health Centers
(Questions 1-15 and 17-34 reserved for future release)
Q16. Over the past year, has your health center noticed any of the following among your immigrant patients and their family members?
Please indicate whether the following have been seen among many patients, some patients, a few patients, no patients, not applicable, or don’t know.
Patients who refuse to enroll in Medicaid for themselves
Patients who refuse to enroll in Medicaid for their children
Patients who disenroll or refuse to renew their own Medicaid coverage
Patients who disenroll or refuse to renew Medicaid coverage for their children
A reduction in the number of adult patients seeking care from the health center
A reduction in the number of patients seeking care for their children from the health center
In the lead up to the fourth round of Democratic primary debates, majorities of Democrats and Democratic-leaning independents say Democratic candidates for president are spending too little time talking about women’s health care and surprise medical bills, while most feel they are spending the right amount or too much time talking about coverage expansions and Medicare-for-all.
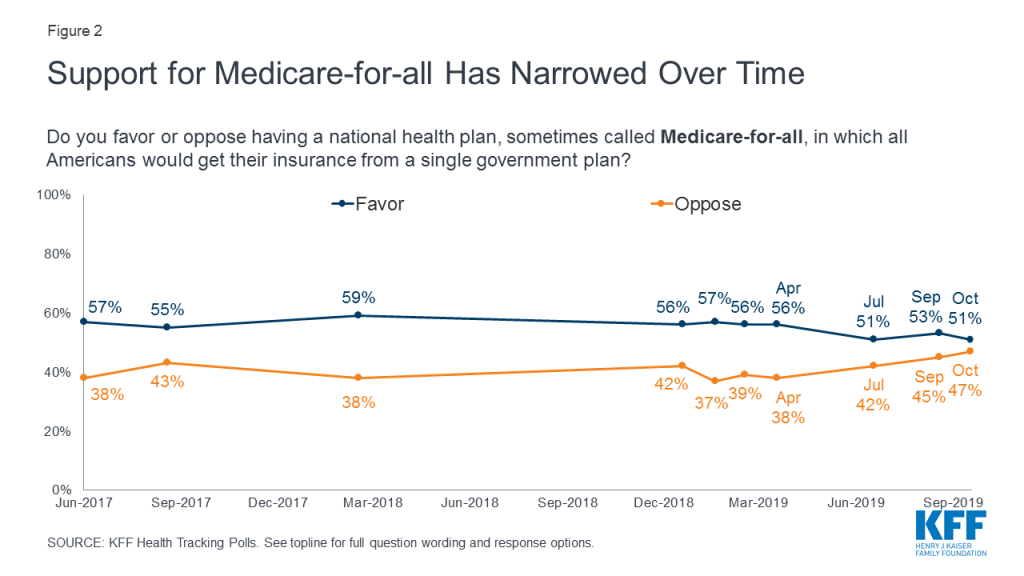
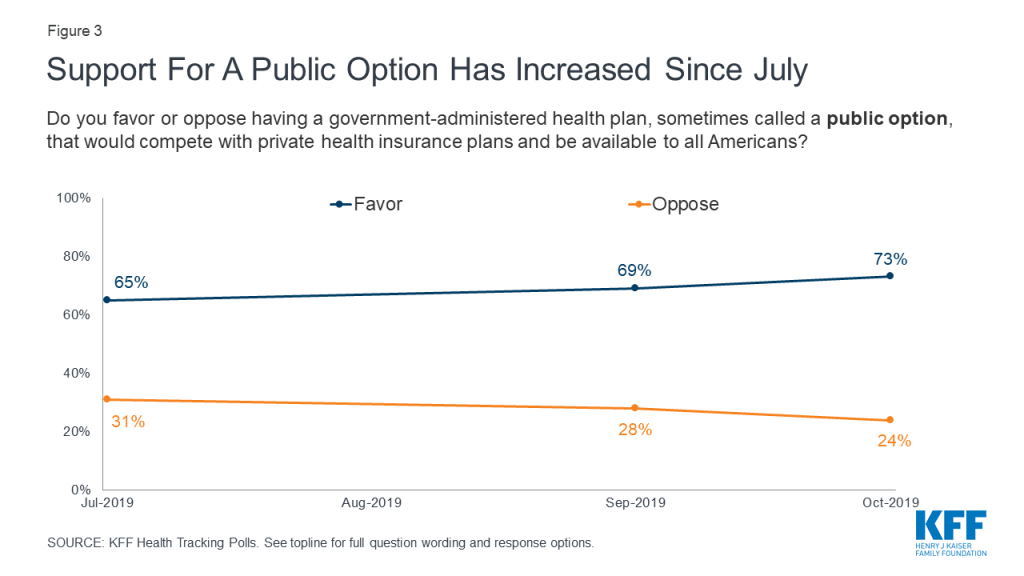
Support for Medicare-for-all has narrowed in recent months, with 51% now saying they favor a national health plan and 47% opposed. At the same time, support for a public option has inched up since July, with 73% now saying they favor a government plan that would compete with private health care plans and 24% opposed.
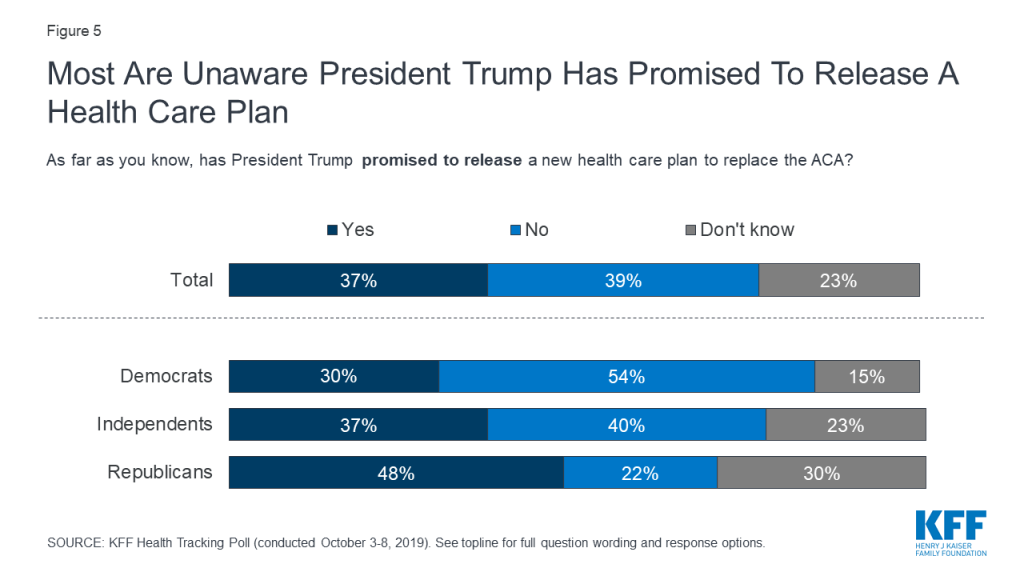
Fewer than four in ten adults (37%) are aware that President Trump has promised to release a health care plan to replace the Affordable Care Act, while most say the president has not promised such a plan or are unsure. Most (62%) are not too confident or not at all confident that the president will be able to deliver on his promise that Americans will get better health care at a lower cost under his plan.
Following House Speaker Nancy Pelosi’s announcement of a formal impeachment inquiry into President Trump, the public is divided on whether an impeachment investigation will keep Congress from addressing key health care issues (47%) or whether Congress can work on impeachment and pass legislation to address issues such as prescription drug costs and surprise medical bills at the same time (45%). Partisans diverge, but among independents, more think that working on impeachment will keep Congress from passing legislation than say Congress can work on both at the same time (53% vs. 40%).
Large majorities of the public favor various policy options aimed at lowering the cost of prescription drugs, including over eight in ten who favor allowing the federal government to negotiate with drug companies to get a lower price on medications for people with Medicare and allowing negotiations that would apply to both Medicare and private insurance. However, support can shift with arguments for and against government negotiation of drug prices.
Health Care And The 2020 Election
Democratic Presidential Primary Debates
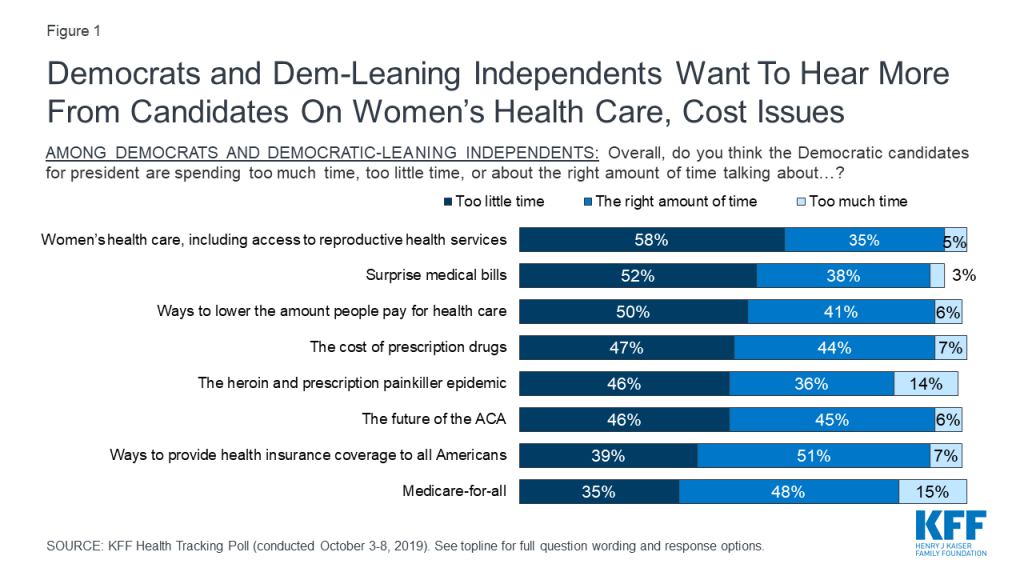
In recent KFF Health Tracking Polls health care has consistently emerged as a top issue that Democrats and Democratic-leaning independents want to hear the 2020 Democratic presidential candidates address. This month’s tracking poll, conducted in the week prior to the fourth round of Democratic presidential debates, finds a majority of Democrats and Democratic-leaning independents say the Democratic candidates for president are spending too little time talking about women’s health care (58%) and surprise medical bills (52%) and half say the candidates are spending too little time discussing ways to lower health care costs (50%). Nearly half say candidates are spending too little time discussing the cost of prescription drugs (47%), the opioid epidemic (46%), and the future of the ACA (46%). The upcoming debates present an opportunity for Democratic candidates to address other health care issues that Democrats and Democratic-leaning independents want to hear more about as most say the candidates have spent the right amount of time or too much time talking about Medicare-for-all and ways to provide health insurance coverage to all Americans—two topics which have dominated health care discussions in the past three rounds of Democratic debates.
Figure 1: Democrats and Dem-Leaning Independents Want To Hear More From Candidates On Women’s Health Care, Cost Issues
Support For Medicare-for-all Narrows, While Support For Public Option Grows
Support for a national health plan, or Medicare-for-all, appears to have narrowed somewhat in recent months. This month’s poll finds about half the public (51%) favors a national Medicare-for-all plan while 47% are opposed. This is the narrowest gap between those who favor and oppose such a plan measured in KFF polls since 2017, and represents a 5-percentage point drop in the share in favor and an 8-percentage point increase in the share opposed since April.
Figure 2: Support for Medicare-for-all Has Narrowed Over Time
By contrast, support for a so-called “public option” plan in which a government-administered plan would compete with private health insurance appears to be inching up. Since July, there has been an 8-percentage point increase in the share in favor of such a plan, from 65% to 73%.
Figure 3: Support For A Public Option Has Increased Since July
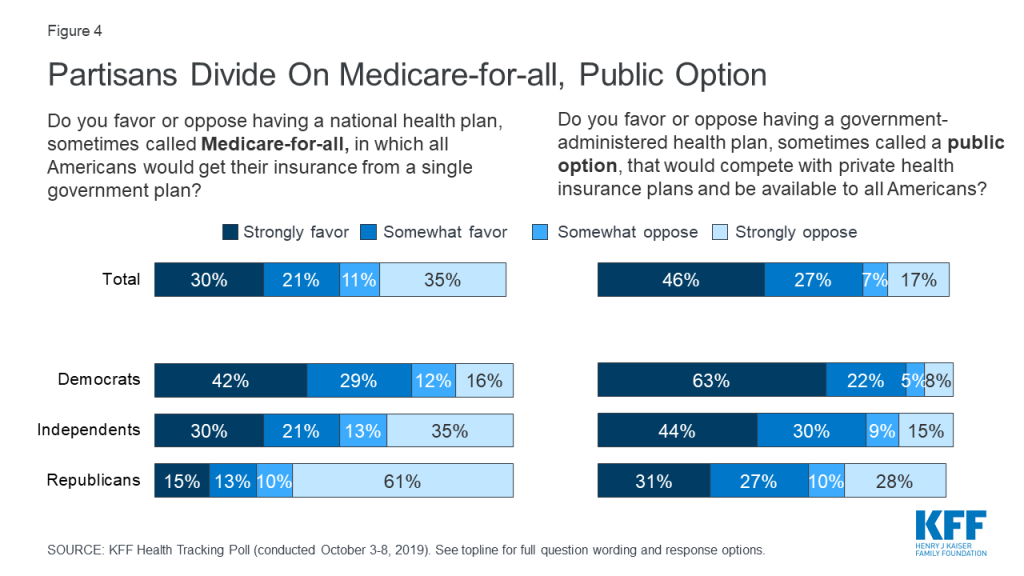
Large majorities of Democrats continue to favor both Medicare-for-all (71%) and a public option (85%). While a Medicare-for-all proposal is less popular among independents (50%) and Republicans (28%), majorities in both groups favor a public option that would compete with private health insurance plans (73% of independents and 58% of Republicans).
Figure 4: Partisans Divide On Medicare-for-all, Public Option
President Trump’s Health Care Plan
In March, President Trump stated that the Republican Party will become “the party of health care.”1 In April, he indicated that a Republican health care plan was forthcoming and that a vote would be planned following the 2020 election.2 Fewer than four in ten adults (37%) are aware that President Trump has promised to release a health care plan to replace the Affordable Care Act, while most say he has not promised to release a plan (39%) or they are unsure (23%). Notably, Republicans are more likely than Democrats and independents to know that President Trump has promised to release a health care plan to replace the ACA.
Figure 5: Most Are Unaware President Trump Has Promised To Release A Health Care Plan
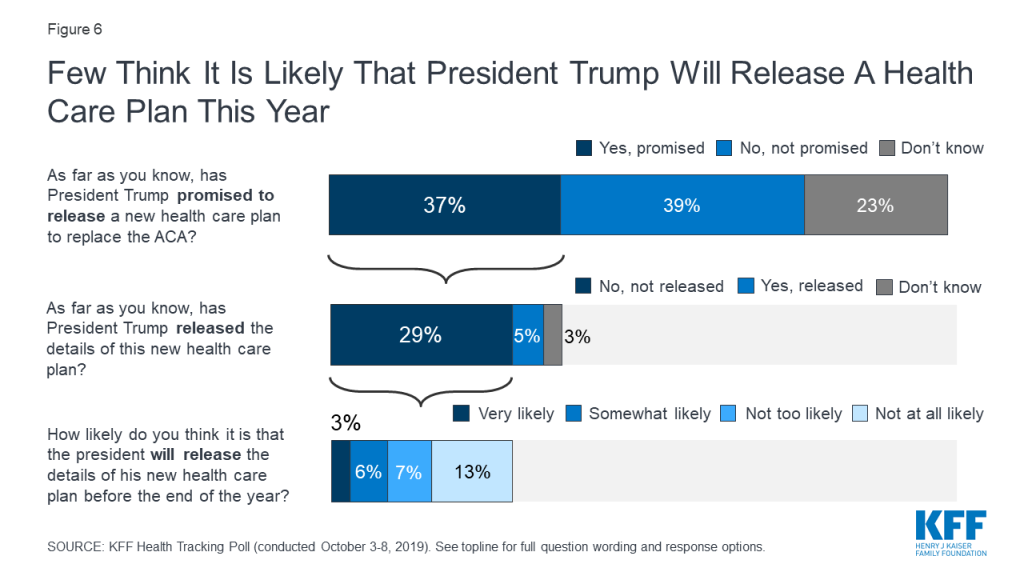
About three in ten (29%) know that President Trump has promised to release a health care plan and that he has not yet released the details of his plan. Moreover, only 9% of adults think it is very or somewhat likely that Trump will release the details of his promised health care plan to replace the ACA by the end of the year.
Figure 6: Few Think It Is Likely That President Trump Will Release A Health Care Plan This Year
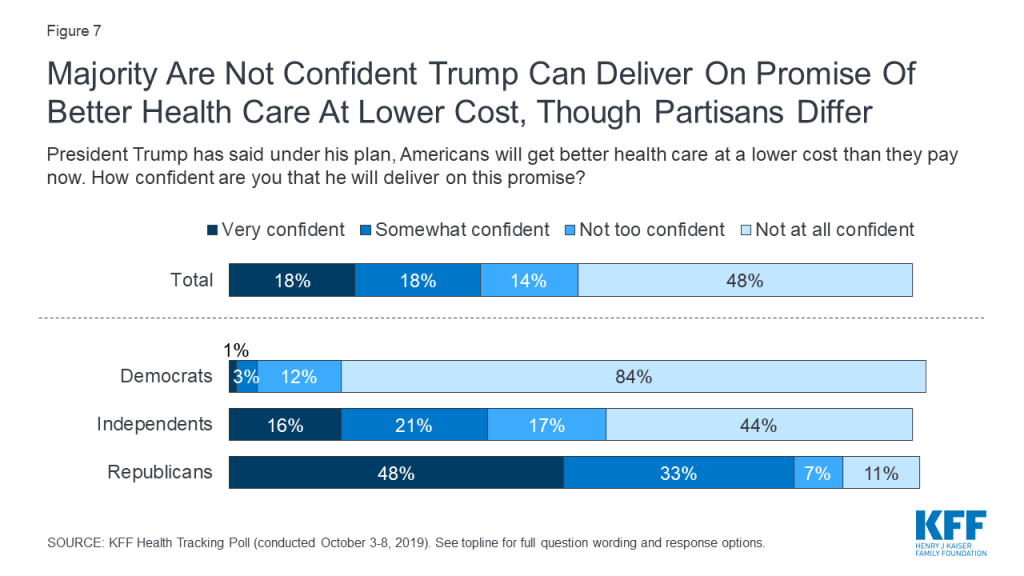
President Trump has stated that under his health care plan, Americans will get better health care at a lower cost than they currently pay3 . About three in ten adults are very or somewhat confident the President will deliver on his promise while a majority (62%) say they are not too confident or not at all confident. While most Republicans are either very confident (48%) or somewhat confident (33%) that President Trump will be able to deliver on his promise, majorities of Democrats and independents say they are not confident that the President will be able to deliver on this.
Figure 7: Majority Are Not Confident Trump Can Deliver On Promise Of Better Health Care At Lower Cost, Though Partisans Differ
Public More Likely To Trust Democratic Party On Health Care
When it comes to health care, the public continues to give the Democratic Party the edge over the Republican Party. Larger shares say they trust the Democrats than the Republicans when it comes to handling health care (44% vs. 29%), lowering the cost of prescription drugs (49% vs. 30%), determining the future of Medicare (47% vs. 35%), and making sure seniors on Medicare are able to get the health care they need (51% vs. 32%). Unsurprisingly, majorities of partisans trust their own party to do a better job on each of these issues. While independents are more likely to trust the Democratic Party than the Republican Party, nearly one third (32%) say they trust neither party when it comes to handling health care.
Figure 8: Public More Likely to Trust Democrats Than Republicans On Health Care, Medicare
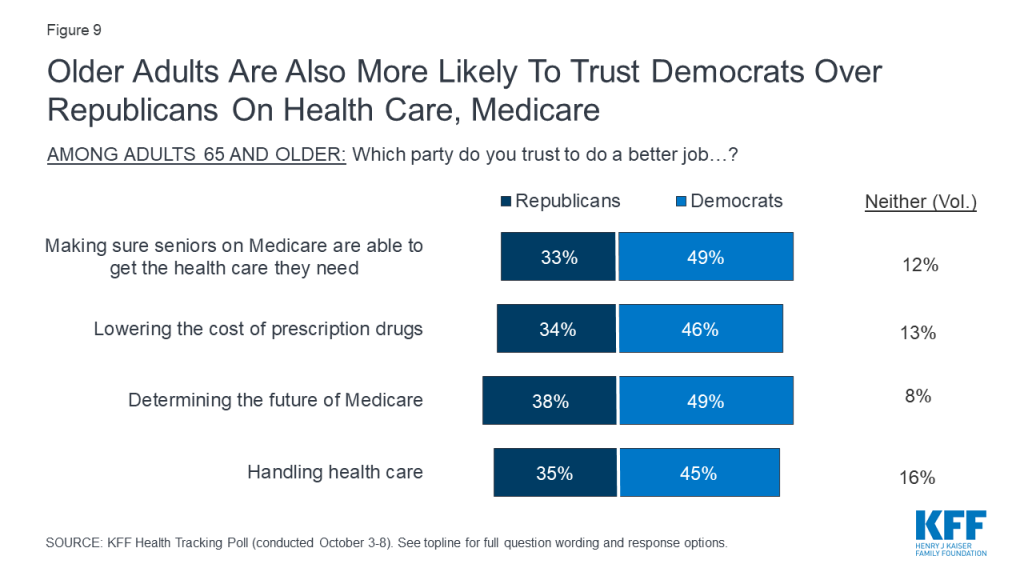
Despite President Trump’s health care speech in Florida earlier this month telling older adults that Democrats would harm their health care4 , those ages 65 and older are more likely to trust the Democratic Party than the Republican Party to do a better job handling health care (45% vs. 35%), making sure seniors are able to get the health care they need (49% vs. 33%), and lowering the cost of prescription drugs (46% vs. 34%).
Figure 9: Older Adults Are Also More Likely To Trust Democrats Over Republicans On Health Care, Medicare
Health Care And The Congress: Impeachment And Lowering Prescription Drug Prices
Public Divided On Whether Impeachment Will Prevent Congressional Action On Prescription Drugs, Surprise Bills
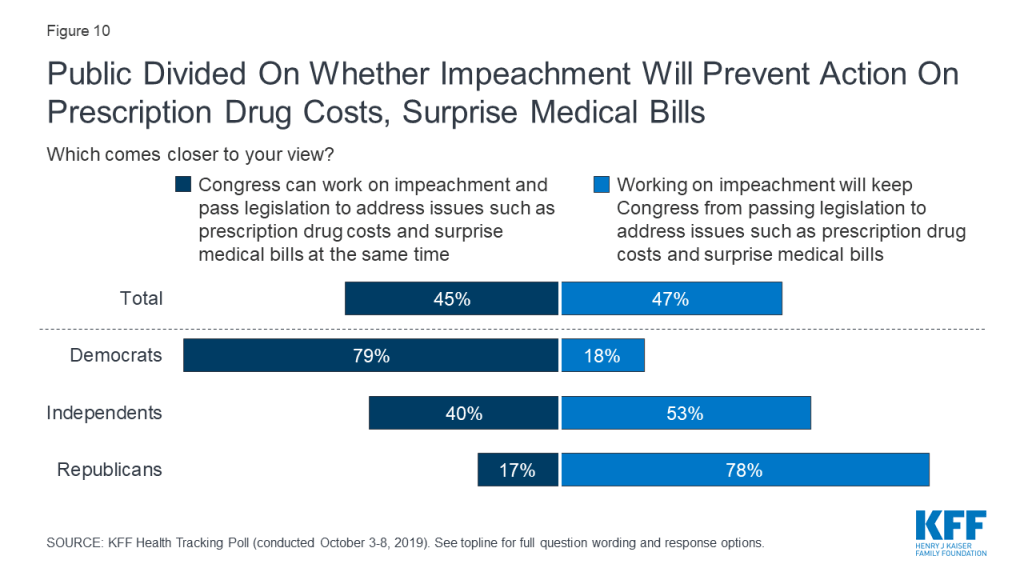
On September 24th, House Speaker Nancy Pelosi announced the House would begin a formal impeachment inquiry into President Trump. The public is divided on whether the recently launched impeachment investigation will keep Congress from addressing key health care issues. Forty-five percent of adults say Congress can work on impeachment and pass legislation to address issues such as prescription drug costs and surprise medical bills at the same time, while a similar proportion (47%) say impeachment will keep Congress from passing legislation to address these issues.
There are stark partisan differences, with nearly eight in ten Republicans (78%) saying impeachment will keep Congress from addressing health care issues while a similar share of Democrats (79%) say Congress can both work on impeachment and pass legislation at the same time. Independents are more likely to say that impeachment will keep Congress from passing legislation than to say they can do both (53% vs. 40%).
Figure 10: Public Divided On Whether Impeachment Will Prevent Action On Prescription Drug Costs, Surprise Medical Bills
Majorities Support Various Approaches To Lowering Drug Costs, But Support Is Malleable
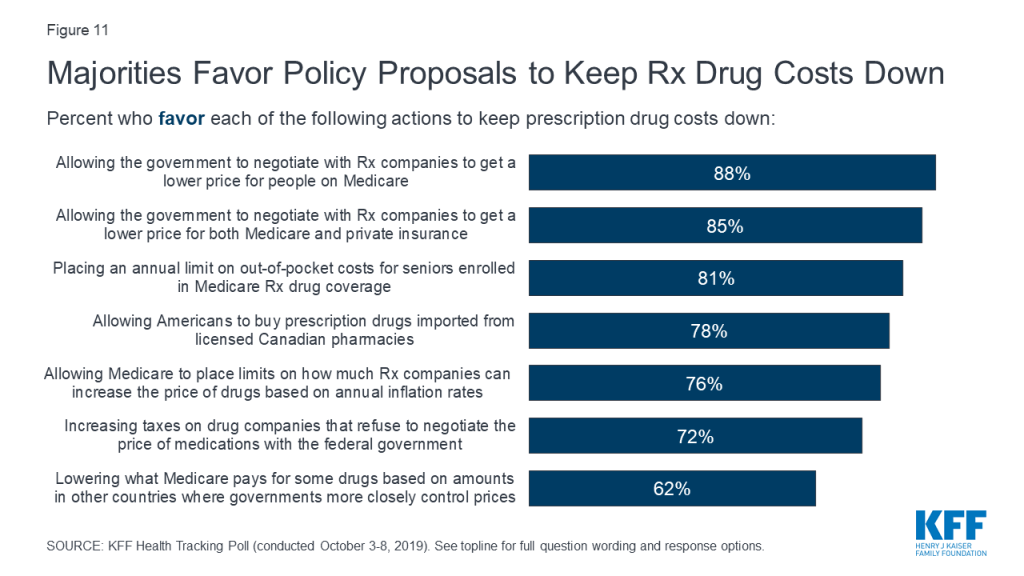
KFF’s September Health Tracking Poll found that lowering prescription drug costs remain a priority for the public, with majorities across parties saying this was an important issue for Congress to address. This issue has been a focus of lawmakers, with hearings held in both the House and Senate, proposals put forward by the Trump administration, and most recently a prescription drug policy proposal unveiled by House Speaker Nancy Pelosi. About eight in ten Americans (78%) say the cost of prescription drugs is unreasonable and majorities favor most of policy options aimed at lowering the cost of prescription drugs included in this month’s survey.
Nearly nine in ten Americans favor allowing the federal government to negotiate with drug companies to get a lower price on medications for people on Medicare (88%). A similar proportion favor allowing the federal government to negotiate prices with drug companies that would apply to both Medicare and private insurance (85%). Both of these policy proposals are supported by large majorities of Democrats, independents, and Republicans. Moreover, seven in ten adults (72%) favor increasing taxes on drug companies that refuse to negotiate with the federal government, including majorities of Democrats (79%), independents (71%), and Republicans (69%).
Figure 11: Majorities Favor Policy Proposals to Keep Rx Drug Costs Down
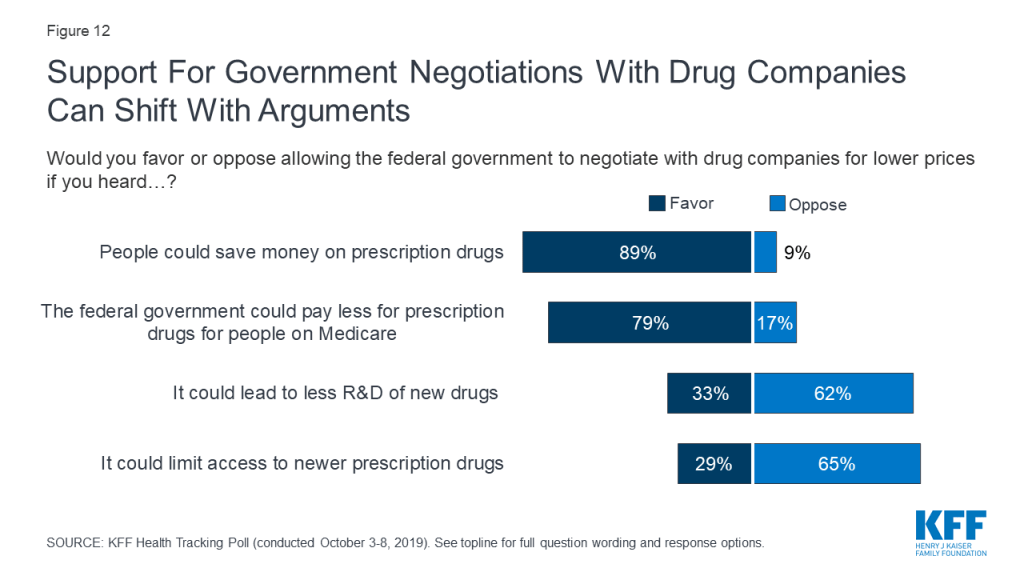
While allowing the federal government to negotiate prices with prescription drug companies is a popular policy proposal, attitudes can shift after hearing potential arguments that have been made both in favor and against the proposal. Support for government negotiations is 89% after hearing the argument that this could help people save money on their prescription drugs. In contrast, opposition is as high as two-thirds after hearing the argument that allowing government negotiation could limit access to new prescription drugs. It is important to note that these arguments do not include specific details about different approaches and constraints that could be imposed on potential negotiations, details of which may influence the public’s attitudes.
Figure 12: Support For Government Negotiations With Drug Companies Can Shift With Arguments
Other proposals aimed at lowering prescription drug costs are also popular among the public. At least three in four favor allowing Medicare to place limits on how much drug companies can increase the price of drugs every year based on annual inflation rates (76%), allowing Americans to buy drugs imported from licensed Canadian pharmacies (78%), and placing an annual limit on out-of-pocket costs for seniors enrolled in Medicare prescription drug coverage (81%). About six in ten (62%) favor lowering what Medicare pays based on amounts paid in other countries where governments more closely control prices. Notably, majorities of Democrats, Republicans and independents favor each of these proposals.
The ACA And The Courts
In December 2018, a federal district court judge in Texas issued a ruling siding with Republican state attorneys general that declared the Affordable Care Act invalid since Congress zeroed out the penalty for not having health insurance. In March 2019, the Trump administration filed a brief stating that the administration supports the federal judge’s ruling that all of the ACA is invalid. The Trump administration had previously stated that as part of the lawsuit known as Texas v. United States, it will no longer defend the ACA’s protections for people with pre-existing medical conditions.
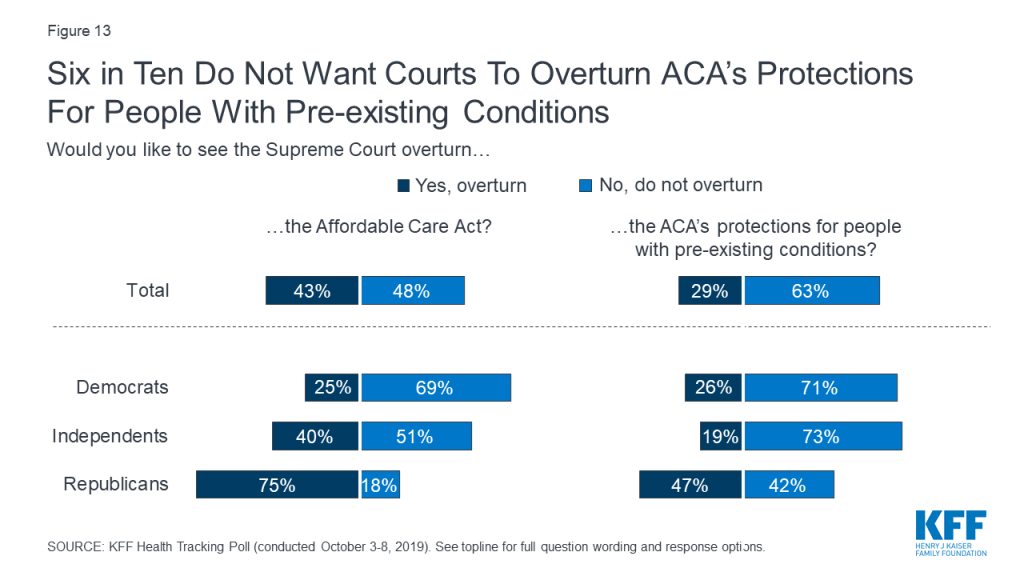
Overall, 63% of the public do not want to see the Supreme Court overturn the ACA’s pre-existing condition protections; yet the public is more divided on whether they want the Court to overturn the entire law (43% would like to see it overturned and 48% would not). While about seven in ten Democrats and about half of independents do not want to see the 2010 health care law overturned, three in four Republicans say they would like to see the courts overturn the law. However, fewer than half of Republicans (47%) want to see the ACA’s protections for people with pre-existing conditions overturned.
Figure 13: Six in Ten Do Not Want Courts To Overturn ACA’s Protections For People With Pre-existing Conditions
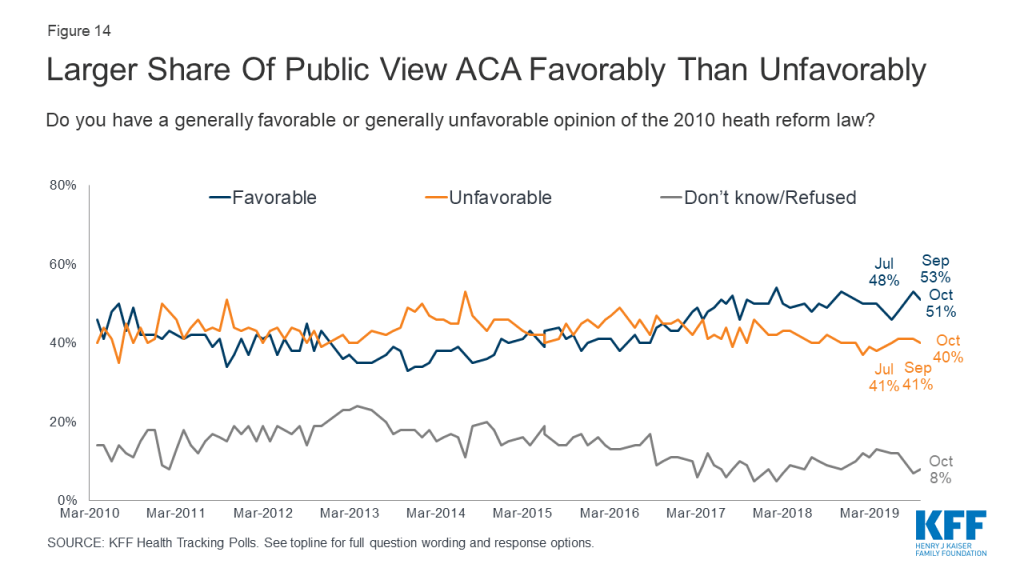
Overall opinions of the Affordable Care Act have remained relatively unchanged for the past two years since the Republican efforts to repeal the law. Half of the public (51%) this month hold favorable opinions of the ACA while four in ten hold a negative opinion of the law. The public still holds largely partisan views of the ACA as eight in ten Democrats (81%) have a favorable view of the ACA compared to half of independents (51%) and about one-sixth of Republicans (15%).
Figure 14: Larger Share Of Public View ACA Favorably Than Unfavorably
Methodology
This KFF Health Tracking Poll was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted October 3rd – 8th 2019, among a nationally representative random digit dial telephone sample of 1,205 adults ages 18 and older, living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). The sample included 290 respondents reached by calling back respondents that had previously completed an interview on the KFF Tracking poll at least nine months ago. Computer-assisted telephone interviews conducted by landline (300) and cell phone (905, including 623 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers) as well as a subsample of respondents who had previously completed Spanish language interviews on the SSRS Omnibus poll (n=10). Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2017 American Community Survey (ACS) on sex, age, education, race, Hispanic origin, and region along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the July-December 2018 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of prepaid cell phones and likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
1,205
±3 percentage points
Party Identification
Democrats
355
±6 percentage points
Republicans
301
±7 percentage points
Independents
447
±6 percentage points
Democrats/Democratic-leaning independents/Independents with no leaning
Poll: Democrats Say They Are Hearing Enough From Presidential Candidates About Medicare-for-All and Expanding Coverage, But Want Them to Talk More about Health Costs and Women’s Health Care
More Seniors Trust Democrats than Republicans on Medicare, Drug Costs and Other Health Issues; Large Majority of Public Initially Favors Government Drug Price Negotiations, But Counterarguments Dampen Support
Heading into tonight’s Democratic primary debate, most Democrats and Democratic-leaning independents say the candidates are spending the right amount or too much time talking about ways to provide coverage to more Americans and Medicare-for-all, two topics that have dominated health care discussions in the past three rounds of Democratic debates, the latest KFF Health Tracking Poll finds.
In contrast, large shares of Democrats and Democratic-leaning independents say that the presidential candidates are spending too little time on other health care issues such as women’s health care, including reproductive health services (58%), surprise medical bills (52%), and lowering the amount people pay for health care (50%).
Medicare-for-all and other approaches to expand public coverage have gotten substantial attention at prior debates, and critics have focused their attacks on Medicare-for-all, which would create a single government health plan that would cover all Americans.
Amidst this attention, the new poll finds about half (51%) of the public now favors a Medicare-for-all plan, down 5 percentage points since April. Nearly as many (47%) now oppose a Medicare-for-all plan, up significantly since April (38%).
The poll also finds more than seven in 10 (73%) now favor a government-run “public option” plan available to all Americans that would compete with private health insurers, while one in four (24%) are opposed.
More Americans, Including Seniors, Trust Democrats than Republicans on Health Care
President Trump warned seniors in an Oct. 3 speech in Florida that Democrats would harm their health care. Fielded after the President’s speech, the poll finds more seniors trust the Democratic Party than the Republican Party on health care overall (45% v. 35%), as well as on making sure seniors can get needed care (49% v. 33%), and lowering drug costs (46% v. 34%).
The broader public also trust Democrats more than Republicans on health care overall (44% v. 29%), as well as on the future of Medicare (47% v. 35%), making sure seniors can get needed care (51% v. 32%), and lowering drug costs (49% v. 30%).
Not surprisingly, majorities of partisans trust their own party to do a better job on each of these issues. Independents are more likely to trust the Democrats than Republicans, though about a third (32%) say they don’t trust either party when it comes to handling health care.
Large Majorities across Parties Favor Government Negotiations to Lower Drug Prices, Though Counterarguments Significantly Dampen Support
As Congress weighs options to lower what people pay for prescription drugs, large majorities continue to favor a range of actions, including allowing the government to negotiate with drug companies to get a lower price for people with Medicare (88%), or for both people with Medicare and private insurance (85%). This includes large majorities of Democrats, Republicans and independents.
About seven in 10 (72%) – including a similar share of Republicans (69%) also favor increasing taxes on drug companies that refuse to negotiate with the government.
The poll also tests common arguments made for and against allowing the federal government to negotiate with drug companies to obtain lower prices and finds that some arguments can significantly affect public support.
For example, two thirds (65%) say they oppose government negotiations after hearing the argument that it could limit access to new prescription drugs, and nearly as many (62%) oppose it after hearing it could lead to less research and development of new drugs. On the flip side, support is as high as 89% when people are told that government negotiations could help people save on their drug costs.
Other proposals aimed at lowering prescription drug costs are also popular, including: placing an annual limit on out-of-pocket costs for seniors in Medicare drug plans (81%); allowing Americans to buy drugs imported from licensed Canadian pharmacies (78%); allowing Medicare to limit drug companies’ price increases based on annual inflation rates (76%); and setting Medicare prices based on prices in other countries with more government control (62%). Majorities of Democrats, independents and Republicans favor each of these options.
The public is divided on whether Congress can pass legislation on issues such as drug costs and surprise medical bills at the same time it is working on impeachment, with nearly equal shares saying Congress can do both (45%) as saying impeachment will prevent action on those issues (47%). Most Republicans (78%) and just over half of independents (53%) say impeachment will keep Congress from passing such legislation, while most Democrats (79%) say Congress can do both.
Nearly Two Thirds of the Public Do Not Want the Courts to Overturn the ACA’s Pre-Existing Condition Protections, Though Nearly Half of Republicans Do
The poll also looks at the public’s views on a pending court case that could overturn all or parts of the Affordable Care Act. A federal judge in Texas last year ruled in favor of conservative state attorneys general that the entire law was invalid since Congress zeroed out the penalty. The Trump Administration subsequently expressed its support for eliminating the entire ACA, including the provisions that prevent insurance companies from discriminating against people with pre-existing conditions. An appeals court is now weighing its decision in the case, and the results could eventually end up before the Supreme Court.
The poll finds the public narrowly divided on whether the Supreme Court should overturn the entire ACA, with 43% favoring such a decision and 48% opposing it. This reflects partisan views of the law itself, with most Republicans (75%) wanting it overturned, most Democrats (69%) wanting to keep it, and independents falling in between (51% want to keep it, 40% want it overturned).
At the same time, most (63%) do not want to see the Supreme Court overturn the law’s protections for people with pre-existing condition protections. This includes most Democrats (71%) and independents (73%). Among Republicans, 47% say they want the court to overturn those protections and 42% say they do not.
The poll finds half (51%) of the public views the ACA favorably this month, while 40% view it unfavorably. The split is similar to other KFF polls over the past two years since President Trump and Republicans in Congress attempted to repeal the 2010 law.
Designed and analyzed by public opinion researchers at KFF, the poll was conducted October 3-8, 2019 among a nationally representative random digit dial telephone sample of 1,205 adults. Interviews were conducted in English and Spanish by landline (300) and cell phone (905). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
Medicare Part D enrollees with relatively high out-of-pocket expenses can expect see their costs rise in 2020, according to a new KFF analysis. This is mainly due to an increase in how much enrollees will pay out of pocket for their prescription drugs in the Part D benefit coverage gap phase before they qualify for catastrophic coverage.
The analysis finds that out-of-pocket drug costs will increase by nearly $400 — from $2,275 in 2019 to $2,652 in 2020 — for Part D enrollees who take only brand-name drugs and have annual total drug costs that reach the catastrophic coverage threshold.
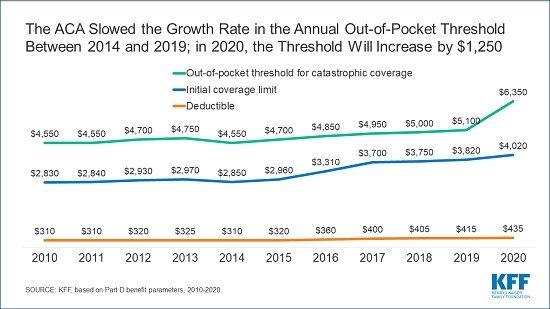
Between 2019 and 2020, this catastrophic threshold will increase by $1,250, or nearly 25 percent, rising from $5,100 in 2019 to $6,350 in 2020.
For enrollees who take only brand-name drugs, about a quarter of this increase will be paid out-of-pocket, with the remainder covered by drug manufacturers in the form of a price discount for brands in the coverage gap phase. Those who take only generics will pay the entire increase out-of-pocket. The relatively large increase in 2020 is due to the expiration of the Affordable Care Act (ACA) provision that slowed the growth rate in the catastrophic threshold between 2014 and 2019.
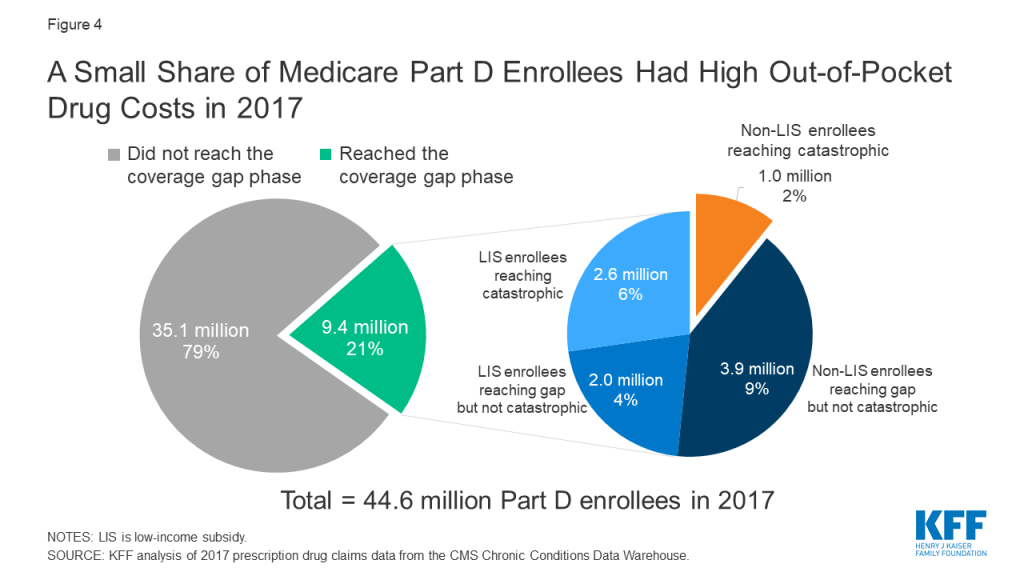
In 2017, the most recent year for which claims data is available, 4.9 million enrollees who were not eligible for low-income subsidies reached the Part D coverage gap, including 1 million who reached the catastrophic threshold. Had the threshold been higher in 2017, fewer than 1 million enrollees would have qualified for catastrophic coverage that year, meaning a larger number of enrollees would have remained in the coverage gap in 2017, where they pay a larger share of their total costs than in the catastrophic phase.
The analysis of higher out-of-pocket costs that Part D enrollees will face in 2020 comes at a time when lawmakers in Congress are considering proposals to address concerns about prescription drug costs. Proposals from the Senate Finance Committee, Speaker Pelosi, and the Trump Administration each include changes to the standard Medicare Part D benefit, including a hard cap on out-of-pocket costs for Part D enrollees and a reallocation of liability above the catastrophic threshold.
Since 2006, Medicare beneficiaries have had access to prescription drug coverage through Part D, where private plan sponsors contract with Medicare to provide the drug benefit. In recent years, policymakers have expressed concerns about the absence of a hard cap on out-of-pocket spending for Part D enrollees, the significant increase in Medicare spending for enrollees with high drug costs, and the relatively weak financial incentives faced by Part D plan sponsors to control high drug costs. Recent proposals aim to address these concerns, including the Trump Administration’s Fiscal Year 2020 budget, the bipartisan prescription drug bill passed by the Senate Finance Committee, and H.R.3, the prescription drug bill recently announced by Speaker Pelosi (D-CA). This brief describes how the Medicare Part D benefit will change in 2020 under current law and proposed changes that would affect what beneficiaries, plans, manufacturers, and Medicare pay for drug costs under Part D in the future.
How Are Total Drug Costs Under Part D Divided Up?
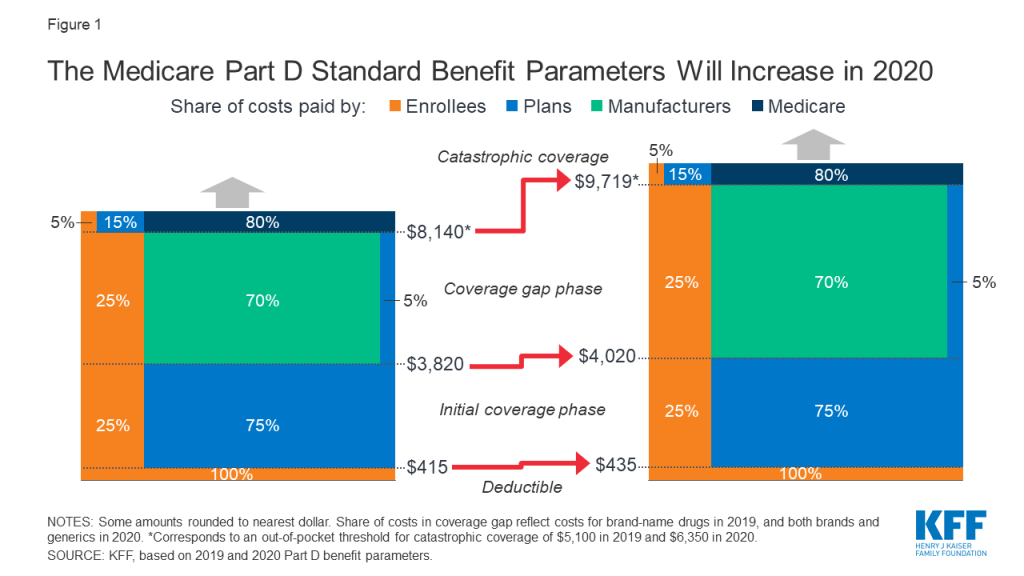
The Medicare Part D standard benefit has different phases where enrollees, Part D plan sponsors, drug manufacturers, and Medicare pay varying shares of total drug costs. These phases include a deductible, an initial coverage phase, a coverage gap phase (once known as the “doughnut hole”), and catastrophic coverage (Figure 1). The allocation of costs in each benefit phase was spelled out in the Medicare Modernization Act of 2003 (the law establishing the Part D program), and has been modified through subsequent legislation.
Figure 1: The Medicare Part D Standard Benefit Parameters Will Increase in 2020
In the deductible phase, Part D enrollees who do not receive low-income subsidies (LIS) pay 100% of their drug costs.
After the deductible, in the initial coverage phase, enrollees pay 25% and Part D plans pay 75%.
After reaching the initial coverage limit but before reaching the catastrophic threshold:
For brand-name drugs, enrollees pay 25% of drug costs, plans pay 5%, and drug manufacturers provide a 70% price discount.
For generic drugs, enrollees pay 37% of drug costs and plans pay 63% in 2019.
When enrollees’ annual out-of-pocket spending—including what they pay directly and the value of the manufacturer discount on brand-name drugs in the coverage gap—exceeds the catastrophic coverage threshold, they pay 5% of their total drug costs, plans pay 15%, and Medicare pays 80%.
Originally, non-LIS Part D enrollees were responsible for paying 100% of their total drug costs in the coverage gap phase. The Affordable Care Act (ACA) included provisions to phase out the coverage gap by 2020 by gradually reducing the share of total drug costs paid by non-LIS enrollees to 25%, requiring drug manufacturers to provide a 50% discount on the price of brand-name drugs, and increasing the share of total drug costs paid by plans to 25% for brands and 75% for generics. The Bipartisan Budget Act of 2018 (BBA) made additional changes to expedite the closing of the coverage gap, beginning in 2019, by reducing beneficiary coinsurance for brands from 30% to 25% in 2019, increasing the manufacturer discount from 50% to 70%, and reducing plans’ share of costs for brand from 25% to 5%.
What’s Changing in Part D for 2020 Under Current Law?
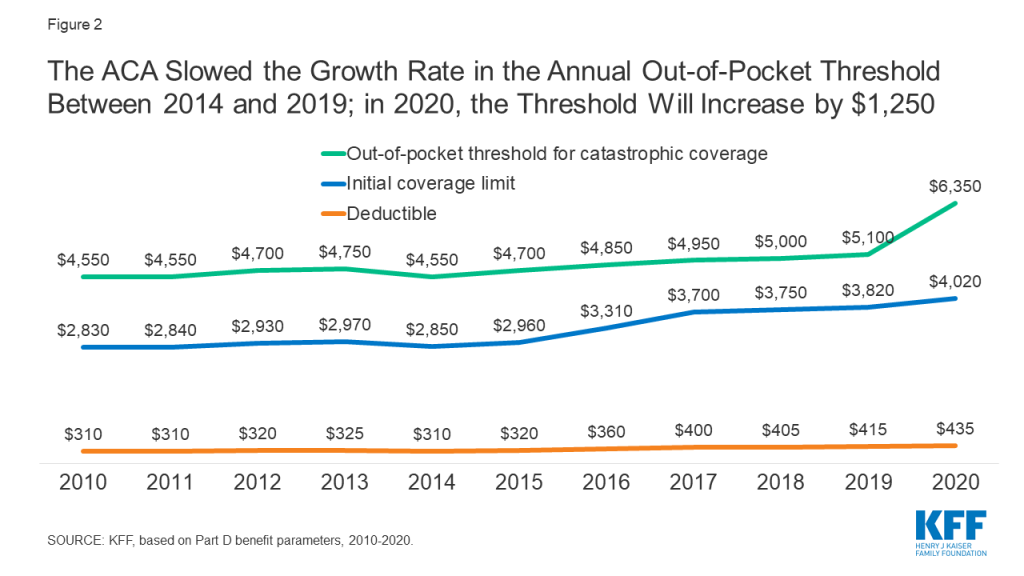
In 2020, Medicare Part D enrollees are facing a relatively large increase in out-of-pocket drug costs before they qualify for catastrophic coverage (Figure 2). This is due to the expiration of the ACA provision that constrained the growth in out-of-pocket costs for Part D enrollees by slowing the growth rate in the catastrophic threshold between 2014 and 2019; in 2020 and beyond, the threshold will revert to the level that it would have been using the pre-ACA growth rate calculation. For 2020, the out-of-pocket spending threshold will increase by $1,250, from $5,100 to $6,350.
Figure 2: The ACA Slowed the Growth Rate in the Annual Out-of-Pocket Threshold Between 2014 and 2019; in 2020, the Threshold Will Increase by $1,250
Part D enrollees will also face higher out-of-pocket costs in 2020 for the deductible and in the initial coverage phase, as they have in prior years. The standard deductible is increasing from $415 in 2019 to $435 in 2020, while the initial coverage limit is increasing from $3,820 in 2019 to $4,020 in 2020. For costs in the coverage gap phase, beneficiaries will pay 25% for both brand-name and generic drugs, with plans paying the remaining 75% of generic drug costs—which means that, effective in 2020, the Part D coverage gap will be fully phased out.
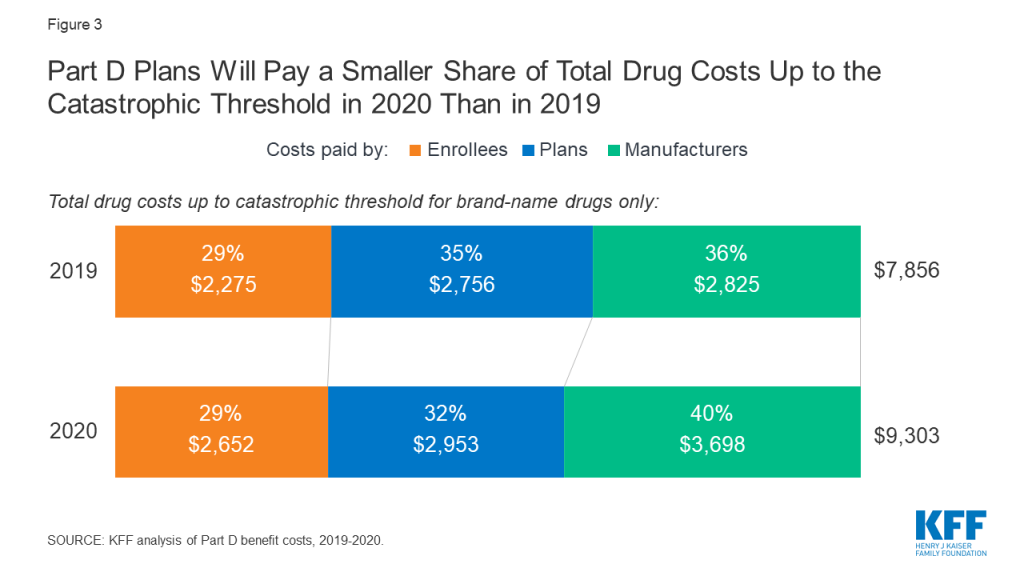
For non-LIS Part D enrollees who take only brand-name drugs and whose annual total drug costs reach the catastrophic coverage limit, these changes in the Part D benefit amounts will increase their annual out-of-pocket costs. Costs for Part D plan sponsors and drug manufacturers will also increase in dollar terms—but in terms of the share of total drug costs up to the catastrophic threshold, Part D plan sponsors will pay a smaller share in 2020 than in 2019, while manufacturers will pay a larger share (Figure 3).
Figure 3: Part D Plans Will Pay a Smaller Share of Total Drug Costs Up to the Catastrophic Threshold in 2020 Than in 2019
Part D enrollees who takes only brand-name drugs and have annual total drug costs that reach the catastrophic coverage limit, will pay nearly $400 more in 2020 than in 2019, from $2,275 in 2019 to $2,652 in 2020. This includes a $20 increase in the deductible, a $45 increase in costs in the initial coverage phase, and a $312 increase in out-of-pocket costs in the coverage gap phase. (Enrollees who take only generic drugs will pay the entire $1,250 increase out-of-pocket.)
Part D plans will pay a smaller share of total drug costs up to the catastrophic threshold for enrollees who take only brands in 2020 (32%) than in 2019 (35%) due to the increase in the out-of-pocket threshold in 2020 and the reduction in plan liability for brand-name drug costs in the coverage gap which took effect in 2019. The actual dollar increase in liability for total drug costs in 2020 is smaller for Part D plan sponsors ($197) than for Part D enrollees themselves ($377).
Drug manufacturers will be responsible for a larger share of total drug costs up to the catastrophic threshold in 2020 (40%) than in 2019 (36%) because of the 70% discount on the price of brand-name drugs in the coverage gap benefit phase, the amount of which will increase due to the higher out-of-pocket threshold for 2020. The actual dollar increase in total annual covered drug costs will be significantly larger for drug manufacturers ($873) than for Part D plan sponsors ($197).
Under current law, Part D plan liability for drug costs are expected to rise (in dollars) during the coverage gap phase, but their liability for catastrophic coverage could potentially decline. The increase in plan liability during the coverage gap phase is due to the increase in the out-of-pocket spending threshold, which means plans will pay 5% of total drug costs in that phase over a much longer span in 2020 than in 2019. This change, alone would increase premiums to the extent that it increases plan liability. However, the majority of Part D enrollees do not have drug costs high enough to reach the coverage gap phase, and because fewer enrollees are expected to qualify for catastrophic coverage in 2020 (where plans pay 15% of total drug costs), total plan costs could go down, on net, which would result in lower premiums.
How Many Part D Enrollees Could Be Affected By These Changes?
While there are no precise estimates of the number of Part D enrollees who will be affected by the increase in the out-of-pocket threshold for 2020, the increase will directly affect Part D enrollees with very high out-of-pocket drug costs. In 2017 (the most current year of Part D claims data available), 4.9 million non-LIS enrollees reached the coverage gap phase; of that total, 1 million non-LIS enrollees had out-of-pocket drug costs that exceeded the catastrophic threshold (Figure 4). Had the threshold been higher in 2017, fewer than 1 million enrollees would have qualified for catastrophic coverage that year. This means that a larger number of enrollees would have remained in the coverage gap in 2017, where they pay a larger share of their total costs than in the catastrophic phase.
Figure 4: A Small Share of Medicare Part D Enrollees Had High Out-of-Pocket Drug Costs in 2017
Proposed Changes to the Medicare Part D Benefit Design
Lawmakers have introduced several proposals to address concerns about the lack of a hard cap on out-of-pocket spending for Part D enrollees and the significant increase in Medicare spending for catastrophic coverage in recent years, by adding a cap on out-of-pocket drug costs and shifting more of the responsibility for catastrophic coverage costs to Part D plans and drug manufacturers (Figure 5).
Figure 5: Comparison of Proposals to Modify the Allocation of Catastrophic Coverage Costs Under Medicare Part D
In its FY 2020 budget, the Trump Administration proposed establishing an out-of-pocket spending limit in Part D by phasing down beneficiary coinsurance in the catastrophic phase from 5% to 0% over four years, beginning in 2020. The Administration also proposed to increase Part D plans’ share of catastrophic coverage costs from 15% to 80%, and decrease Medicare’s share from 80% to 20%.
In July 2019, the Senate Finance Committee approved legislation that includes a proposal to establish a cap on out-of-pocket drug spending under Part D and reallocate liability for costs above the catastrophic threshold, as part of a larger package of drug price proposals. The cap on beneficiary out-of-pocket spending would be set at $3,100 in 2022. For costs above the catastrophic threshold, the proposal reduces Medicare payments from 80% to 20%, increases plans’ share from 15% to 60%, and requires drug manufacturers to pay 20%, instead of providing discounts in the coverage gap, which would be phased out. The proposed changes to the Medicare benefit design would be phased in over a three-year period, from 2022 to 2024.
In September 2019, Speaker Nancy Pelosi (D-CA) announced legislation that includes a proposal to restructure the Part D benefit, among other provisions. This proposal would establish a hard cap on out-of-pocket spending that would initially be set at $2,000. For costs above the catastrophic threshold, the proposal reduces Medicare payments from 80% to 20%, increases plans’ share from 15% to 50%, and requires drug manufacturers to pay 30%. In addition, the House proposal would also phase out the coverage gap and modify the allocation of costs in the initial coverage phase, by requiring manufacturers to pay 10% of costs. The proposed changes would take effect in 2022.
Conclusion
In the absence of a change in law, Medicare Part D enrollees can expect to face an increase in their out-of-pocket drug costs in 2020. Costs for Part D plan sponsors and drug manufacturers will also increase in dollar terms—but in terms of the share of total drug costs up to the catastrophic threshold, Part D plan sponsors will pay a smaller share in 2020 than in 2019, while manufacturers will pay a larger share. These changes are also likely to affect Part D premiums in 2020 and future years.
Proposed changes to the Part D benefit design would help to mitigate out-of-pocket drug cost increases for Medicare beneficiaries, particularly for those with high drug costs who currently face no limit in their annual out-of-pocket expenses, with Part D plan sponsors and drug manufacturers potentially picking up much of the additional cost.
On October 4, 2019, President Trump released a proclamation suspending entry of immigrants into the United States unless they provide proof of health insurance within 30 days of entry or have financial resources to pay for reasonably foreseeable health insurance costs. The proclamation indicates that the suspension is necessary to protect the health care system and taxpayers from uncompensated care costs. This brief provides an overview of the proclamation and data on health coverage and health care use for immigrants.
Overview of Proclamation
Effective November 3, 2019, the proclamation would suspend entry of immigrants unless they can prove they will be covered by approved health insurance within 30 days of entry into the U.S. or that they have financial resources to pay for reasonably foreseeable medical costs.
Approved health coverage. Under the proclamation, approved health insurance would include employer-sponsored and other private coverage, including unsubsidized coverage through the ACA Marketplaces, short-term plans, traveler plans, or catastrophic plans. Subsidized Marketplace coverage and Medicaid coverage for adults would not count as approved coverage. State or local programs and other programs, like Ryan White, are also not included as approved coverage in the proclamation.
Individuals subject to suspension. The suspension would apply to individuals seeking an immigrant visa on or after November 3, 2019. The new requirement would primarily affect family-based immigrants. It would not apply to refugees, asylees, people entering as non-immigrants, and certain other groups. Children under age 18 are subject to suspension if they are traveling with a parent who is also subject to the suspension.
Individuals subject to the proclamation will need to establish that they meet its requirements to the satisfaction of a consular officer before an immigrant visa is issued. The proclamation indicates that the Secretary of State may establish standards and procedures for these determinations.
An earlier regulation from the Trump administration made changes to public charge policies that will make it harder for immigrants to adjust to lawful permanent resident status or get a green card if they are low-income, sick, or likely to enroll in Medicaid. It is likely that the confusion and chilling effect surrounding the regulation will lead to declines in Medicaid and CHIP coverage among immigrant families beyond those directly affected by the changes and increase the uninsured rate among immigrant families.
Health Coverage and Health Care for Immigrants
In 2017, there were 22 million noncitizens residing in the United States, accounting for about 7% of the total U.S. population.1 About six in ten noncitizens were estimated to be lawfully present immigrants, while the remaining four in ten were estimated to be undocumented immigrants:2 Many individuals live in mixed immigration status families that may include lawfully present immigrants, undocumented immigrants, and/or citizens.
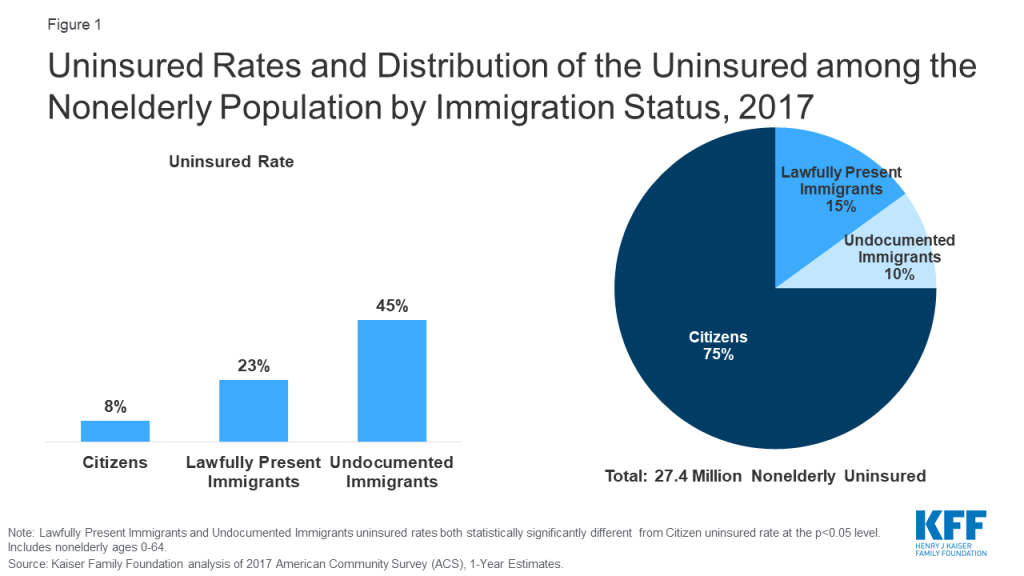
Noncitizens are more likely to be uninsured than citizens, but citizens account for the majority of the total uninsured. Noncitizens, including lawfully present and undocumented immigrants, are significantly more likely to be uninsured than citizens, reflecting limited eligibility for coverage options and enrollment barriers. As of 2017, among the total nonelderly population, 23% of estimated lawfully present immigrants and more than four in ten (45%) estimated undocumented immigrants were uninsured compared to fewer than one in ten (8%) citizens (Figure 1). Despite the higher uninsured rate among noncitizens, citizens still accounted for three-quarters of the total 27.4 million uninsured.
Figure 1: Uninsured Rates and Distribution of the Uninsured among the Nonelderly Population by Immigration Status, 2017
The higher uninsured rates among noncitizens reflect limited access to employer-sponsored coverage; eligibility restrictions for Medicaid, CHIP, and ACA Marketplace coverage; and barriers to enrollment among eligible individuals.
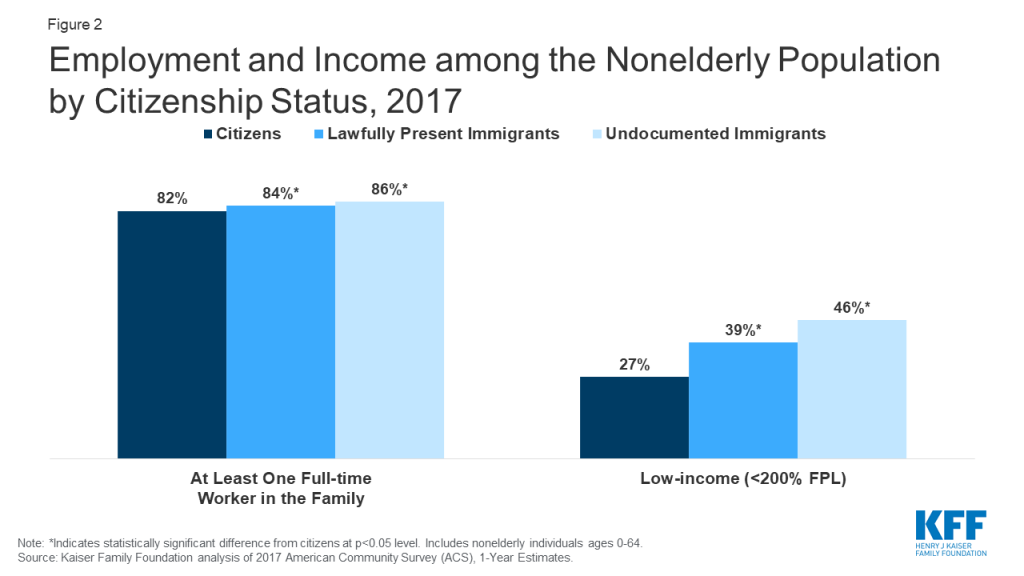
Although most nonelderly noncitizens live in a family with a full-time worker, they face gaps in access to private coverage. Nonelderly noncitizens are more likely than nonelderly citizens to live in a family with at least one full-time worker, but they also are more likely to be low-income (Figure 2). They have lower incomes because they are often employed in low-wage jobs, and they work in industries that are less likely to offer employer-sponsored coverage. Further, given their lower incomes, noncitizens face increased challenges affording employer-sponsored coverage when it is available or purchasing coverage through the individual market.
Figure 2: Employment and Income among the Nonelderly Population by Citizenship Status, 2017
Lawfully present immigrants may qualify for Medicaid and CHIP but are subject to certain eligibility restrictions. In general, lawfully present immigrants must have a “qualified” immigration status to be eligible for Medicaid or CHIP and many, including most LPRs or “green card” holders, must wait five years after obtaining qualified status before they may enroll. States have an option to eliminate the five-year wait for lawfully residing immigrant children and pregnant women, and half of states (24) apply the option to both children and pregnant women, while ten states use it for children only, and one state (Wyoming) uses it only for pregnant women.3 Lawfully present immigrants can purchase coverage through the ACA Marketplaces and may receive subsidies for this coverage within the five-year waiting period. Undocumented immigrants are not eligible to enroll in Medicaid or CHIP or to purchase coverage through the ACA Marketplaces.
Many lawfully present immigrants who are eligible for coverage remain uninsured because immigrant families face a range of enrollment barriers, including fear, confusion about eligibility policies, difficulty navigating the enrollment process, and language and literacy challenges.
Research shows immigrants tend to be younger and healthier and to use less health care than U.S born individuals. Data show that immigrants spend less on health care, compared to their U.S. born counterparts, and make larger out-of-pocket health care payments compared to nonimmigrants.4 Immigrants have lower spending, in part, because they use less care due to their low coverage rates and limited access to care.5 They also tend to be younger and healthier than nonimmigrants, although this health difference decreases over time as immigrants spend longer in the United States.6
Though uninsured people are less likely to access care than those with coverage, when they do seek care they are typically billed for these services. Most uninsured people do not receive health services for free or at reduced charge, and many are asked to pay in full up front before they receive care.7 As a result, when uninsured people use care, they are at risk of incurring medical debt. Like other uninsured individuals, many immigrants without coverage can obtain low-cost care through community health centers. Moreover, under federal law, hospitals are required to screen and stabilize every patient who seeks emergency care.
Some of the cost of care for uninsured people is converted to uncompensated care for providers, but uncompensated care costs have declined in recent years and immigrants likely account for a small share of uncompensated care costs. When uninsured people are unable to pay their bills, providers absorb some of the cost of care for the uninsured. Some uncompensated care is offset by private or public programs specifically for this purpose. In recent years, uncompensated care costs have declined due to coverage expansions under the Affordable Care Act (ACA).8 Further, there is limited evidence that uncompensated care for uninsured patients is associated with hospitals charging higher prices for those who are privately insured.9 Given that immigrants account for a small share of the total uninsured population and that they use less care compared to the U.S. born, they likely account for a small share of total uncompensated care costs.
Kaiser Family Foundation analysis of 2017 American Community Survey (ACS), 1-Year Estimates. ↩︎
The estimate of the total number of non-citizens in the US is based on the 2017 American Community Survey (ACS). The ACS does not include a direct measure of whether a non-citizen has legal status or not. We impute documentation status by drawing on methods underlying the 2013 analysis by the State Health Access Data Assistance Center (SHADAC) and the recommendations made by Van Hook et. al.. This approach uses the second wave of the 2008 Survey of Income and Program Participation (SIPP) to develop a model that predicts immigration status for each person in the sample; it then applies the model to a second data source, controlling to state-level estimates of total undocumented population as well as the undocumented population in the labor force from the Pew Research Center. See, “U.S. Unauthorized Immigrant Total Dips to Lowest Level in Decade,” available here: http://www.pewhispanic.org/2018/11/27/u-s-unauthorized-immigrant-total-dips-to-lowest-level-in-a-decade/. ↩︎
Lila Flavin, Leah Zallman, Danny McCormick, and J. Wesley Boyd, Medical Expenditures on and by Immigrant Populations in the United States: A Systematic Review, (Boston, MA: Tufts University School of Medicine, 2018), https://doi.org/10.1177%2F0020731418791963↩︎
Almost Half of Non-Elderly Families have At Least One Adult with a Pre-Existing Condition
An updated KFF analysis estimates that almost 54 million people – or 27% of all adults under 65 —have pre-existing health conditions that would likely have made them uninsurable in the individual markets that existed in most states before the Affordable Care Act.
The share of adults under 65 with such declinable pre-existing conditions varies significantly across states, from at least a third in West Virginia (37%), Arkansas (34%), Kentucky (34%), and Mississippi (34%) to a little more than one in five in Colorado (22%).
Older working-age Americans (ages 55-64) are the most likely age group to have declinable pre-existing conditions (44%), more than twice the share (18%) among the youngest age group (18-34). Women are more likely than men to have declinable conditions (30% compared to 24%).
Almost half (45%) of non-elderly families include at least one adult with a medical condition who might not be able to buy individual insurance without the ACA’s prohibition of medical underwriting.
The analysis comes as the Fifth Circuit Court of Appeals weighs a decision in the Texas v. Azar case, which seeks to overturn the entire Affordable Care Act, including the provisions that prohibit insurers from denying coverage or charging more to people with pre-existing conditions. The Trump administration has joined the conservative state Attorneys General in arguing that the ACA should be invalidated.
While most people with pre-existing conditions are covered now through employers or public programs such as Medicaid, people may look to the individual market for coverage during periods of transition, such as losing or changing a job, leaving a job due to illness, starting a business, aging off a parent’s policy, retiring before age 65, or losing Medicaid eligibility.
Before the ACA protections took effect in 2014, private insurers in the individual market could use applicants’ health status, history and other risk factors to determine whether and under what terms to issue coverage. Some conditions that could lead to automatic denials of coverage at the time include cancer, diabetes, epilepsy, heart disease, and pregnancy.
Using 2018 data from two large government surveys, the analysis estimates the total number of nonelderly adults in each state with a health condition that could lead to a denial of coverage in the individual insurance market, based on pre-ACA field underwriting guides for brokers and agents. The estimates do not include people with other health conditions that would not necessarily cause a denial, but could lead to higher insurance costs based on underwriting.
Whether and how people with pre-existing conditions could be affected if they seek coverage on the individual market in the future depends on the outcome of the ongoing court challenge, and how federal and state lawmakers respond to the court’s decision.