A Look at the Latest Suicide Data and Change Over the Last Decade
Note: This data note was updated on Aug. 4, 2023, to correct a data error in Figure 4.
From 2011 to 2022, over half a million lives (539,810) were lost to suicide, with 2022 showing the highest number of deaths on record. Within this period, the adjusted suicide rate increased by 16%. Recognizing the mounting mental health crisis and demand for accessible crisis care, the federal government introduced a new crisis number, 988, available nationwide in July 2022. This easy to remember three-digit number connects callers who are suicidal or experiencing a mental health emergency to a crisis counselor at one of 200+ local crisis call centers. There, they may access crisis counseling, resources, referrals, and connections to other crisis services. Though suicide deaths slowed in 2019 and 2020, they began to increase again in 2021 and 2022, but the cause of this recent rise in suicides is unclear.
Key takeaways from an analysis of aggregate provisional data from 2022 and CDC WONDER data from 2011 to 2021, which represents the most recent and comprehensive data available before the mid-2022 launch of 988, include the following:
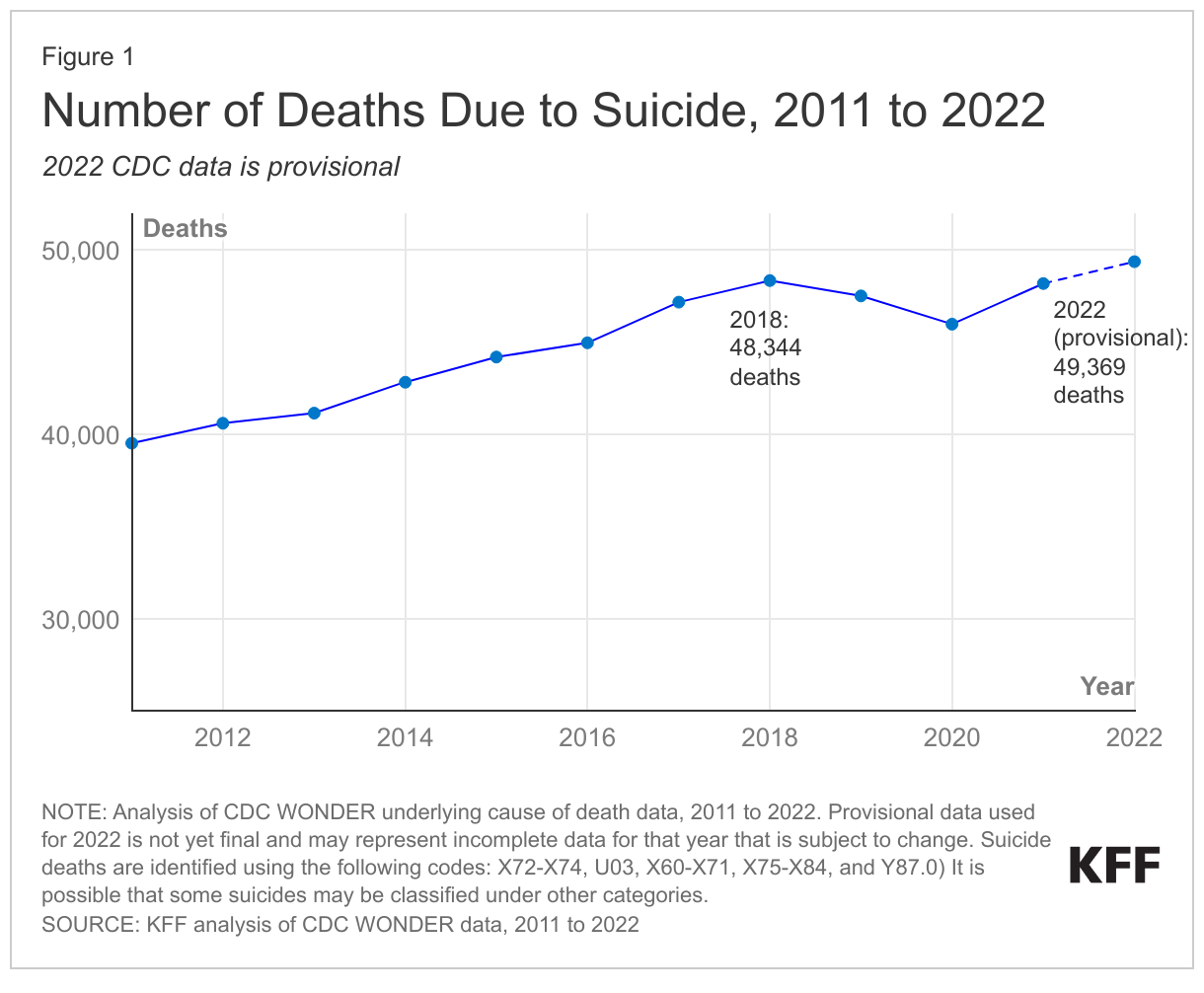
- CDC’s provisional data for 2022 show a record high of 49,369 suicide deaths, coming after modest declines in 2019 and 2020.
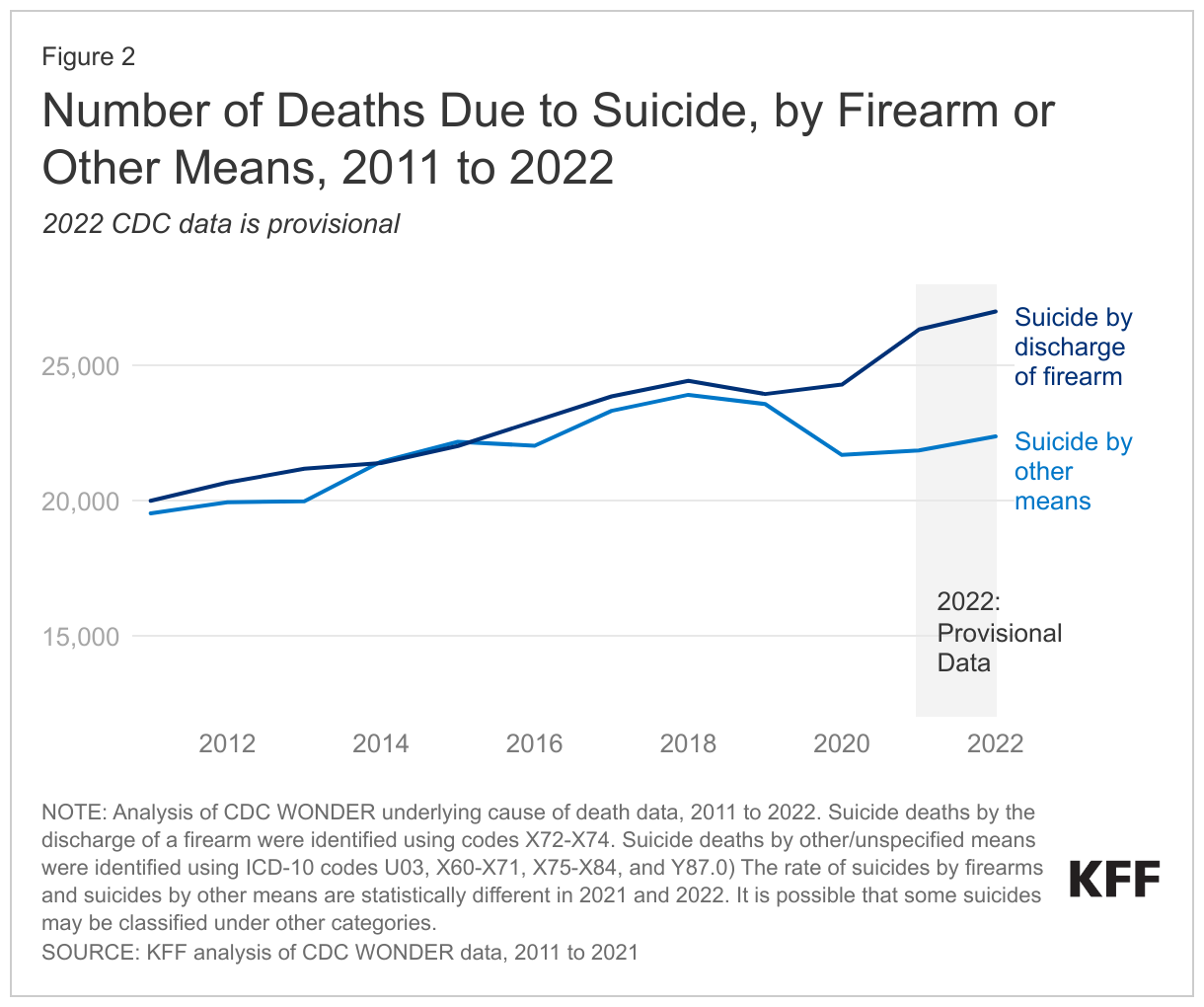
- In 2022, provisional data indicates the highest number of gun-related suicides on record; increases in firearm suicides are driving the increases in overall suicide deaths in recent years.
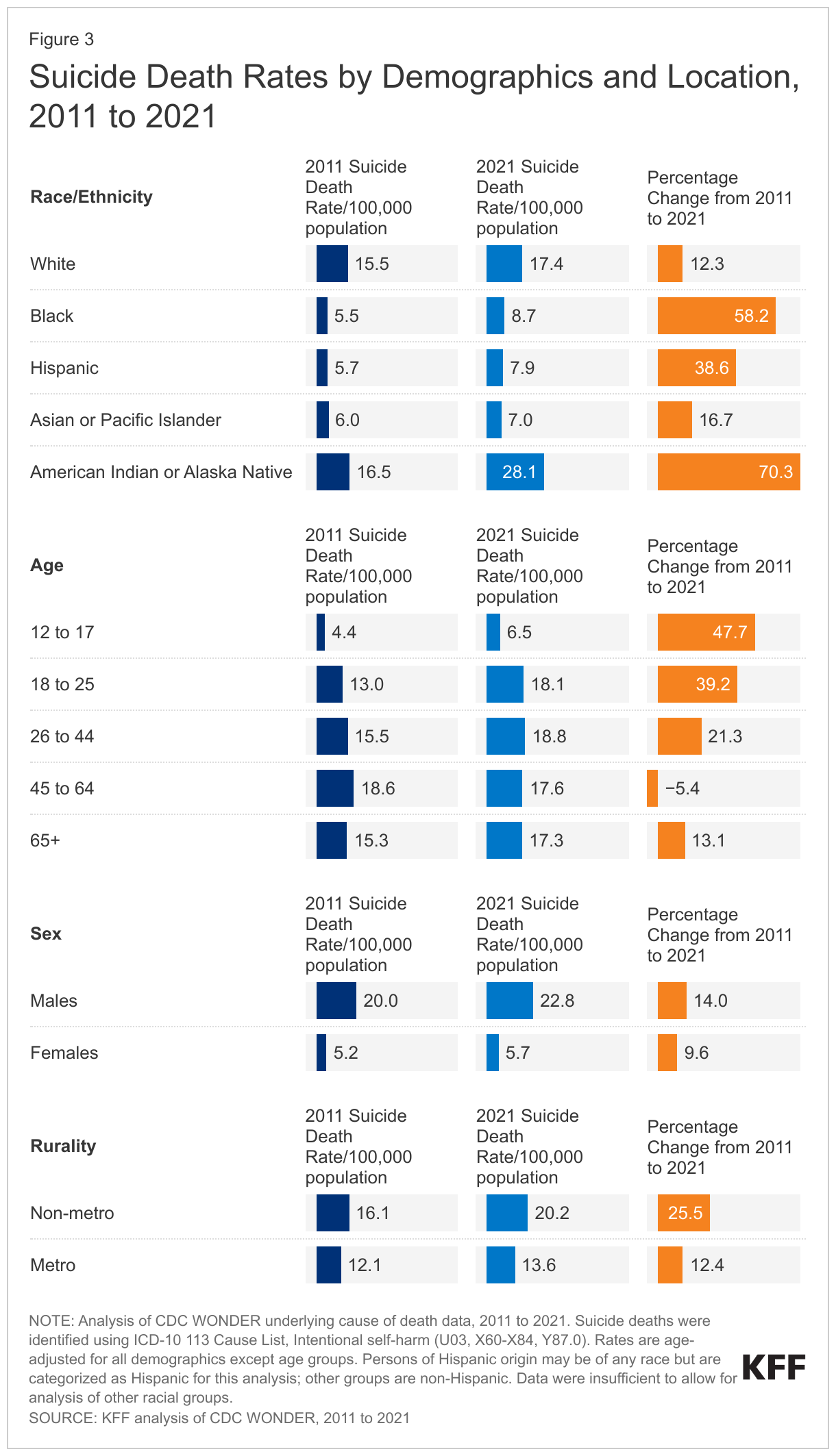
- Suicide death rates in 2021 were highest among American Indian and Alaska Native people, males, and people who live in rural areas.
- Suicide deaths are increasing fastest among people of color, younger people, and those who live in rural areas with many groups seeing increases of 30% or more from 2011 to 2021.
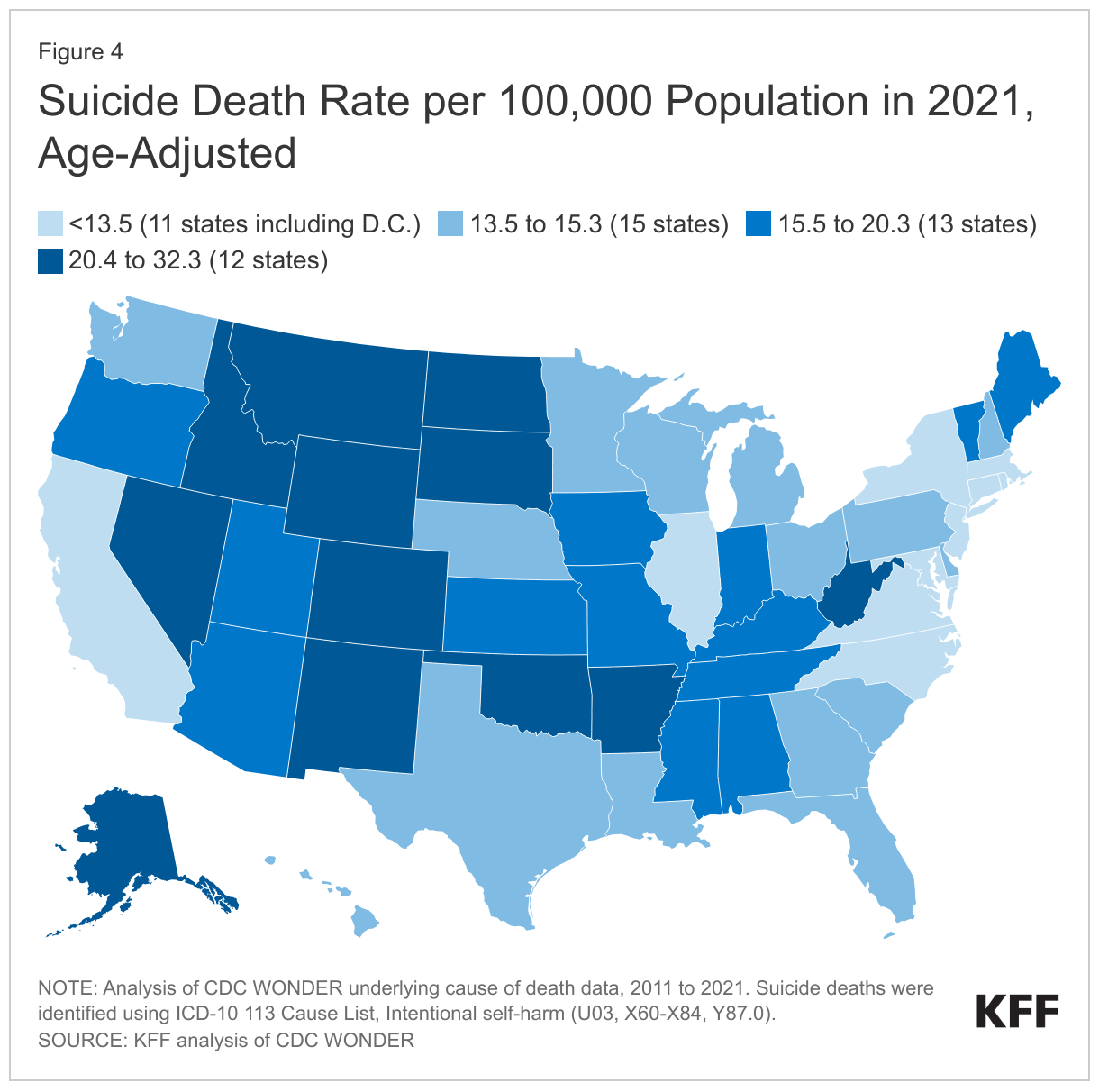
- Suicide death rates varied considerably by state in 2021, as did the rate of change between 2011 and 2021.
Provisional CDC data show that the number of suicide deaths in 2022 is the highest recorded, exceeding the next closest year (2018) by over 1,000 deaths (Figure 1). When adjusted for population growth and age, the suicide rate has risen by 16% from 2011 to 2022, moving from 12.3 to 14.4 deaths per 100,000 individuals. Looking back further to 1999, there is a substantial 37% increase from a rate of 10.57 per 100,000. Notably, while 2022 had the highest recorded number of suicide deaths, its rate is similar to 2018 (14.5 in 2022 vs. 14.2 in 2018 per 100,000) but higher than the rate in 2020—the year before suicide deaths began to climb again. Increases in the number of suicide deaths follow high levels of mental health symptoms during COVID, rising financial stressors, and longstanding difficulty accessing needed mental health care—particularly for some populations. Total suicide numbers may be undercounted, as some research suggests that suicides may be misclassified as drug overdose deaths since it can be difficult to determine whether drug overdoses are intentional.
Provisional data from 2022 show the highest number of firearm-related suicides on record, driving the overall increases in suicide deaths to record levels. Firearm-related suicides have been increasing in recent years. In 2021, firearm-related suicides increased by 8% from 2020 and went up another 3% in 2022, while deaths from other suicide methods remained more stable (Figure 2). Firearm-related suicides are now the most common method of suicide, accounting for 55% of all suicide fatalities in both 2021 and 2022. The availability of guns (measured indirectly by the number of gun laws in a state) is linked to firearm suicide rates – with states with fewer gun laws having higher rates. Suicide deaths accounted for more than half (55%) of all deaths involving a firearm in 2021.
Suicide death rates in 2021 were highest among American Indian and Alaska Native (AIAN) people, males, and people who live in rural areas. As of 2021, AIAN people had the highest suicide death rate at 28.1 per 100,000 people, one and a half times higher than the rate for White people (17.4 per 100,000 people). Suicide death rates for Black, Hispanic, and Asian and Pacific Islander people were at least half the rate of White people. Females are more likely to report mental illness and are more likely to attempt suicide, but male suicide death rates are four times higher (22.8 versus 5.7 per 100,000). Non-metropolitan areas have a higher suicide rate (20.2 per 100,000) than metro areas (13.6 per 100,000). There are similar suicide rates across adult age groups in 2021 (Figure 3). Because younger people are less likely to die of other causes, suicides are the second leading cause of death in adults under the age of 45, accounting for 16% of deaths in people 18-25 and 9% of deaths in people 26-44 in 2020.
Suicide deaths are increasing fastest among people of color, younger individuals, and people who live in rural areas. Between 2011 and 2021, suicide death rates increased substantially among people of color, with the highest increase among AIAN people (70% increase, from 16.5 to 28.1 per 100,000), followed by Black (58% increase, from 5.5 to 8.7 per 100,000), and Hispanic (39% increase, 5.7 to 7.9 per 100,000) people (Figure 3). Other studies show a particularly large increase in suicide deaths among Black youth and adolescents. Underdiagnosis of mental health conditions, structural barriers to care, stereotypes and discrimination associated with poor mental health, racism and discrimination, and disparities in the use of mental health services may all contribute to rising suicide rates among people of color. Among adolescents, emergency department visits for suicide attempts have increased in recent years, primarily driven by females. And a KFF/CNN survey found that roughly half of parents said the pandemic had a negative impact on their child’s mental health, including 17% who said it had a “major negative impact.” In rural areas, suicide death rates increased significantly, possibly due to acute shortages of mental health workers in these areas. The suicide death rate also increased in adolescents (48% increase, from 4.4 to 6.5 per 100,000) and young adults (39% increase, from 13.0 to 18.1 per 100,000) between 2011 and 2021 (Figure 3).
Suicide death rates varied substantially by state in 2021, as did the rate of change from 2011 to 2021. Suicide death rates by state range from a low of 6.21 per 100,000 population in Washington, D.C. to a high of 32.34 in Wyoming, with a median death rate of 15.3 per 100,000 in 2021 (Figure 4). The suicide rate may vary by state due to factors such as demographics, firearm availability (involved in over half of suicides), mental health status, and access to mental health services. Between 2011 and 2021, suicide death rates increased by 25% or more in 12 states, with the largest increases in Alaska (54% increase, from 20.0 to 30.8 per 100,000), South Dakota (48% increase, from 15.7 to 23.4 per 100,000), Nebraska (43% increase, from 10.5 to 15.0 per 100,000), and Montana (42% increase, from 22.5 to 32.0 per 100,000).
While the exact cause for the rise in suicides in recent years is unknown, it may reflect, in part, increasing stressors and longstanding unmet mental health needs—challenges that coincide with 988’s launch. In its first year, 988 improved answer rates and reduced wait times while handling nearly 5 million contacts due to surging demand; however, its influence on overall suicide rates, particularly among people of color or other vulnerable populations, is yet to be seen. Since its introduction in July 2022, 988 has received almost 5 million contacts, including almost 1 million from the Veteran’s Crisis Line. While early nationwide metrics look positive, disparities in state performance and questions about long-term funding for state call centers and crisis infrastructure persist. Current publicly available data on 988 gives only a partial view of its implementation and possible access challenges. Analysis of more comprehensive 988 metrics, coupled with future data on suicide attempts and deaths may help shed light on the impact of 988 and related crisis services in addressing escalating suicide deaths.
If you or someone you know is considering suicide, contact the 988 Suicide & Crisis Lifeline at 988.
This work was supported in part by Well Being Trust. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.