States’ Management of Medicaid Home Care Spending Ahead of H.R. 1 Effects
State Findings
Over one-third of Medicaid spending pays for long-term care, with most of the spending paying for home care—also known as “home- and community-based services” or HCBS. Medicaid pays for almost 70% of all home care spending in the U.S., nearly all of which is provided through optional services. Among those optional services, states rely heavily on Medicaid “waivers” to provide home care, which allow them to manage costs using mechanisms such as capping spending or enrollment in the waiver (Box 1). States may also use waiting lists to track and manage people who want to receive but are not yet receiving home care. While waiting lists may result from caps on waiver spending or enrollment, states also used them for other administrative reasons (Box 2).
Medicaid’s significant spending on home care and the availability of mechanisms for limiting such spending could spur states to cut home care spending in response to the 2025 reconciliation law. Cutting spending on home care could result in either fewer people receiving any benefits or people receiving fewer covered services, even though the need for home care is unlikely to fall in future years. The recently passed reconciliation law is estimated to reduce federal Medicaid spending by $911 billion between 2025 and 2034, roughly a 14% reduction in federal funding for the program. During the last major reduction in federal Medicaid spending, all states reduced spending on home care by serving fewer people (40 states) or by cutting benefits or payment rates for long-term care providers (47 states).
Using data from the 23rd KFF survey of officials administering Medicaid home care programs, this issue brief describes the mechanisms states are currently using to limit Medicaid spending on home care and their plans for adopting new mechanisms in state fiscal year (FY) 2026. The survey was sent to all home care programs in all 50 states and the District of Columbia (hereafter referred to as a state), which states completed between April and July 2025. All states except Florida completed the survey, although response rates for specific questions may have been lower. States generally completed the survey prior to enactment of the reconciliation law, so changes to limit spending in FY 2026 are not attributable to the new law. Survey findings are reported by state and waiver target population, although states often offer multiple waivers for a given target population. Key takeaways include:
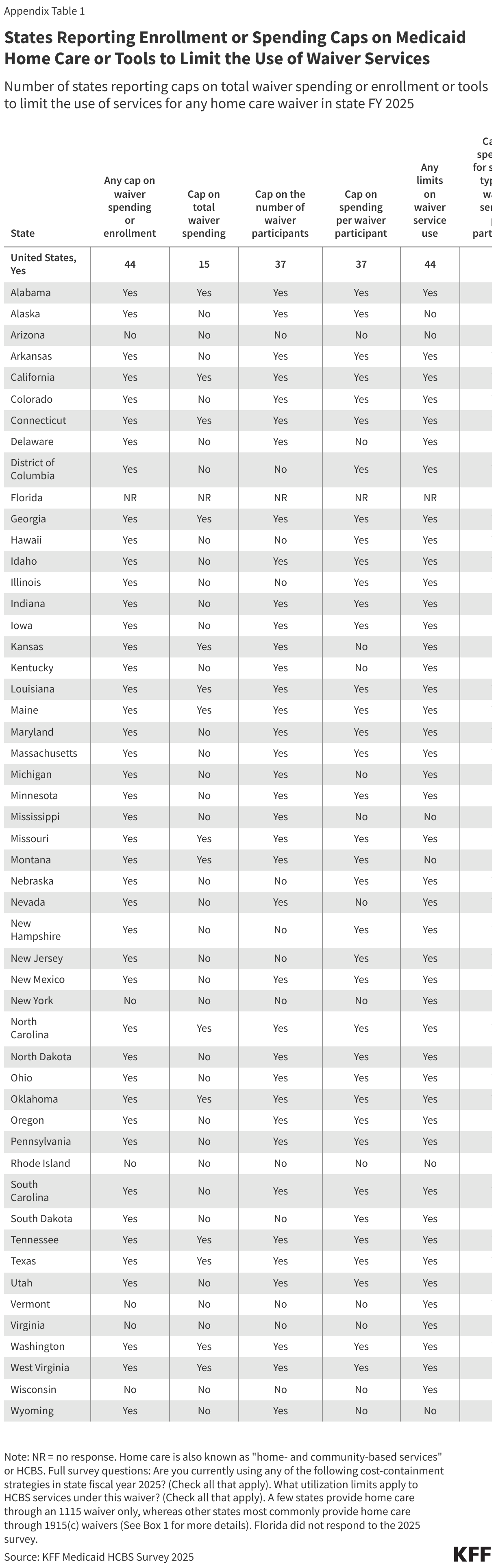
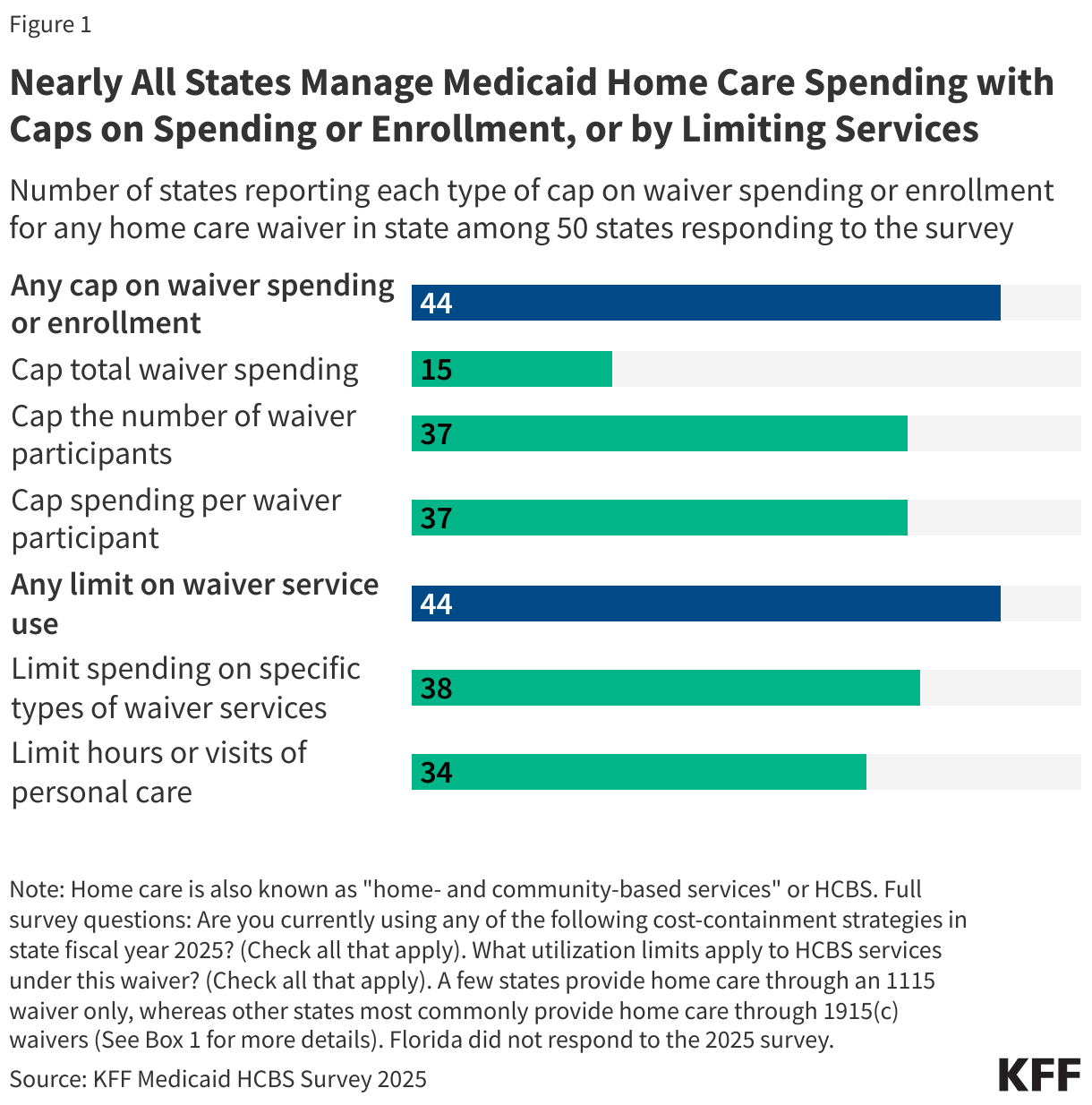
- For most home care services, which are delivered through waiver programs, 44 out of the 50 responding states constrain spending through limits on either total enrollment (37 states) or on total spending (15 states, Figure 1). Most states (37) also cap waiver spending per participant for at least one waiver.
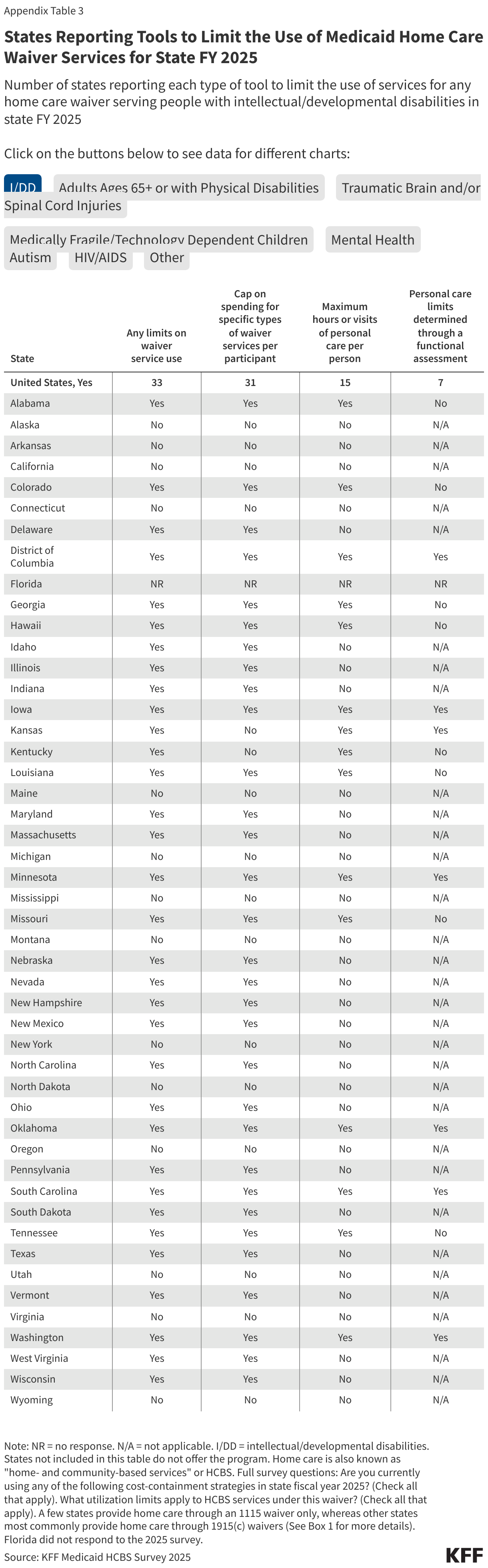
- Most states (44) reported using mechanisms in at least one waiver to restrain spending that applies to specific services, such as limiting the amount of spending for services per participant (38 states) or limiting the quantity of personal care enrollees may receive (34 states).
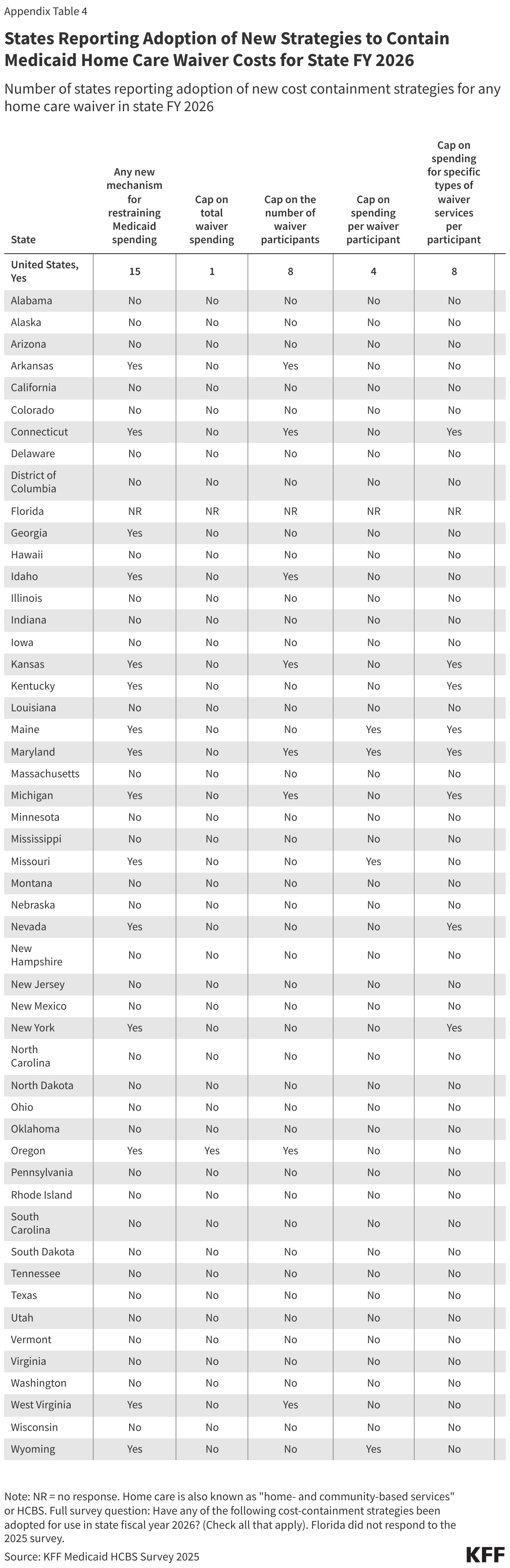
- Nearly a third of responding states (15) reported planning to adopt new strategies in FY 2026 to contain home care costs. Since most survey responses were collected before enactment of the reconciliation bill, it is not yet known how this number will change as states prepare for the forthcoming cuts to federal Medicaid spending.
- Fewer mechanisms are available to states in managing spending for home care services provided outside of waivers, but nearly all states use prior authorization as a tool to manage that type of spending.
Box 1: Legal Requirements and Options for Medicaid Home Care Waivers
Most Medicaid home care is provided through 1915(c) waivers, which allow states to provide home care to people who prefer to receive long-term care in their home or community rather than from an institution. The 1915(c) waiver allows states to waive several requirements of Medicaid law including that services be available statewide, and on a comparable basis to all Medicaid enrollees. States may offer a variety of unlimited services through the waiver, and states tailor the benefit packages to meet the needs of a particular target group. All services must follow an individualized plan of care. Among other requirements, 1915(c) waivers must demonstrate that the services will not cost more than institutional care would. This requirement is implemented through a cost neutrality test [see Instructions, Technical Guide and Review Criteria V3.7], that compares the per person costs of waiver services to the per person costs of providing care to similar people in an institutional setting.
States are permitted, but not required, to set limits on total enrollment or spending in a 1915(c) waiver. Enrollment limits may take several forms including the number of participants served, the number of enrollees at a given time, or the rate at which people are enrolled or disenrolled. States may also keep waiver slots available as “reserve capacity” for people to enroll on a priority basis, such as people transitioning from institutions to the community or people in crisis.
Four states also only provide home care through 1115 waivers, which offer states an avenue to test new approaches in Medicaid that differ from what is required from federal statute, if the approach is likely to “promote the objectives of the Medicaid program” in the view of the Secretary of Health and Human Services. There is no statutory requirement for waivers to be “budget neutral,” but long-standing policy and practice has required states to demonstrate budget neutrality. One way to demonstrate budget neutrality is to show that per enrollee spending over the course of the waiver does not exceed projected per enrollee spending in the absence of the waiver.
Mechanisms for Limiting Waiver Home Care Spending and Enrollment
Most states (37) manage Medicaid spending on home care by capping either total enrollment, or both total spending and enrollment (Figure 1). Most states also cap per person spending for home care waiver services. The two primary types of waivers states use to offer Medicaid home care are 1915(c) and 1115. The two waivers differ in that 1915(c) waivers are specifically used to provide Medicaid home care to people who require an institutional level of care whereas 1115 waivers can test all types of new Medicaid approaches (Box 1). Among the 50 responding states that provide home care through waivers, 15 states have caps on total waiver spending, 37 have caps on the total number of participants, and 37 have caps on spending per person (Appendix Table 1).
Box 2: Differences Between Waiver Caps and Waiting Lists
Although caps on total spending or participants may result in waiting lists when the caps result in too few waiver slots relative to the number of people who wish to receive services, in many cases, waiting lists and enrollment caps are conceptually different. In nearly all states, there are waivers that use spending or enrollment caps but don’t have waiting lists or waivers that have waiting lists without spending or enrollment caps.
States may constrain waiver spending by capping total enrollment or total spending but not have a waiting list for that waiver in the following types of situations:
- The caps are set high enough that no people who wish to receive services are unable to do so,
- The state allows all applicants to enroll in the waiver but limits spending by reducing the services provided, or
- The state allocates services to people with the greatest need and refers people who are not approved for waiver services to other home care programs.
States may have waiting lists in the absence of caps on enrollment or total spending in the following types of situations:
- People have registered to receive home care, but the state has not yet determined whether they are eligible,
- People are determined eligible for waiver services, but they have not yet had their level of care assessed or started receiving services, or
- People are eligible for services but not receiving them on account of provider shortages.
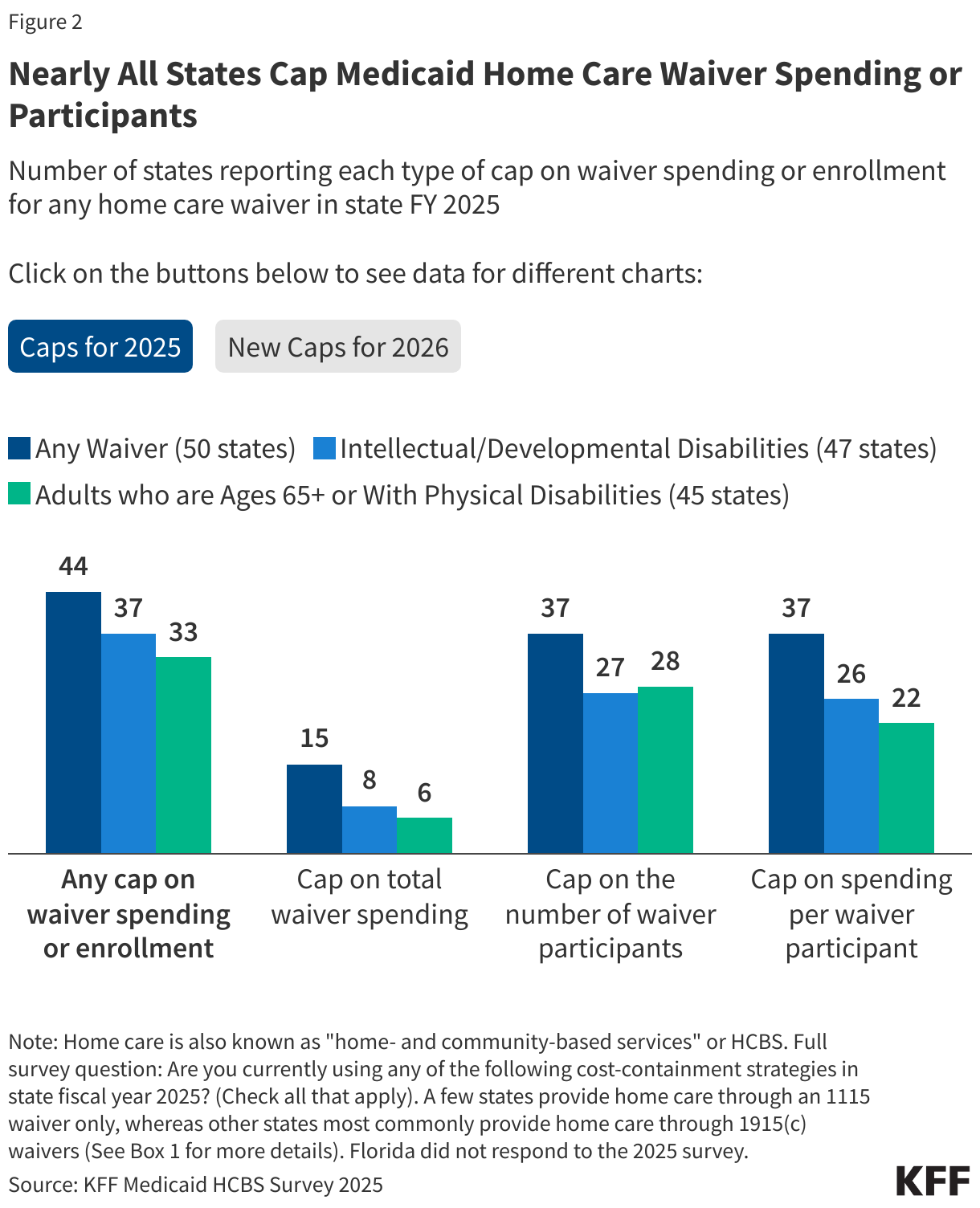
Use of caps on total spending, participation, or costs per participant were reported in 44 states (Figure 2). Among the 50 responding states with waivers, 44 had caps of some sort, including 15 with caps on total spending, 37 with caps on total participants and 37 with caps on spending per participant. For both 1915(c) and 1115 waivers, states are required to meet cost neutrality requirements to demonstrate that the costs per enrollee in waiver services do not exceed the per enrollee costs of institutional care (Box 1). States may meet this requirement by showing that average costs per enrollee are below the average costs of institutional care or they may establish cost limits for all participants enrolled in the waiver. States that adopt such individual cost limits [see Instructions, Technical Guide and Review Criteria V3.7] must specify the safeguards in place to address people’s needs after they have reached the individual cost limit.
Use of caps is similar for waivers that serve different target populations. Among waivers for people with intellectual or developmental disabilities (47 states) or people who are ages 65 and older or have physical disabilities (45 states), the number of states with caps on total spending (8 and 6 respectively), participation (27 and 28), and spending per participant (26 and 22) are similar. Similar trends also apply for waivers that are available in a smaller number of states (Appendix Table 2).
Less than a quarter of states (11) reported planning to adopt new mechanisms to limit waiver enrollment or spending in state FY 2026. Among states that are planning to adopt new mechanisms, caps on the number of waiver participants are most common (8 states) with few states planning to newly cap spending per waiver participant (4) or total waiver spending (1). Only two states, Maryland and Oregon, reported planning to adopt more than one mechanism (Appendix Table 4).
Mechanisms for Limiting the Costs of Specific Waiver Home Care Services
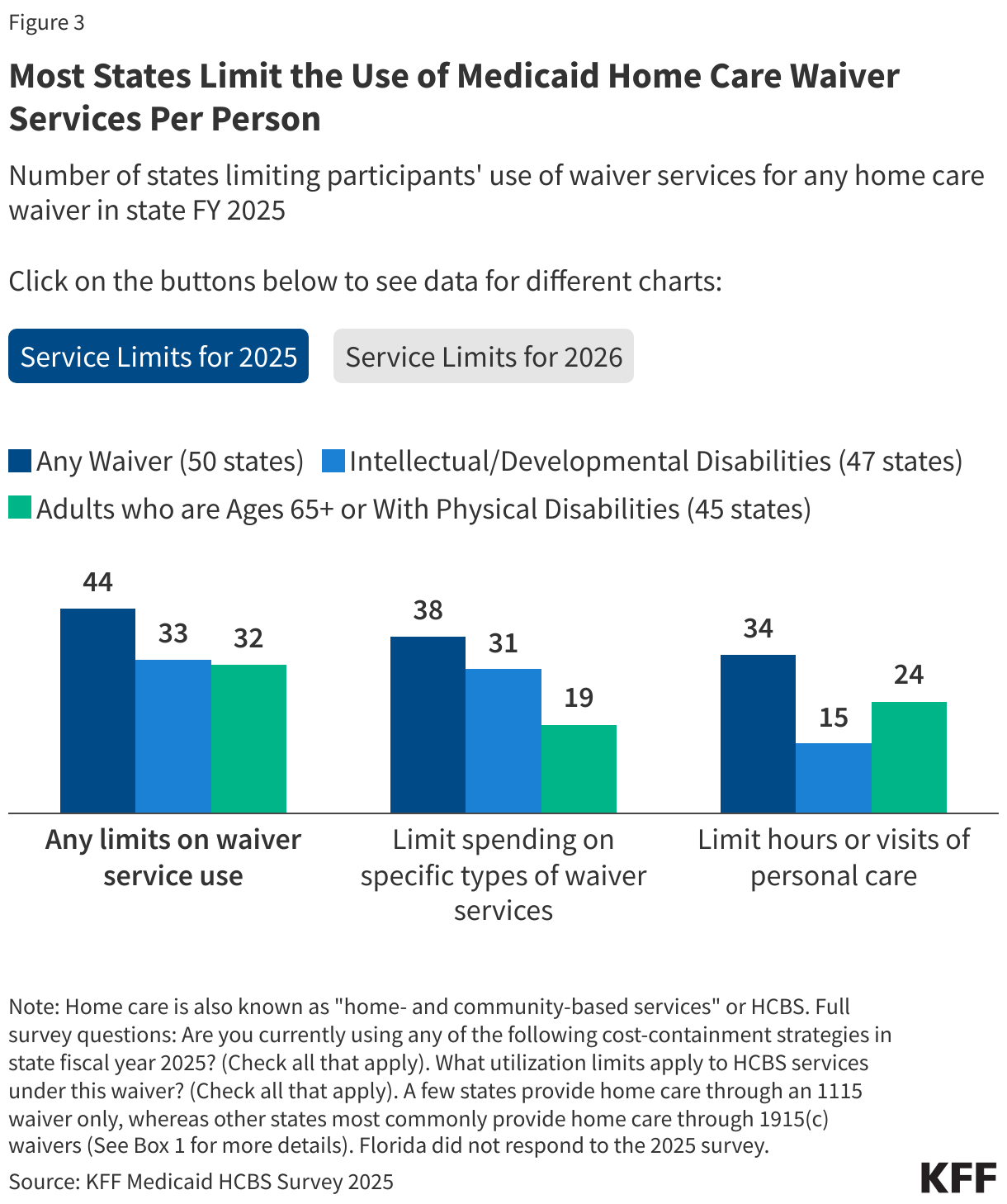
Most states (44) use at least one mechanism to constrain the costs of specific home care services per participant in their waivers (Figure 3). Among states with service-specific limits, caps on spending for specific services (38 states) are more common than volume-based limits such as maximum hours of personal care or number of visits (used by 34 states).
States are more likely to use spending caps for waivers that serve people with intellectual and developmental disabilities but are more likely to use volume-based limits for waivers that serve older adults and people with physical disabilities. Of the 47 states offering 1915(c) waivers serving people with intellectual and developmental disabilities, close to two-thirds of states (31) cap spending for waiver services per participant and nearly a third limit personal care hours or visits per person (15 states). For the 45 states with waivers serving people who are ages 65 and older or have physical disabilities, limits on the quantity of personal care are more common (24 states) than caps on spending for waiver services per participant (19 states). The number of states with these service caps varies for less common waivers. The maximum number of hours or visits of personal care vary by state and over a third of states determine limits through a functional assessment (19 states).
States reported capping spending on a range of different waiver services, including home and vehicle accessibility modifications and adaptive equipment and assistive technology. Home and vehicle accessibility modification limits, such as ramps and wheelchair van lifts, vary across states; Delaware and Nebraska have waivers serving people with intellectual and developmental disabilities that cap adaptations to $10,000 per participant every five years while Massachusetts waivers for the same population limit home modifications to $50,000 and vehicle modifications to $25,000 per participant in a five-year period. Some states, like Illinois, group all equipment, technology, and modifications into a combined category for spending limitations, but other states have separate caps. For example, Louisiana’s waiver serving people with intellectual and developmental disabilities caps spending on specialized medical equipment at $2,500 per year and Michigan’s waiver for people who are ages 65 and older or have physical disabilities caps spending on assistive technology at $5,000 per year.
For FY 2026, 12 states reported planning to adopt new waiver service limits to constrain costs. New caps on spending for specific types of waiver services per participant (8 states) are more common than limits on the quantity of personal care (5 states). Connecticut is the only state that reported planning to adopt both mechanisms (Appendix Table 4).
Use of Prior Authorization to Manage Spending on State Plan Home Care
For Medicaid home care that is provided through the state plan, states cannot use waiver-specific mechanisms for constraining costs but do generally use prior authorization. State Medicaid agencies often require enrollees to obtain approval of certain health care services or medications before the care is provided—an insurance practice commonly referred to as “prior authorization.” In Medicaid, prior authorization is used for both mandatory services, such as home health, and optional services, such as personal care, and is widely used by Medicaid managed care organizations. If the requested service is deemed not appropriate or medically necessary, the request may be denied (fully or partially), but enrollees may be able to appeal the decision through certain appeals and exemption procedures. However, the appeals process can be difficult to navigate, and individuals may be denied access to needed care while waiting for a decision. In a KFF survey conducted in July 2025, 79% of Medicaid enrollees under age 65 and 67% of those ages 65 and older found delays and denials of health care services by health insurance companies to be a major problem.
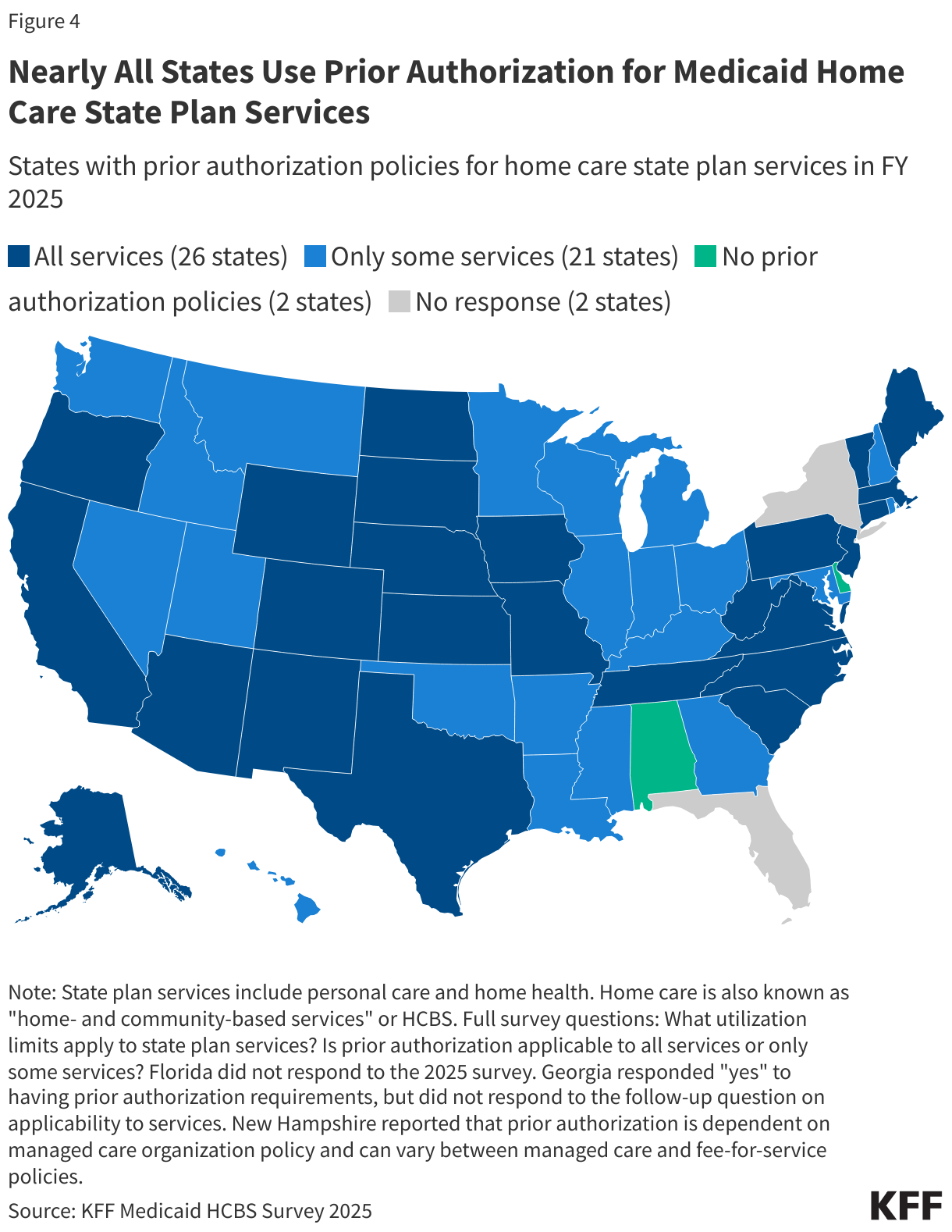
Nearly all states (47) reported using prior authorization to constrain costs on either personal care or home health services (Figure 4). Among those states, over half (26) use prior authorization for all home care services, while the remaining states (21) have this policy in place for only some services. Home health is a mandatory benefit for all states, and 40 states use prior authorization for home health. Personal care is an optional benefit offered by 33 states, and nearly all (29) use prior authorization for personal care. Common services that require prior authorization include personal care, private duty nursing, specialized equipment and technology, and home and vehicle modifications. Prior authorization is also used for home care service requests above certain thresholds (e.g. more than 40 hours per week of personal care).
States reported that prior authorization for Medicaid home care services may be conducted by various entities, including Medicaid agencies, other state entities, managed care organizations, or case managers. Across state plan services, the most common entities responsible for approving or denying services are managed care organizations (12 states), utilization management vendors (7 states), state Medicaid agencies (6 states), or other state agencies (6 states). The same entities are typically responsible for conducting prior authorization for waiver services.
States may also use prior authorization for waiver services, but it may be part of person-centered service planning requirements that apply to all 1915(c) waivers [see Instructions, Technical Guide and Review Criteria V3.7]. All services provided through a 1915(c) waiver must be specified in advance through a written service plan, also known as a plan of care. The plan is intended to provide a complete picture of how enrollees’ needs are met. The plan documents which specific waiver services will be provided to participants, including the amount, duration, and frequency of each service, and the types of providers that may furnish each service.
KFF asked states about whether they required cost sharing for home care and found that few do. Only 3 states reported requiring cost sharing for personal care offered through waivers (Georgia, Illinois, and Rhode Island) and 3 states reported requiring copayments for other waiver services (Minnesota, Oklahoma, and Rhode Island). Additionally, 3 states (Georgia, Idaho, and Maine) reported requiring copayments for home health services. No states reported adopting new copayments for state FY 2026. Starting October 1, 2028, the reconciliation law requires states to impose cost sharing of up to $35 per service on adults eligible for Medicaid through the Affordable Care Act Medicaid expansion with incomes 100-135% FPL. Nearly 400,000 Medicaid enrollees who use long-term care are eligible on account of the Medicaid expansion, and that group will be required to pay cost sharing under this requirement. It is unknown whether states will choose to apply the cost sharing requirements for home care more broadly—either on account of administrative efficiencies or as a mechanism to reduce state spending on home care in response to the historic reduction in federal Medicaid funding from the reconciliation law.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Appendix Tables