Medicaid Managed Care Reporting and Transparency: Managed Care Program Annual Reports
Introduction
Comprehensive, capitated managed care is the dominant Medicaid delivery system, accounting for about 78% of beneficiaries (over 66 million individuals as of July 2024) and 50% of total Medicaid spending (over $458 billion in FY 2024). States were contracting with over 290 individual Medicaid managed care organizations (MCOs) (as of July 2024), which represent a mix of private for-profit, private non-profit, and government plans. Medicaid managed care contracts are among the largest and most complex state contracts, frequently exceeding billions of dollars a year. While the majority of states contract with managed care plans, states decide which populations and services to include in managed care arrangements, leading to considerable variation across states. States have been largely responsible for monitoring and overseeing managed care plans, while federal rules have evolved over time. Historically, publicly available managed care performance data has been limited and inconsistently available across states, limiting transparency and accountability of individual plans.
Sweeping changes to Medicaid managed care rules and regulations in 2016 and 2024 included provisions related to beneficiary protections, access, and program oversight, including new managed care reporting and oversight requirements and efforts to promote transparency. The first Trump administration relaxed some managed care requirements in rules issued in 2020, but the administration left the managed care reporting requirements intact. To date, the Centers for Medicare and Medicaid Services (CMS) has continued to publicly post newly collected state managed care reports on Medicaid.gov. It remains uncertain whether the Trump administration will seek to roll back or revise provisions included in the 2024 managed care final rules.
This brief describes the Managed Care Program Annual Report (“MCPAR”), a relatively new, comprehensive report on state managed care programs that includes plan-level data, that must be submitted (to CMS) by states annually. It functions alongside other managed care reports aimed at improving state and federal managed care program monitoring, oversight, and transparency. (Future KFF analysis will explore policy relevant metrics from the data.)
MCPAR Background
By introducing the MCPAR reporting requirement, CMS intended to address the fragmented program information it received from states and to improve managed care program oversight. In finalizing the MCPAR requirement in 2016, CMS indicated it expected the reports would provide valuable and timely information to assess managed care program operations in each state and would improve transparency. In its June 2021 guidance, CMS noted the structured data collected from MCPARs (and other newly required managed care reports) would allow for the analysis of state-specific and national data and that CMS could use these data to assist states in improving their managed care programs while also ensuring compliance with federal laws and regulations. See Appendix for additional information on key administrative actions related to the MCPAR.
The first MCPARs were due to CMS between December 2022 and September 2023 (with due dates dependent on the managed care contract period). Following the release of CMS guidance in June 2021 that triggered the 2016 requirement, states are required to submit one MCPAR report for each managed care program the state administers, no later than 180 days after each program’s contract year (which typically operate on a calendar- or state fiscal year-basis). A managed care “program” is defined by a specified set of benefits and eligibility criteria identified in managed care plan contracts.1 A state may run separate programs for different populations (e.g., children, adults, etc.). As of February 2026, CMS has made MCPAR reports from 2023 and 2024 available on Medicaid.gov. (States are also required to post MCPARs on their websites; however, it is unclear how many states have posted their MCPAR reports. The 2024 rule reaffirmed regulatory transparency requirements and sets a timeframe (within 30 calendar days of submitting to CMS) for posting MCPARs on state websites.)
MCPAR Data
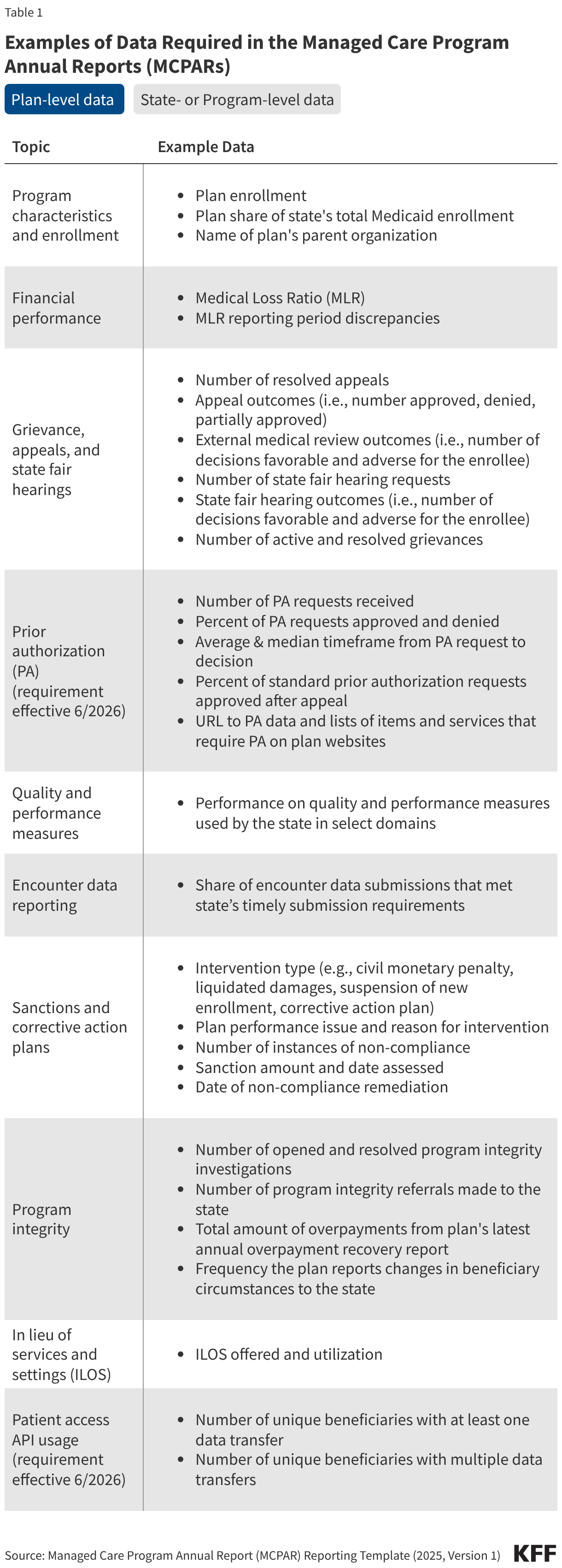
The MCPAR collects data across many areas of managed care program operations, including plan-level data (Table 1). Notably, the MCPAR template is designed to collect plan-level data in specific areas including enrollment, prior authorization, grievances and appeals, quality measures, encounter data submissions, sanctions, program integrity, and financial performance. While there are some limitations (discussed in more detail below), plan-level data can be used to analyze and compare individual plan performance within and across states. In addition, the MCPAR template collects state- and program-level data – for example, providing information on certain state monitoring activities, contract requirements, and program characteristics.
The bullets below provide additional context and information involving select MCPAR data elements/domains that are often cited as key to improving managed care oversight and transparency:
- Grievances and appeals. Plan-level data on appeals and grievances can help reveal quality and access issues. MCPAR reported grievance and appeal data include the total number of appeals and grievances resolved, the service types and reasons for appeals and grievances, the total number of state fair hearings and their outcomes, and the outcomes of external medical reviews (if offered by the state). Previously, states were not required to report appeals and grievances data to CMS.
- Prior authorization. The original MCPAR reporting template did not require states to track the number of prior authorization denials or appeal outcomes. Beginning with MCPAR reports submitted in June 2026, states will be required to report new plan-level prior authorization data, including the total number prior authorization requests, denial and approval rates, the percentage of standard prior authorization requests that were approved after appeal, and average and median decision times. These new data can be used to assess timeliness of prior authorization decisions, the extent of plan denials, and plan-wide issues with access to care. CMS expanded prior authorization reporting requirements following the release of an Office of Inspector General (OIG) report that raised concerns about the high number and rates of denied prior authorization requests by some plans and concerns that states were not adequately overseeing and monitoring MCO decisions on prior authorization requests. MCPAR prior authorization reporting requirements align with public reporting requirements included in the 2024 Interoperability and Prior Authorization rule.
- Sanctions. States may impose monetary or non-monetary sanctions on managed care plans if they do not meet contractual obligations. Historically, publicly available data on states’ use of sanctions has varied across states. A recent MACPAC state scan indicated the most common sanction tools identified in managed care contracts include monetary penalties, corrective action plans, and administrative/corrective actions. The MCPAR template collects plan-level data on state-imposed sanctions. Reported elements include intervention type (e.g., civil monetary penalty, liquidated damages, suspension of new enrollment, correction action plan), performance issues (e.g., quality measure performance, network adequacy, timely payment to providers), and sanction amount (if applicable/a monetary penalty was imposed).
- Program integrity. Plans are required to conduct a variety of program integrity activities. For example, plans must have a system for routine internal monitoring and auditing of compliance risks, promptly report to the state all overpayments identified or recovered, and notify the state if they receive information regarding changes to enrollee and provider eligibility. The MCPAR collects data related to plan program integrity activities, including plan-level data on managed care provider overpayments recovered, the number of program integrity investigations opened and resolved by plans, and how frequently plans report changes in beneficiary circumstances to the state. The reports also collect data on state program integrity responsibilities including contract standards for overpayments, how the state monitors overpayment reporting, and links to audits of plan encounter and financial data.
MCPAR Limitations
While the data and information contained in MCPARs have the potential to facilitate assessment and comparison of plan performance within and across states, there are also limitations. For example:
- Relatively new requirements. MCPARs are still in the initial years of implementation. The MCPAR template has evolved since its initial release. CMS is likely to continue to refine MCPAR reporting requirements and instructions to ensure consistency across states and to improve data quality and completeness.
- Data variation & comparability. There is significant variation across states in managed care programs (populations served, benefits), plan contract requirements, and state monitoring and oversight approaches. As a result, direct comparison across states, particularly in certain areas, may be challenging. States may also use inconsistent methods for certain metrics or reporting may be inconsistent across states.
- Importance of contextualized data. Without context, MCPAR data may be difficult to interpret in some areas. For example, listing sanctions without context may make it difficult to determine the significance of the noncompliance or the state’s approach to enforcing contract compliance issues. Low numbers of appeals and grievances could reflect few adverse benefit determinations, that access to care met enrollees’ needs, or that the plan does not adequately categorize or track appeals and grievances.
- Scope. MCPARs do not capture all aspects of managed care program and plan performance. MCPARs are also not the only source of plan or program performance information. Additional data can be found in other reports, including the MLR summary report and external quality review (EQR) annual technical report.
- Report format. TheMCPAR reports are currently posted on Medicaid.gov as PDF files, which allows for a centralized, uniform report repository. While the reports are posted publicly, they are technical and may be difficult for the general public/consumers to understand or gain actionable insights.
- Report period. As states operate with different contract years, the timing of data submission and the scope of reported data can differ (including number of months covered).
- Timeliness. The lag in time between end of contract year and report posting (on Medicaid.gov or state website) may affect the immediacy and relevance of the data.
According to a March 2024 U.S. Government Accountability Office (GAO) report, CMS had developed a draft plan (as of April 2023) for processing and analyzing MCPAR data, including developing an analytic dashboard, publishing summary reports and state-level data, and implementing an oversight plan. While CMS began publishing state MCPAR reports on Medicaid.gov in July 2024, CMS indicated to GAO they planned to prioritize working with states on data quality and technical assistance before implementing next steps related to data use and oversight. In November 2025, CMS told GAO that the agency is working on developing an internal appeals and grievance dashboard, to facilitate using the data for oversight, with planned implementation by June 2026. MACPAC is also currently examining state and federal tools for ensuring accountability of managed care organizations and may issue additional policy recommendations in a future report.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Appendix
Key Administrative Actions Related to the MCPAR
Federal oversight has primarily focused on reviewing and approving plan contracts and capitation rates, and states have generally had considerable flexibility in implementing federal managed care monitoring and oversight requirements. While states have historically produced a variety of data and reports on their managed care programs (e.g., encounter data, external quality reviews etc.), states were not required to produce or submit standardized, comprehensive managed care program reports. Publicly available managed care performance data has been limited and inconsistently available across states, limiting transparency. The following bullets track administrative action related to introducing and implementing the MCPAR reporting requirements:
- 2016. In 2016, under the Obama Administration, CMS issued sweeping managed care regulations to advance program goals related to access, quality, fiscal and program integrity, beneficiary protections, and monitoring and oversight. The rules created new managed care reporting requirements, requiring states to submit three annual reports: 1) an annual managed care program report, 2) a network adequacy and access report, and 3) a medical loss ratio (MLR) summary report. Implementation of the reporting requirements was phased in. However, the first annual managed care program reports were not due until CMS issued guidance on the content and form of the report.
- 2017-2020. In 2017, under the first Trump administration, CMS indicated it would use “enforcement discretion” to allow states to postpone compliance with certain managed care rules introduced in 2016 (although it’s unclear what enforcement discretion was offered and to which states). In 2020, CMS finalized revisions to Medicaid managed care rules in specific areas (e.g., relaxing network adequacy requirements and beneficiary protections) aimed at reducing state and federal burden, streamlining regulations, improving rate setting transparency, and promoting state flexibility. The new managed care reporting requirements from the 2016 rule were left intact, including the annual managed care program report requirement, though the administration did not issue further guidance to effectuate the reporting requirement.
- 2021-2024. In June 2021, the Biden administration released guidance that triggered the annual managed care program report (referred to now as the managed care program annual report or “MCPAR”) requirement, developed standard reporting templates (for the MCPAR, network adequacy and access report, and MLR Summary report) and a variety of toolkits, and released a series of informational bulletins on managed care monitoring and oversight. The first MCPAR reports were due to CMS in December 2022. To improve transparency, CMS began posting state-submitted MCPAR (and MLR Summary) reports on Medicaid.gov in 2024 (from “performance year” 2023). In 2024, the Biden administration also issued significant new Medicaid managed care regulations aimed at improving access, quality of care, and monitoring and transparency, including expanding MCPAR reporting elements and transparency requirements.
- 2025 and beyond. The second Trump administration has continued to post state-submitted MCPAR reports on Medicaid.gov (reports from 2024 were posted in 2025). The administration has also made minor revisions and additions to the MCPAR template2 and released an updated MCPAR “FAQ” in August 2025. CMS has also given states the option to forgo completing the access and network adequacy sections of the MCPAR, noting this option was introduced to reduce state burden and duplication with the separate network adequacy and access report; however, it may also reduce transparency as the network adequacy and access report is not currently posted on Medicaid.gov. In November 2025, CMS told GAO that the agency is working on developing an internal appeals and grievance dashboard, to facilitate using the data for oversight, with planned implementation by June 2026. Beginning with MCPAR reports submitted in June 2026, states are required to report new plan-level prior authorization data including the total number prior authorization requests, denial and approval rates, appeal outcomes, and average and median decision times. The 2024 managed care rule requires states to include the results of enrollee experience surveys in the MCPAR (for contract rating periods that begin on/after July 9, 2027).
- States must submit MCPAR reports for MCO programs and for limited benefit prepaid inpatient health plan (PIHP) and prepaid ambulatory health plan (PAHP) programs (except for PAHPs that only cover non-emergency medical transportation). States must also submit MCPAR reports for primary care case management (PCCM) entities but are only required to complete certain sections. ↩︎
- The Excel template posted on Medicaid.gov lists 2025 MCPAR updates and effective dates on the “Revisions” tab. ↩︎