Utilization of Health Care Services by Medicaid Expansion Status
Legislation passed by the House of Representatives on May 22nd includes a number of Medicaid provisions that would cut federal Medicaid spending by more than $700 billion over the next ten years and notably increase the number of people without health insurance. Provisions that would only apply to states that have adopted the ACA expansion account for more than half of all of the savings estimated by CBO. Some critics of Medicaid expansion have argued that expansion diverts resources away from other groups of Medicaid enrollees, including people with disabilities and children, and that expansion enrollees are “able-bodied” implying they have minimal health care needs. However, data show that expansion states spend more per enrollee overall and on each eligibility group than non-expansion states and that nearly half of expansion enrollees have a chronic condition. This data note builds on a previous analysis about Medicaid expansion enrollees to understand more about their health care utilization patterns compared to other enrollees. Specifically, this data note analyzes 2021 Medicaid claims data to compare utilization of health care services among Medicaid expansion enrollees with other Medicaid enrollees in expansion states and to compare utilization of health care services among adult Medicaid enrollees living in expansion and non-expansion states.
In expansion states, adults covered through the ACA expansion use more services than other adults who are eligible on the basis of having low-income (Figure 1). While some groups claim that expansion adults are primarily “able-bodied” adults with minimal health needs, analysis of 2021 Medicaid claims data finds that expansion adults were more likely to use prescription drugs (62% vs. 55%) and behavioral health treatment (30% vs 23%) compared to other adults. High utilization of these services by expansion adults likely reflects that one-third have a chronic physical health condition and a quarter have a chronic behavioral health condition. However, their utilization rates were lower than rates among adults who qualified on the basis of having a disability.

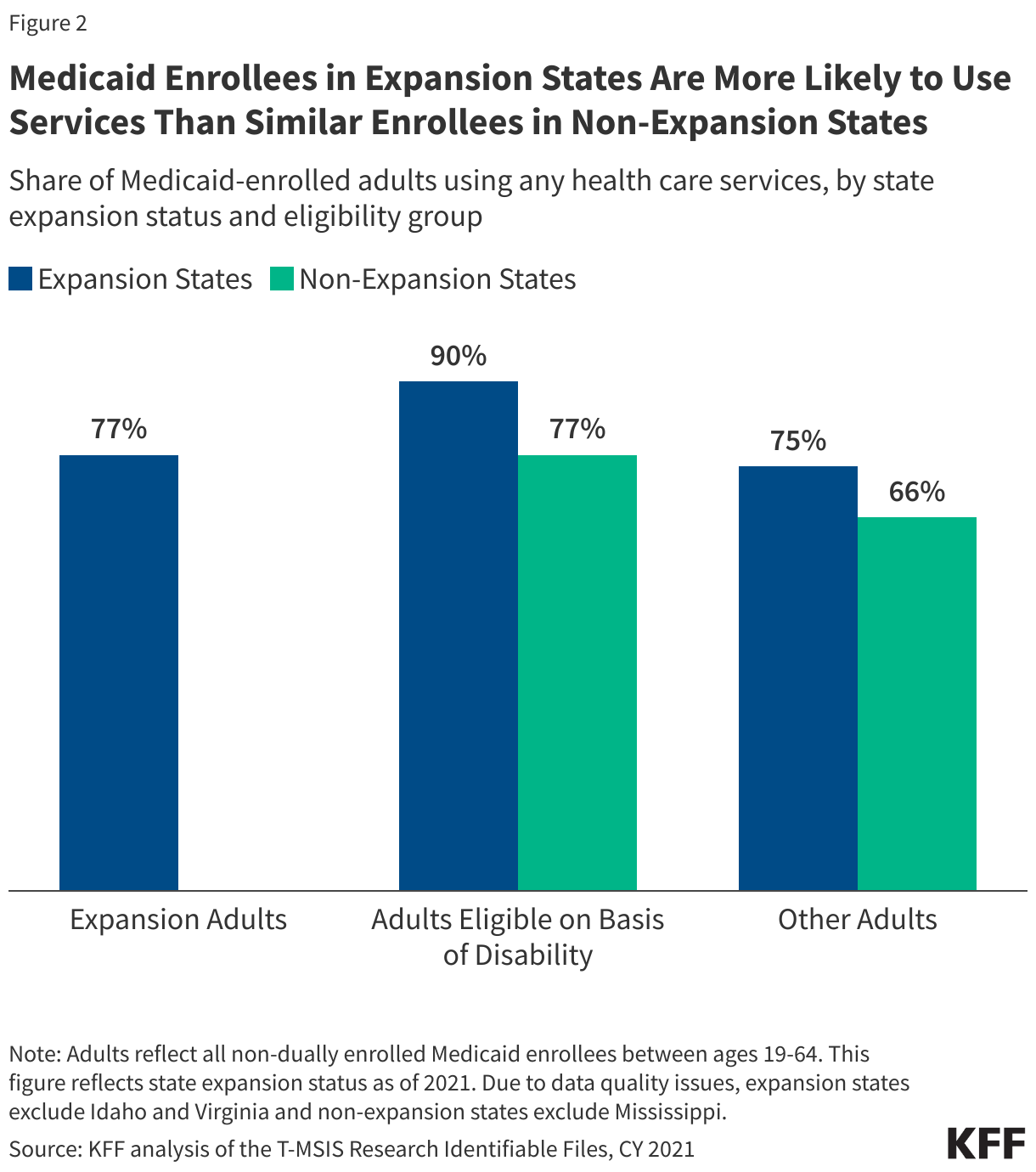
Medicaid enrollees in expansion states are more likely to use health care services than similar enrollees in non-expansion states (Figure 2). Though some groups suggest that Medicaid expansion takes resources away from traditional Medicaid enrollees, analysis of 2021 Medicaid claims finds that rates of health care utilization among adults in expansion states is higher than utilization among adults in non-expansion states. About 90% of adults eligible for Medicaid on the basis of disability in expansion states used any health care services, compared with just 77% of adults eligible on the basis of disability in non-expansion states. Similarly, excluding adults who qualified through the expansion pathway, 75% of other adults in expansion states (those who qualified for Medicaid on the basis of low-income) used health care services, while just 66% of their counterparts in non-expansion states had any utilization. Notably, expansion adults had similar utilization rates as adults eligible on the basis of disability in non-expansion states.
A state’s expansion status is not the sole reason for the variation in utilization rates. Rather, there are a variety of factors that may contribute to this variation, including substantial differences in state adoption of optional long-term care and behavioral health care programs; provider participation in such programs; and variation in the duration and scope of covered benefits as well as cost sharing requirements.
These differences in utilization persist for specific services for low-income adults and people with disabilities (Figure 3). Adults eligible on the basis of low-income (excluding those eligible through the ACA expansion) in expansion states had notably higher utilization of certain services than those in non-expansion states, including outpatient care (64% vs 58%) and prescription drugs (55% vs 47%).
Similarly, among adults eligible on the basis of disability, utilization of certain services needed to manage their conditions is higher in expansion states than in non-expansion states. In expansion states, 81% of adults with disabilities had any claims for prescription drugs compared to just 63% of those in non-expansion states. These enrollees in expansion states were also over twice as likely to use long-term care (25% vs 12%) and had higher utilization of behavioral health treatment services (62% vs 44%) as those in non-expansion states.
When controlling for health status, enrollees in expansion states still had higher rates of utilization than those in non-expansion states (Figure 3). Enrollees who qualified on the basis of disability and who had three or more diagnosed chronic conditions had the highest utilization rates of prescription drugs, long-term care, and behavioral health treatment in both expansion and non-expansion states, compared to all other adult enrollees. However, within this group of adults with particularly high health care needs, those in expansion states had higher utilization than those in non-expansion states for prescription drugs (98% vs. 93%), long-term care (33% vs. 23%), and behavioral health treatment (84% vs. 78%). (The measure of overall utilization for those with chronic conditions is not reported since enrollees have to have at least one health care claim to have a chronic condition diagnosis.)

Methods
Medicaid Claims Data: This analysis uses the 2021 T-MSIS Research Identifiable Demographic-Eligibility and Claims Files (T-MSIS data) to identify Medicaid expansion enrollees, utilization, and chronic conditions.
State Inclusion Criteria:
- Expansion states: Though Idaho and Virginia expanded Medicaid prior to 2021, adult expansion enrollees primarily show up in the traditional adult eligibility group. Therefore, those expansion states are excluded.
- Non-expansion states: Mississippi was also excluded from this analysis due to data quality concerns flagged by the DQ Atlas.
Enrollee Inclusion Criteria: Enrollees were included if they were ages 19-64, had full Medicaid coverage for at least one month, and were not dually enrolled in Medicare. Dually enrolled individuals were excluded from these calculations since they may not have had sufficient claims in T-MSIS to identify utilization.
Identifying Utilization: This analysis defines health care utilization in T-MSIS using the following methods:
- Any utilization: Where CLM_TYPE_CD equals 1, 3, 4, A, C, D, U, W, or X
- Inpatient hospital: Where TOS_CD equals 001, 060, 061, 090-093, and 132
- Outpatient care: Where TOS_CD equals 002-008, 012, 028, 042, 134, 135
- Drugs: Where TOS_CD equals 033, 034, and 131; or where TOS_CD equals 145 and the claim is in the RX file
- Long-term care: See our brief on long-term care users for methods
- Behavioral health treatment: SUD and mental health treatment are identified using the Behavioral Health Service Algorithm (BHSA) reference codes provided by The Urban Institute.
Defining Chronic Conditions (Figure 3): This table identifies Medicaid enrollees with three or more chronic conditions. This analysis used the CCW algorithm for identifying chronic conditions (updated in 2020). This analysis also included in its definition of chronic conditions substance use disorder, mental health, obesity, HIV, hepatitis C, and intellectual and developmental disabilities. In total, 35 chronic conditions were included.
