5 Key Facts About Nursing Facilities and Medicaid
The substantial Medicaid savings in the reconciliation bill that has been passed by the House could have major implications for nearly 15,000 federally certified nursing facilities and the 1.2 million people living in them. Nursing facilities provide medical and personal care services for older adults and people with disabilities, and Medicaid covered 44% of long-term institutional care costs in 2023. In response to cuts in federal Medicaid spending, states could opt to lower Medicaid reimbursement rates for nursing facilities, which could result in reductions in staffing that are tied to lower nursing facility quality and poorer outcomes. A separate Medicaid provision would tighten eligibility by reducing the home equity limit overtime, making it more difficult for people to qualify for nursing facility, home care and other long-term care services.
The proposed legislation would also put a moratorium on implementing a Biden-era rule intended to help address long-standing concerns about staffing shortages and the quality of care in nursing homes. The Congressional Budget Office (CBO) estimates that eliminating the rule would save $23.1 billion over 10 years. Even if the legislation does not pass, a recent court decision overturned the first-ever minimum staffing ratios for nursing facilities that were part of the rule. The Trump administration is considered unlikely to appeal the court’s decision. Amid debates to limit federal Medicaid support, this brief provides information on how Medicaid programs support nursing facilities and the people living in them.
1. Medicaid is the primary payer for over 6 in 10 residents in nursing facilities.
As of July 2024, there were 1.2 million people living in nursing facilities, over 60% of whom had Medicaid as a primary payer. The share of people living in nursing facilities with Medicaid as their primary payer has remained steady, but the total number of residents living in nursing facilities decreased by 10% over the last decade. The decline in the total number of nursing home residents over the past decade may in part reflect a preference for home-based care, including care in assisted and independent living facilities, rather than in nursing facilities.
Medicaid is the primary payer for nursing facility care, providing long-term care services not offered by Medicare. Medicare covers up to 100 days of skilled nursing facility care following a qualifying hospital stay and does not cover long-term nursing facility care, custodial nursing facility care, or nursing facility care that does not follow a qualifying hospital stay. Despite Medicaid’s primary role in funding nursing facility services, KFF polling shows that four in ten people identify Medicare as the main source of coverage for low-income people in nursing facilities.

2. Medicaid paid for 44% of the $147 billion that the US spent on institutional long-term care in 2023.
Medicaid is the primary payer for long-term care (LTC) in the US, paying for at least 44% of institutional LTC and 69% of home care. Unlike Figure 1, which reflects the number of people using any nursing facility care, including short-term skilled care paid for by Medicare and other post-acute care payers, Figure 2 reflects spending on long-term institutional care only and excludes short term skilled care paid for by Medicare and other payers. The institutional care services in Figure 2 include costs for long-term nursing facility stays, intermediate care facilities, and continuing care retirement communities. The costs attributable to each type of facility are unknown because the National Health Expenditures data do not break these costs out separately. There are fewer nursing facility residents and nursing facilities than there were a decade ago, and more people use home care now than nursing facility care, leading to the higher U.S. spending on home care.

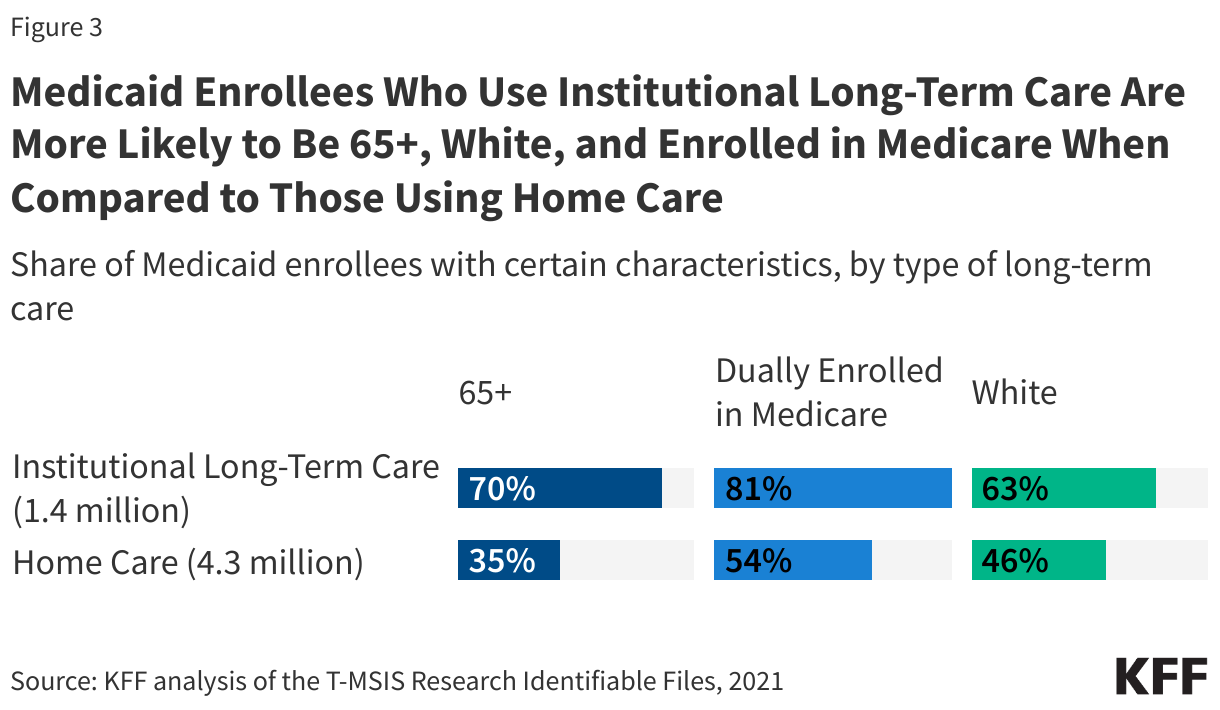
3. Medicaid enrollees who use institutional long-term care are more likely to be 65+, White, and enrolled in Medicare when compared to those using home care.
In 2021, there were 1.4 million people who used Medicaid institutional LTC throughout the year. This includes about 1.3 million people who used Medicaid nursing facility care and 0.1 million people who used care in an intermediate care facility. Figure 1 reports fewer people using nursing facility care since it captures the number of people in a nursing facility in a given month while Figure 3 reflects nursing facility use over the course of the year. Most Medicaid enrollees who use institutional LTC are ages 65 and older while most who use home care are under 65. Most Medicaid enrollees using institutional LTC are dually enrolled in Medicare, compared to just over half of those using home care. People who use institutional LTC are also more likely to be White than those using home care.
4. Medicaid financing for nursing facilities is complex.
There are four main sources of Medicaid funding for nursing facilities including:
- Payments from the state to nursing facilities that are tied to specific patient care (known as fee-for-service or FFS base payments),
- Payments from a private health plan to nursing facilities that are tied to specific patient care in cases where the state is paying private health plans to provide Medicaid benefits (known as managed care payments),
- Payments from nursing facility residents (which represent patient cost sharing), and
- Supplemental payments from states to nursing facilities that are not tied to specific patients.
According to the Medicaid and CHIP Payment and Access Commission, fee-for-service payments are the largest source of Medicaid spending (57%) followed by managed care payments (29%). Residents paid 9% of the total, and the remaining 5% came from supplemental payments to providers.
Under current law, states are permitted to finance the non-federal share of Medicaid spending through multiple sources including healthcare-related taxes or “provider taxes”, though legislation that has been passed by the House would prohibit states from establishing any new provider taxes or increasing the rates of existing taxes. CBO estimates that the moratorium would save $89.3 billion over 10 years. Provider taxes are defined as state taxes where at least 85% of the tax burden falls on health care items or services or entities that provide or pay for health care. All but six states finance part of the state share of nursing facility spending with provider taxes on nursing facilities, and the moratorium or new or addition taxes could limit states’ options to fund their share of nursing facility costs in the future, potentially resulting in reduced Medicaid spending, coverage, and payment rates to nursing facilities. States may also finance the state share of payments with intergovernmental transfers or certified public expenditures for the 6% of nursing facilities that are publicly owned (although this varies across the states from less than 1% in the District of Columbia and Connecticut to 43% in Wyoming).

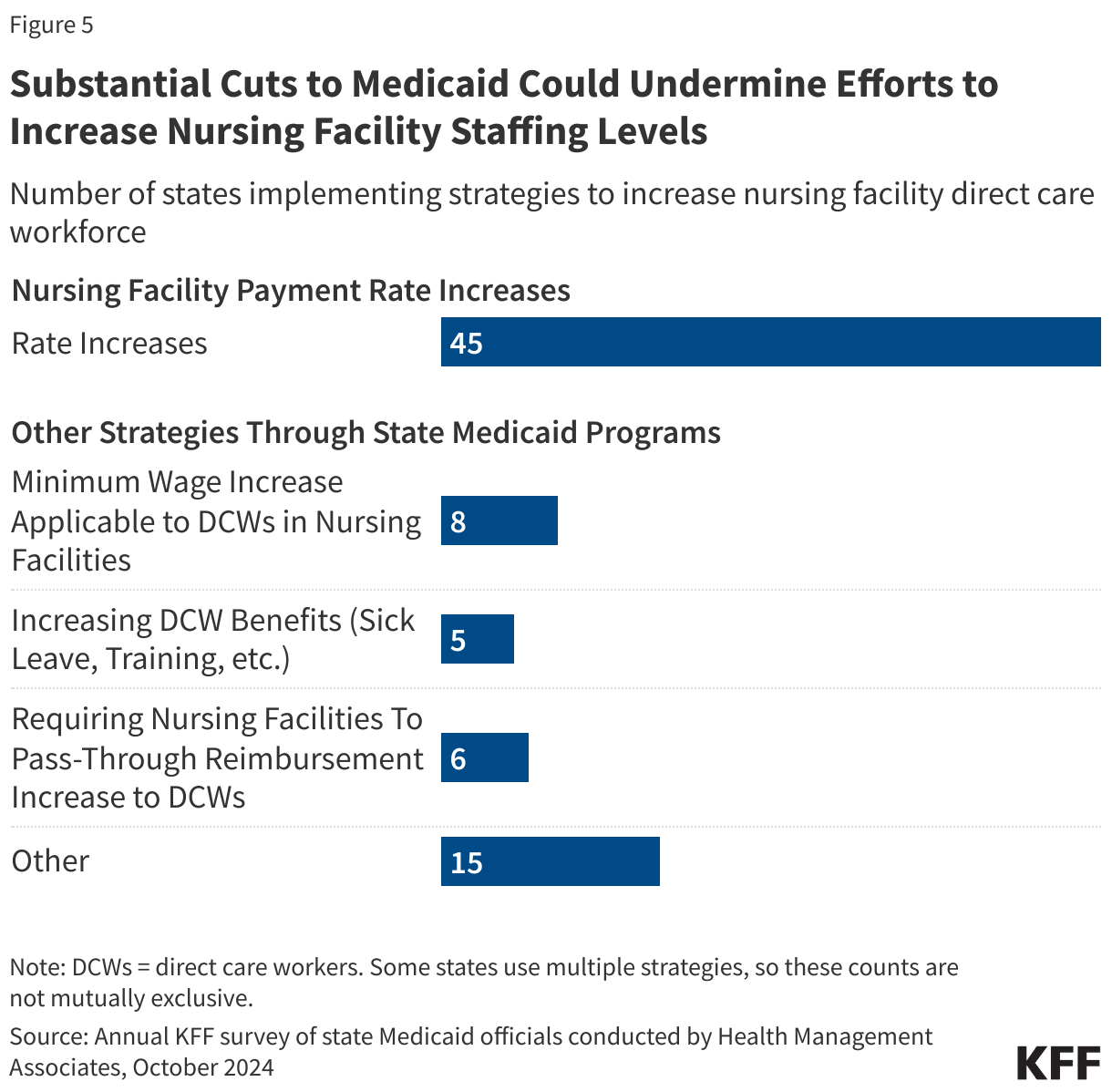
5. Substantial cuts to Medicaid could undermine efforts to increase nursing facility staffing levels.
Research finds that higher staffing levels in nursing facilities have been consistently tied to better outcomes for residents and are closely tied to overall quality of care. States are currently leveraging Medicaid to support nursing facility staffing efforts through higher payment rates, but those payment rates may be unsustainable if Medicaid spending is significantly cut. In a 2024 survey of state Medicaid programs, most states (45 of 49 reporting states) reported increasing nursing facility FFS base rates in both FY 2024 and FY 2025 in response to staffing shortages. Several states reported particularly significant nursing facility base rate increases, including Iowa with a 25.49% base rate increase and Ohio with a 17% increase.
Beyond increasing payment rates, states are making efforts to bolster nursing facility staffing by leveraging Medicaid to strengthen the nursing facility direct care workforce. These strategies include increases to minimum wage that would apply to workers in nursing facilities (eight states), strengthening direct care worker benefits (five states), and requiring nursing facilities to pass reimbursement increases through to the workforce (six states). Other strategies adopted by state Medicaid programs include efforts to promote and subsidize health care careers, increased payments to nursing facilities for maintaining higher levels of staffing, and incentive payments for demonstrating that a certain share of a nursing facility’s total revenue was spent on workforce compensation and benefits.
This work was supported in part by The John A. Hartford Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
