HIV Policy Alignment with International Standards in PEPFAR Countries
Introduction
Key Findings
- Adoption of evidence-based guidelines, laws, and policies is important for improving HIV-related health outcomes. While PEPFAR’s primary focus is on HIV service delivery, it also aims to create conditions within countries that can contribute to successful implementation of HIV programs, which includes helping to foster policy environments through both operational guidance and diplomacy.
- We examined the policy environments in PEPFAR countries to assess alignment with international HIV-related standards, looking at four main categories (clinical care and treatment, testing and prevention, structural, and health systems). We also compared PEPFAR countries to other low- and middle-income countries (LMICs).
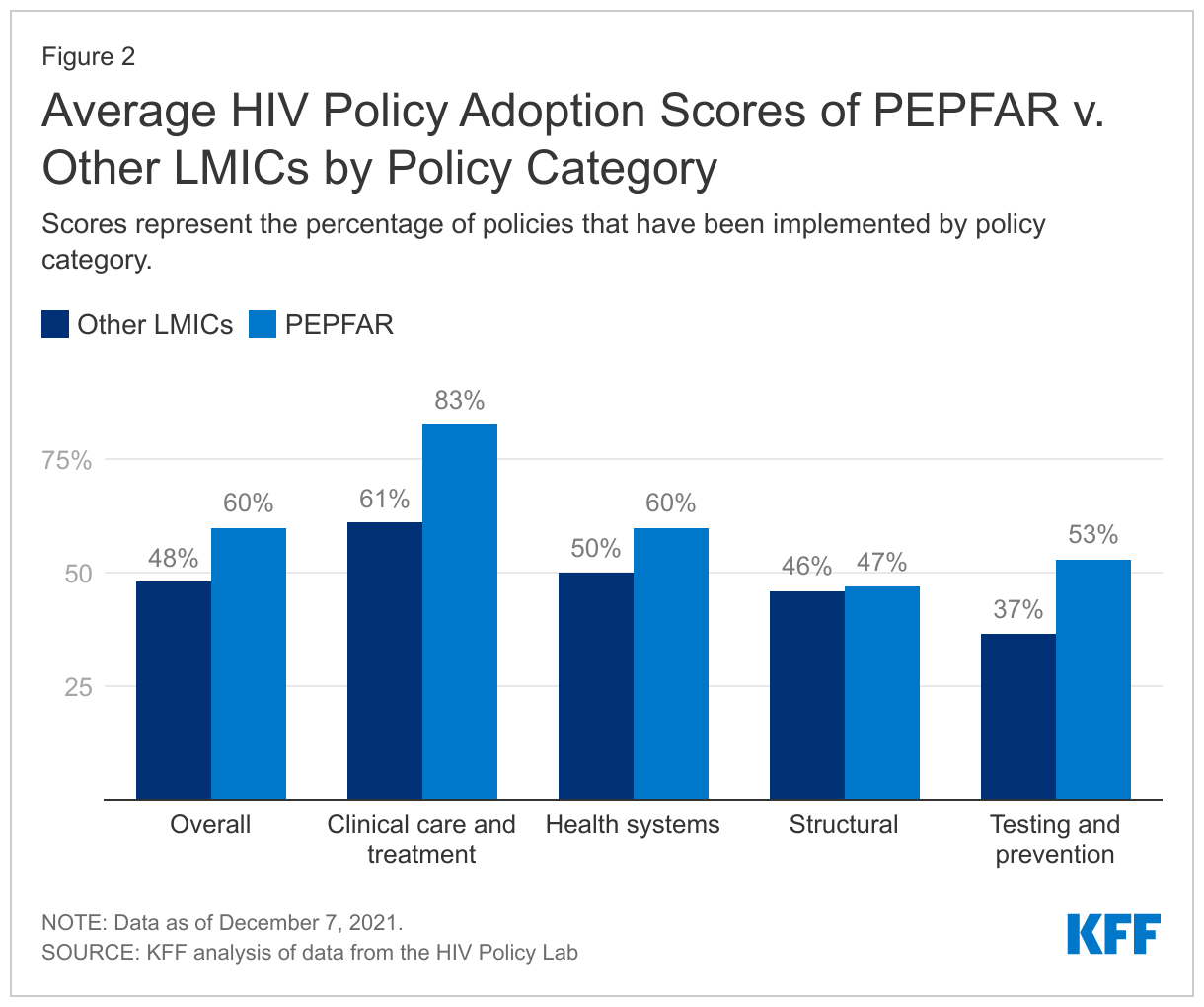
- Overall, we find that PEPFAR countries have stronger policy alignment than other LMICs – PEPFAR countries as a group have adopted 60% of recommended policies, compared with 48% among other LMICs, and PEPFAR countries have higher alignment scores than other LMICs in three of the four categories.
- Policy alignment was particularly strong, including relative to other LMICs, in areas in which PEPFAR directly focuses and supports. PEPFAR countries scored highest (81%) in the area of clinical care and treatment, which includes policies related to early treatment initiation, treatment regimens, and viral load testing, and scored 20 percentage points higher than other LMICs. While the overall score on testing and prevention was lower than that of clinical care and treatment, there was still a large differential compared to other LMICs (57% compared to 37%). Scores were lowest and similar for both groups on policies and laws related to structural factors, such as HIV-related non-criminalization policies.
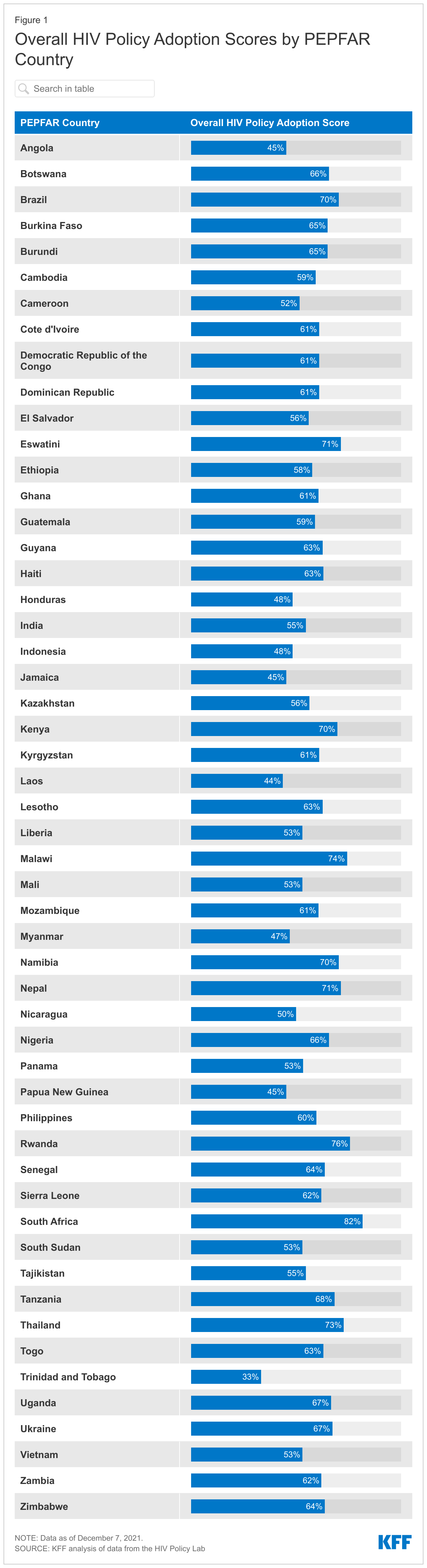
- Policy alignment across PEPFAR countries varies substantially – overall policy adoption scores range from 33% in Trinidad & Tobago to 82% in South Africa and there is also variation within each main category – for instance, while no PEPFAR country has adopted policies related to drug use non-criminalization (structural), all 53 PEPFAR countries have fully aligned viral load testing policies (clinical care and treatment) with international standards.
- While PEPFAR countries scored higher than other LMICs overall, a significant share of recommended policies have yet to be adopted in PEPFAR countries, particularly in the area of structural barriers, which may be the most difficult to affect at the country level, given that they often require national legal changes and/or reach beyond HIV. Going forward, these findings may serve as a baseline for targeting and assessing future PEPFAR efforts as the program seeks to further improve HIV outcomes in the countries within which it works.
Introduction
The U.S. government’s President’s Emergency Plan for AIDS Relief (PEPFAR), the world’s largest commitment by any nation to address a single disease, has played a significant role in addressing HIV/AIDS in the hardest-hit countries around the world and is credited with helping to shift the trajectory of the epidemic.1 While most of PEPFAR’s efforts are focused on providing services to those with and at risk for HIV, PEPFAR also aims to create conditions that can contribute to the successful implementation of HIV programs. 2 ,3 ,4 This includes working to foster the adoption of normative, evidence-based guidance and policies developed by international bodies aimed at improving HIV-related health outcomes.5 ,6 ,7
Through its operational guidance and direct diplomatic engagement,8 PEPFAR has worked to encourage and in some cases require that country programs adopt certain policies, such as new antiretroviral treatment guidelines; differentiated service delivery9 – including multi-month dispensing of antiretrovirals (ARVs) to reduce the need for frequent refills, which has become particularly important to ensure continuity of treatment during COVID-19; and the removal of user fees that can serve as obstacles to HIV service access; as well as increase domestic budgets for HIV.10 ,11 ,12 ,13 ,14 PEPFAR also has emphasized the importance of addressing stigma and a human rights approach, particularly for reaching key populations that some societies have historically shunned.15 ,16 ,17 ,18 As a result, the program has been found to have played an important role in helping to shape the HIV policy environments in the countries in which it operates.19 ,20 ,21 ,22 ,23 ,24
We sought to assess policy alignment with international HIV standards in PEPFAR countries. We included PEPFAR countries that were required to develop Country or Regional Operating Plans (COPs or ROPs), which are used for approval of funding and serve as annual strategic plans for U.S. HIV/AIDS efforts in host countries in 2020.25 ,26 ,27 In addition to assessing how PEPFAR COP/ROP countries align with international standards, we also compared this group to other LMICs.28 ,29
Because we looked only at a point-in-time snapshot, findings cannot necessarily be attributed to PEPFAR. Rather, they may serve as a baseline for targeting and assessing future PEPFAR efforts, as the program seeks to further improve HIV outcomes in the countries within which it works. It is possible that policies may have changed in PEPFAR countries since we completed the analysis. For instance, according to a presentation by PEPFAR headquarters staff to stakeholders on August 2, 2021, numerous PEPFAR countries have been making modifications to their polices or guidelines related to multi-month dispensing of antiretrovirals during the COVID-19 pandemic.30
Methods31 ,32
We analyzed data from the HIV Policy Lab, a joint project of Georgetown University’s O’Neill Institute and other academic, civil society, and multilateral partners, with the support of PEPFAR, which compiles and measures the HIV-related policies of the 194 World Health Organization (WHO) member states against international normative guidance. The policies that the HIV Policy Lab uses as benchmarks are those recommended by internationally-recognized authorities, including the WHO, UNAIDS, the U.N. Development Programme, the Global Commission on HIV and the Law, and others based on current science and evidence and aimed at improving HIV-related outcomes. The HIV Policy Lab database uses information reported by governments through the National Commitments and Policy Instrument (NCPI) housed on UNAIDS’ Laws and Policies Analytics platform,33 and collects additional data from official countries sources, reports from U.N. member states, and other partner organizations.
We used the most recent year of data available (through 2020) on policies by country to assess their status in 53 PEPFAR countries required to submit a COP and ROP in 2020, and 85 other LMICs that either did not receive PEPFAR support (82 countries) or received some U.S. HIV support, but were not required to submit a COP or ROP in 2020 (3 countries).34 ,35 ,36 We included the full set of 33 indicators – along with more than 30 sub-indicators – across the four categories that the HIV Policy Lab tracks: clinical care and treatment; testing and prevention; health systems; and structural barriers (see Table 1 and the Appendix; more detailed explanations of each indicator can be found in the HIV Policy Lab’s Codebook).
For each indicator where data are available, the HIV Policy Lab assigns points based on adoption status – “Adopted” (1 point), “Partially Adopted” (0.5), and “Not Adopted” (0). For indicators with sub-indicators, the HIV Policy Lab assigns a full point if all sub-indicators are adopted, a half point (0.5) if some are adopted, and 0 if none are adopted. The points for all indicators are added to obtain a raw score for each country. Adoption percentages are calculated by dividing the raw scores by the total possible scores; indicators for which there are no data available are excluded. Scores for groups (e.g., PEPFAR countries, regions) were calculated by averaging country scores at the overall- and category-level. Scores presented in the text are for the main indicators unless otherwise noted. Countries without data were excluded.
Our analysis is based on data downloaded on December 7, 2021.
| Table 1: Policy Indicators Included in Analysis, by Category | |||
| Clinical Care and Treatment | Testing and Prevention | Health Systems | Structural |
| Treatment Initiation | Self-testing | Task Shifting | Same-sex Sex Non-Criminalization |
| Same-day Treatment Start | Partner Notification/Index Testing | Healthcare Financing | Sex Work Non-Criminalization |
| Treatment Regimen | Compulsory Testing | Universal Health Coverage | Drug Use Non-Criminalization |
| Differentiated Service Delivery | Age Restrictions on Testing & Treatment | User Fees | HIV Exposure Non-Criminalization |
| Viral Load Testing | PrEP | Access to Medicines (TRIPS) | Non-discrimination Protections |
| Pediatric Diagnosis & Treatment | Harm Reduction | Unique Identifiers with Data Protections | National Human Rights Institutions |
| Migrant Access to Healthcare | Comprehensive Sexuality Education | Data Sharing | Constitutional Right to Health |
| Tuberculosis Diagnosis | Prisoners Prevention | Girls Education | |
| Gender-based Violence | |||
| Civil Society | |||
Findings
PEPFAR countries, as a group, have greater policy alignment, than other LMICs.
- Overall, PEPFAR countries have an average adoption score of 60% for the recommended policies, compared to 48% for other LMICs. Policy adoption scores in PEPFAR countries range from 33% in Trinidad & Tobago to a high of 82% in South Africa (see Figure 1).
- PEPFAR countries score higher on three of the four policy categories tracked, with an average score 22 percentage points greater than that of other LMICs for clinical care and treatment indicators; 16 percentage points higher for testing and prevention indicators; and 10 points higher for health systems indicators. The score for the fourth category — structural indicators – was similar to that of other LMICs (see Figure 2).
PEPFAR countries have the strongest policy alignment in the area of clinical care and treatment and the weakest on structural indicators.
- On average, PEPFAR countries have an adoption score of 83% for policies related to clinical care and treatment (see Figure 2), ranging from a low of 31% (Nicaragua) to a high of 100% in eight countries (Eswatini, Ethiopia, Haiti, Malawi, Papua New Guinea, South Sudan, Uganda, and Zimbabwe).
- For testing and prevention indicators, PEPFAR countries have an average adoption score of 53%, ranging from 0% (Trinidad and Tobago) to 94% (Nigeria).
- PEPFAR countries scored an average of 60% for health systems indicators, ranging from 14% (Laos) to 93% in three countries (Eswatini, South Africa, and Thailand).
- PEPFAR countries have the weakest alignment for policies related to structural indicators (47%), with Lesotho scoring the lowest in this category at 11%, and Rwanda and South Africa scoring the highest at 70%.
There is also significant variation in policy alignment within each main category– for instance, while no PEPFAR country has adopted policies related to drug use non-criminalization (structural), all 53 PEPFAR countries have fully aligned viral load testing policies (clinical care and treatment) with international standards.
Clinical Care and Treatment
- All PEPFAR countries in this analysis (53) have fully adopted viral load testing policies aligned with international standards (whether a national policy is in place to monitor viral load in people with HIV at least once a year). This was the only indicator among the 33 for which 100% of countries have fully aligned policies. Treatment initiation policies (whether a national policy is in place that states that people with HIV, regardless of CD4 count, are eligible to start treatment) followed closely with 52 of the 53 PEPFAR countries fully adopting.
- Differentiated service delivery (DSD) policies (whether national policy allows for differentiated HIV treatment services such as multi-month dispensing and community antiretroviral therapy) had the smallest share of PEPFAR countries fully adopting – 15 of the 53 PEPFAR countries, although an additional 36 had adopted some DSD policies.
Testing and Prevention
- Adoption of prevention policies is greatest for comprehensive sexuality education (whether national policies require curriculum that meets international standards be taught in primary and secondary schools), with 42 PEPFAR countries fully adopting (out of 52 with available data).
- Policies related to HIV prevention among prisoners (whether national policy stipulates that prevention tools, such as condoms, lubricants, and syringe access/exchange programs available to prisoners) were the least likely to be aligned, with just two countries (Kyrgyzstan and Tajikistan) fully adopting policies aligned with international standards (out of 52 with available data), although an additional 13 had adopted some policies in this area.
Health Systems
- Within this category, PEPFAR countries are most aligned on policies related to unique identifiers with data protections (whether the country utilizes unique identifiers for continuity of care across multiple facilities and has legally-enforceable data privacy protections) – 33 of 53 PEPFAR countries have policies fully aligned with international standards and an additional 17 countries had some national policy related to patient data protection.
- More than half of PEPFAR countries (27 of 52 with available data) have fully aligned policies related to user fees (whether national policy stipulates that public primary care and HIV services are available without user fees) and an additional 20 have adopted some policies in this area.
- PEPFAR countries are least likely to be aligned on policies related to universal health coverage of HIV treatment and PrEP (whether national health coverage includes medications for HIV treatment and PrEP) – 11 PEPFAR countries (out of 51 with available data) have fully aligned policies with international standards, with an additional 22 having adopted some policies related to universal health coverage of HIV treatment and PrEP.
Structural
- PEPFAR countries have the strongest alignment on policies related to gender-based violence – an indicator that assesses whether or not countries have laws that explicitly address domestic violence with enforceable penalties (42 of 53 countries).
- On the other end of the spectrum, no PEPFAR country has adopted policies related to drug use non-criminalization (whether national policy avoids criminalizing personal possession of drugs). Additionally, only three of 53 PEPFAR countries have policies related to sex work non-criminalization (whether national policy avoids criminalizing the buying, selling, and organizing of sex work) that are fully aligned with international standards (Haiti, Honduras, and Panama).

Discussion
While no PEPFAR country has fully aligned its laws and policies with international standards, this analysis shows that they have, on average, greater alignment than other LMICs and this differential is greatest in areas in which PEPFAR focuses most of its direct support, such as treatment and testing policies. As noted above, PEPFAR has actively worked toward changing local policies in countries, principally with regard to the adoption of treatment guidelines, the removal of user fees for HIV services, and the implementation of differentiated service delivery strategies, such as the multi-month dispensing of antiretrovirals – which has become critically important during the COVID-19 pandemic – and increasing domestic budgets for HIV. Further, PEPFAR has played a role in spotlighting the need for countries to address HIV among some of the most vulnerable populations, which have been historically shunned by some countries. At the same time, as this analysis demonstrates, there is still a significant share of recommended policies that have yet to be adopted in PEPFAR countries, particularly in the area of structural barriers, such as policies related to non-discrimination of marginalized groups and decriminalization of activities including sex work and drug use, which may be the most difficult to affect at the country level given that they often require national legal changes and/or reach beyond HIV.
While the data included in this analysis do not measure the extent or quality of implementation, policy adoption can be viewed as a step in the direction of evidence-based practices and indicate a country’s commitment to addressing HIV and creating a foundation that can facilitate and optimize HIV/AIDS efforts. This is especially important in PEPFAR countries, which include those that have been hardest hit by the HIV/AIDS epidemic. Indeed, PEPFAR’s most recent draft guidance to COP and ROP countries for 2022 places an even greater premium on policy change, including requiring country programs to either ensure change in some areas as a condition of receiving funding, or submit a detailed description of existing barriers and proposed plan to be able to meet these requirements.
Looking ahead, there are important questions surrounding PEPFAR’s role, beyond service delivery, in countries, especially as the program awaits the confirmation of a new coordinator, is expected to release a new five-year strategy, and is due for reauthorization in two years, all of which could provide openings for strengthening PEPFAR even further. The findings presented here, while not necessarily attributable to PEPFAR, may serve as a baseline for targeting and assessing future PEPFAR efforts, as the program seeks to further improve HIV outcomes in the countries within which it works and policymakers consider PEPFAR’s next phase.
Appendix
| Appendix 1: Policy Indicators and Sub-Indicators Included in Analysis, by Category | ||
| Category | Name | Indicator or Sub-Indicator |
| Clinical care and treatment | Treatment initiation | Indicator |
| Same-day treatment start | Indicator | |
| Treatment regimen | Indicator | |
| Differentiated service delivery | Indicator | |
| Differentiated service delivery – Community ART distribution | Sub-indicator | |
| Differentiated service delivery – Clinical visit frequency | Sub-indicator | |
| Differentiated service delivery – Multi-month dispensing | Sub-indicator | |
| Viral load testing | Indicator | |
| Pediatric diagnosis and treatment | Indicator | |
| Pediatric diagnosis and treatment – Pediatric diagnosis | Sub-indicator | |
| Pediatric diagnosis and treatment – Pediatric treatment | Sub-indicator | |
| Migrants’ access to health care | Indicator | |
| Migrants’ access to health care – Primary health care | Sub-indicator | |
| Migrants’ access to health care – HIV health care | Sub-indicator | |
| Tuberculosis diagnostics | Indicator | |
| Testing and prevention | Self-testing | Indicator |
| Partner notification/Index testing | Indicator | |
| Partner notification/Index testing – Index testing | Sub-indicator | |
| Partner notification/Index testing – Confidentiality in index testing | Sub-indicator | |
| Compulsory testing | Indicator | |
| Age restrictions on testing and treatment | Indicator | |
| PrEP | Indicator | |
| PrEP – Policy | Sub-indicator | |
| PrEP – Regulatory approval | Sub-indicator | |
| Harm reduction | Indicator | |
| Harm reduction – Harm reduction strategy | Sub-indicator | |
| Harm reduction – Syringe non-criminalization | Sub-indicator | |
| Comprehensive sexuality education | Indicator | |
| Prisoner prevention | Indicator | |
| Prisoner prevention – Condoms | Sub-indicator | |
| Prisoner prevention – Needle and syringe exchange program | Sub-indicator | |
| Health systems | Task shifting | Indicator |
| Health financing | Indicator | |
| Health financing – Budget | Sub-indicator | |
| Health financing – Tax revenue | Sub-indicator | |
| Universal health coverage | Indicator | |
| Universal health coverage – ARVs | Sub-indicator | |
| Universal health coverage – PrEP | Sub-indicator | |
| User fees | Indicator | |
| User fees – Primary care | Sub-indicator | |
| User fees – HIV services | Sub-indicator | |
| Access to medicines (TRIPS) | Indicator | |
| Access to medicines (TRIPS) – Incorporation | Sub-indicator | |
| Access to medicines (TRIPS) – Use | Sub-indicator | |
| Unique identifiers with data protections | Indicator | |
| Unique identifiers with data protections – Unique identifiers use | Sub-indicator | |
| Unique identifiers with data protections – Data protections | Sub-indicator | |
| Data sharing | Indicator | |
| Data sharing – Disaggregation | Sub-indicator | |
| Data sharing - Frequency | Sub-indicator | |
| Structural | Same-sex sex non-criminalization | Indicator |
| Same-sex sex non-criminalization – Laws | Sub-indicator | |
| Same-sex sex non-criminalization – Arrests | Sub-indicator | |
| Sex work non-criminalization | Indicator | |
| Drug use non-criminalization | Indicator | |
| HIV exposure non-criminalization | Indicator | |
| HIV exposure non-criminalization – Laws | Sub-indicator | |
| HIV exposure non-criminalization – Arrests | Sub-indicator | |
| Non-discrimination protections | Indicator | |
| Non-discrimination protections – Sexual orientation | Sub-indicator | |
| Non-discrimination protections – Gender identity | Sub-indicator | |
| Non-discrimination protections – HIV status | Sub-indicator | |
| National human rights institutions | Indicator | |
| Constitutional right to health | Indicator | |
| Girls’ education | Indicator | |
| Civil society | Indicator | |
| Civil society – Social contracting | Sub-indicator | |
| Civil society - Freedom | Sub-indicator | |
| NOTE: Please see the HIV Policy Lab codebook for indicator and sub-indicator definitions. | ||
Endnotes
- For more information on PEPFAR, see KFF’s The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) fact sheet. ↩︎
- U.S. Department of State, PEPFAR 2021 Country and Regional Operational Plan (COP/ROP) Guidance for All PEPFAR Countries, updated February 2021, accessed: https://www.state.gov/wp-content/uploads/2021/02/PEPFAR-COP21-Guidance-Final.pdf. ↩︎
- U.S. Department of State, PEPFAR 2021 Annual Report to Congress, February 2021, accessed: https://www.state.gov/wp-content/uploads/2021/02/PEPFAR2021AnnualReporttoCongress.pdf. ↩︎
- U.S. Department of State, Strategy for Accelerating HIV/AIDS Epidemic Control (2017-2020), September 2017, accessed: https://www.state.gov/wp-content/uploads/2019/08/PEPFAR-Strategy-for-Accelerating-HIVAIDS-Epidemic-Control-2017-2020.pdf. ↩︎
- U.S. Department of State, PEPFAR 2021 Country and Regional Operational Plan (COP/ROP) Guidance for All PEPFAR Countries, updated February 2021, accessed: https://www.state.gov/wp-content/uploads/2021/02/PEPFAR-COP21-Guidance-Final.pdf. ↩︎
- U.S. Department of State, PEPFAR 2021 Annual Report to Congress, February 2021, accessed: https://www.state.gov/wp-content/uploads/2021/02/PEPFAR2021AnnualReporttoCongress.pdf. ↩︎
- Specific examples of normative, evidence-based guidance and policies developed by international bodies include the WHO’s Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach (see: https://www.who.int/publications/i/item/9789240031593) and Key Considerations for Differentiated ART Delivery for Specific Populations jointly produced by the WHO, U.S. Centers for Disease Control and Prevention, PEPFAR, USAID, and the International AIDS Society (see: https://www.who.int/publications/i/item/WHO-HIV-2017.34), among others. All guidelines and policies that the HIV Policy Lab uses as benchmarks with which to assess countries are included in their codebook (see: https://hivpolicylab.org/codebook). ↩︎
- PEPFAR is administered through the Office of the U.S. Global AIDS Coordinator and Health Diplomacy within the U.S. Department of State, led by a Senate-confirmed coordinator with the rank of ambassador, and is housed within U.S. diplomatic missions under the oversight of the U.S. ambassador in country. ↩︎
- For more information on differentiated service delivery, see https://www.differentiatedservicedelivery.org/. ↩︎
- U.S. Department of State, PEPFAR 2021 Country and Regional Operational Plan (COP/ROP) Guidance for All PEPFAR Countries, updated February 2021, accessed: https://www.state.gov/wp-content/uploads/2021/02/PEPFAR-COP21-Guidance-Final.pdf. ↩︎
- U.S. Department of State, PEPFAR 2021 Annual Report to Congress, February 2021, accessed: https://www.state.gov/wp-content/uploads/2021/02/PEPFAR2021AnnualReporttoCongress.pdf. ↩︎
- U.S. Department of State, U.S. Embassy and Consulate in Nigeria. “U.S. Urges Removal of User-fees for People Living with HIV,” October 2019, accessed: https://ng.usembassy.gov/u-s-urges-removal-of-user-fees-for-people-living-with-hiv/. ↩︎
- Ahonkhai AA, et al. “The impact of user fees on uptake of HIV services and adherence to HIV treatment: Findings from a large HIV program in Nigeria,” PLOS ONE, September 2020, accessed: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0238720. ↩︎
- USAID, “Sustainable Financing: Controlling the HIV/AIDS Epidemic Through Shared Responsibility,” webpage, accessed: https://www.usaid.gov/global-health/health-areas/hiv-and-aids/technical-areas/sustainable-financing-initiative (August 5, 2021). ↩︎
- U.S. Department of State, Strategy for Accelerating HIV/AIDS Epidemic Control (2017-2020), September 2017, accessed: https://www.state.gov/wp-content/uploads/2019/08/PEPFAR-Strategy-for-Accelerating-HIVAIDS-Epidemic-Control-2017-2020.pdf. ↩︎
- U.S. Department of State, PEPFAR 2021 Country and Regional Operational Plan (COP/ROP) Guidance for All PEPFAR Countries, updated February 2021, accessed: https://www.state.gov/wp-content/uploads/2021/02/PEPFAR-COP21-Guidance-Final.pdf. ↩︎
- U.S. Department of State, “Statement from Ambassador Deborah Birx, M.D., U.S. Global AIDS Coordinator, on the Principles of PEPFAR's Public Health Approach,” April 2014, accessed: https://web.archive.org/web/20150905071637/http:/www.pepfar.gov/press/releases/2014/224738.htm. ↩︎
- U.S. Department of State, Draft PEPFAR COP 2022 Guidance. ↩︎
- Institute of Medicine, Evaluation of PEPFAR, February 2013, accessed: https://www.nap.edu/catalog/18256/evaluation-of-pepfar. ↩︎
- O’Neill Institute for National and Global Health Law at Georgetown University Law Center, Reorganization and the Future of PEPFAR; Implications of State and USAID Reform, 2018. ↩︎
- Kolker J. “A Diplomat’s Perspective on Use of Science and Evidence in Implementing PEPFAR,” Science and Diplomacy, April 2018, accessed: https://www.sciencediplomacy.org/article/2018/kolker-pepfar. ↩︎
- Daschle T, Frist B, Building Prosperity, Stability, and Security Through Strategic Health Diplomacy: A Study of 15 Years of PEPFAR, Bipartisan Policy Center, 2018, accessed: https://bipartisanpolicy.org/wp-content/uploads/2019/03/Building-Prosperity-Stability-and-Security-Through-Strategic-Health-Diplomacy-A-Study-of-15-Years-of-PEPFAR.pdf. ↩︎
- Collins C et al, “Four Principles for Expanding PEPFAR’s Role as a Vital Force in U.S. Health Diplomacy Abroad,” Health Affairs, July 2012, accessed: https://www.healthaffairs.org/doi/10.1377/hlthaff.2012.0204. ↩︎
- Daschle T, Frist B, The Case for Strategic Health Diplomacy: A Study of PEPFAR, 2015, Bipartisan Policy Center, November 2015, accessed: https://bipartisanpolicy.org/wp-content/uploads/2019/03/BPC_Strategic-Health-November-2015.pdf. ↩︎
- The COP/ROP documents serve as annual strategic plans for U.S. HIV/AIDS efforts in host countries, as well as serve as the basis for the approval of U.S. funding. Each COP focuses on PEPFAR’s efforts in one county in most cases, whereas the ROPs focus on a group of countries. Most, but not all, COP countries receive a greater level of investment than ROP countries. ↩︎
- PEPFAR’s 2020 Country Operational Plan Guidance for all PEPFAR Countries includes a list of 55 countries that were required to submit a COP or ROP that year. This list served as the basis for our “PEPFAR countries” group. Two countries on this list (Barbados and Suriname) were excluded from our analysis following communication with staff in the Office of the Global AIDS Coordinator that confirmed that direct bilateral support had been discontinued to those countries in recent years. ↩︎
- U.S. Department of State, PEPFAR 2021 Country and Regional Operational Plan (COP/ROP) Guidance for All PEPFAR Countries, updated February 2021, accessed: https://www.state.gov/wp-content/uploads/2021/02/PEPFAR-COP21-Guidance-Final.pdf. ↩︎
- According to the U.S. government database www.foreignassistance.gov, three countries that were not required to develop a COP or ROP received some HIV funding in FY 2020 – Colombia, Peru, and Venezuela. These countries were not included in the PEPFAR group. ↩︎
- Only low- and middle-income countries, as defined by the World Bank (https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups) were included in this analysis, with the exception of two high-income countries (Panama and Trinidad and Tobago) that receive PEPFAR support and were required to submit a ROP in 2020. ↩︎
- U.S. Department of State, “PEPFAR Update – Stakeholder Townhall,” presentation delivered on August 2, 2012. ↩︎
- O’Neill Institute for National and Global Health Law at Georgetown University Law Center, HIV Policy Lab, accessed: https://hivpolicylab.org/. ↩︎
- Kavanagh M, et al, “Understanding and comparing HIV-related law and policy environments: cross-national data and accountability for the global AIDS response,” BMJ Global Health, 2020, accessed: https://gh.bmj.com/content/5/9/e003695. ↩︎
- UNAIDS, Laws and Policies Analytics, web platform, accessed: http://lawsandpolicies.unaids.org/. ↩︎
- PEPFAR’s 2020 Country Operational Plan Guidance for all PEPFAR Countries includes a list of 55 countries that were required to submit a COP or ROP that year. This list served as the basis for our “PEPFAR countries” group. Two countries on this list (Barbados and Suriname) were excluded from our analysis following communication with staff in the Office of the Global AIDS Coordinator that confirmed that direct bilateral support had been discontinued to those countries in recent years. ↩︎
- According to the U.S. government database www.foreignassistance.gov, three countries that were not required to develop a COP or ROP received some HIV funding in FY 2020 – Colombia, Peru, and Venezuela. These countries were not included in the PEPFAR group. ↩︎
- Only low- and middle-income countries, as defined by the World Bank (see: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups), were included in this analysis, with the exception of two high-income countries (Panama and Trinidad and Tobago) that receive PEPFAR support and were required to submit a ROP in 2020. ↩︎