Medicare Part B Drugs: Cost Implications for Beneficiaries in Traditional Medicare and Medicare Advantage
In the face of rising prescription drug costs, a large majority of the public supports federal efforts to lower drug spending. In his 2022 State of the Union address, President Biden urged Congress to pass legislation to rein in drug costs. In November 2021, the House of Representatives passed the Build Back Better Act (BBBA), which includes several provisions that would lower prescription drug costs, but the Senate has yet to take action on this legislation. Proposals included in the BBBA would allow the federal government to negotiate the price of some drugs covered under Medicare Part B (drugs administered by physicians and other health care providers) and Part D (retail prescription drugs); require drug companies to pay rebates to the federal government when annual increases in drug prices for Medicare and private insurance exceed the rate of inflation; cap monthly insulin costs for people with Medicare and private insurance; and cap Medicare beneficiaries’ out-of-pocket drug spending under Part D (but not Part B).
To better understand the potential out-of-pocket cost exposure that Medicare beneficiaries may face for Part B drugs, in this brief we analyze cost-sharing liability for these drugs in traditional Medicare and cost-sharing requirements in Medicare Advantage plans. Data limitations preclude us from analyzing actual out-of-pocket costs paid by beneficiaries who used Part B drugs. For traditional Medicare beneficiaries, claims data do not report separately cost-sharing liability paid directly by beneficiaries versus supplemental insurance (where applicable). For Medicare Advantage enrollees, there are no data available on actual out-of-pocket costs paid for Part B drugs.
Beneficiaries in traditional Medicare are charged 20% of the cost of Part B drugs, with no annual limit on their out-of-pocket costs. Beneficiaries enrolled in Medicare Advantage plans – which account for a growing share of the Medicare population and currently cover close to half of all beneficiaries – also typically face cost-sharing requirements for Part B drugs up to their plan’s out-of-pocket limit ($7,550 for in-network cost sharing and $11,300 for in-network and out-of-network cost sharing combined in 2022). Most but not all beneficiaries in traditional Medicare have some form of supplemental coverage to help with their Medicare cost-sharing requirements, while most Medicare Advantage enrollees do not. For example, most traditional beneficiaries who have Medigap have a policy that covers the 20% coinsurance for Part B drugs and services, while Medicaid and some of the Medicare Savings Programs cover Medicare cost sharing for eligible low-income beneficiaries in both traditional Medicare and Medicare Advantage. But even those with supplemental insurance may face some out-of-pocket costs for their Part B drugs, depending on the generosity of their coverage. In addition, roughly 6 million Medicare beneficiaries have no supplemental coverage and would be responsible for the full 20% coinsurance.
In the first part of this analysis, we examine Medicare claims data for 2019 to assess cost-sharing liability for Part B drugs for beneficiaries in traditional Medicare (excluding Part B vaccines since these are provided at no cost to Medicare beneficiaries). In the second part of our analysis, we use Medicare Advantage benefit design data for 2022 to examine the range in cost-sharing amounts at or below 20% coinsurance charged by Medicare Advantage plans for in-network Part B drugs. We also analyze variation in cost-sharing amounts for out-of-network Part B drugs charged by plans that provide out-of-network coverage. (See Methods for additional details on both parts of our analysis.)
Findings
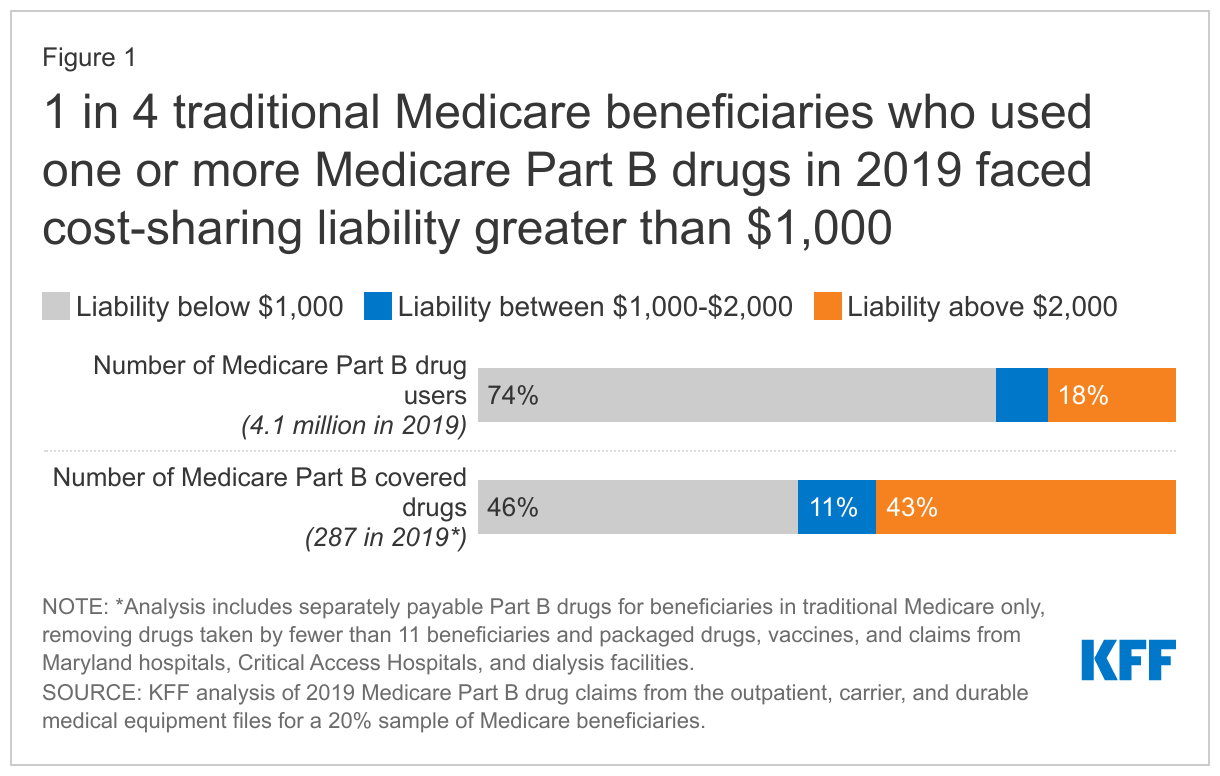
One-fourth of the 4.1 million traditional Medicare beneficiaries who used one or more Part B drugs in 2019 had average annual cost-sharing liability of at least $1,000
Of the 4.1 million beneficiaries in traditional Medicare who received one or more Medicare Part B drugs included in this analysis, 1 in 4 (1.0 million beneficiaries) faced cost-sharing liability of at least $1,000 and nearly 1 in 5 (0.7 million) faced cost-sharing liability of at least $2,000 in 2019 (Figure 1). About 0.4 million traditional Medicare beneficiaries – or 1 in 10 of those who used Part B drugs – had at least $5,000 in cost-sharing liability for these drugs in 2019. As previously noted, we are unable to analyze how many beneficiaries had supplemental insurance to cover some or all of these costs and how many were responsible for paying the full amount out-of-pocket.
For more than half of all Part B drugs included in this analysis, average annual cost-sharing liability was $1,000 or more in 2019
Of the 287 Part B drugs included in this analysis, more than half (54% or 155 drugs) had average annual cost-sharing liability of at least $1,000 in 2019, and more than 4 in 10 (43% or 123 drugs) had cost-sharing liability of at least $2,000.
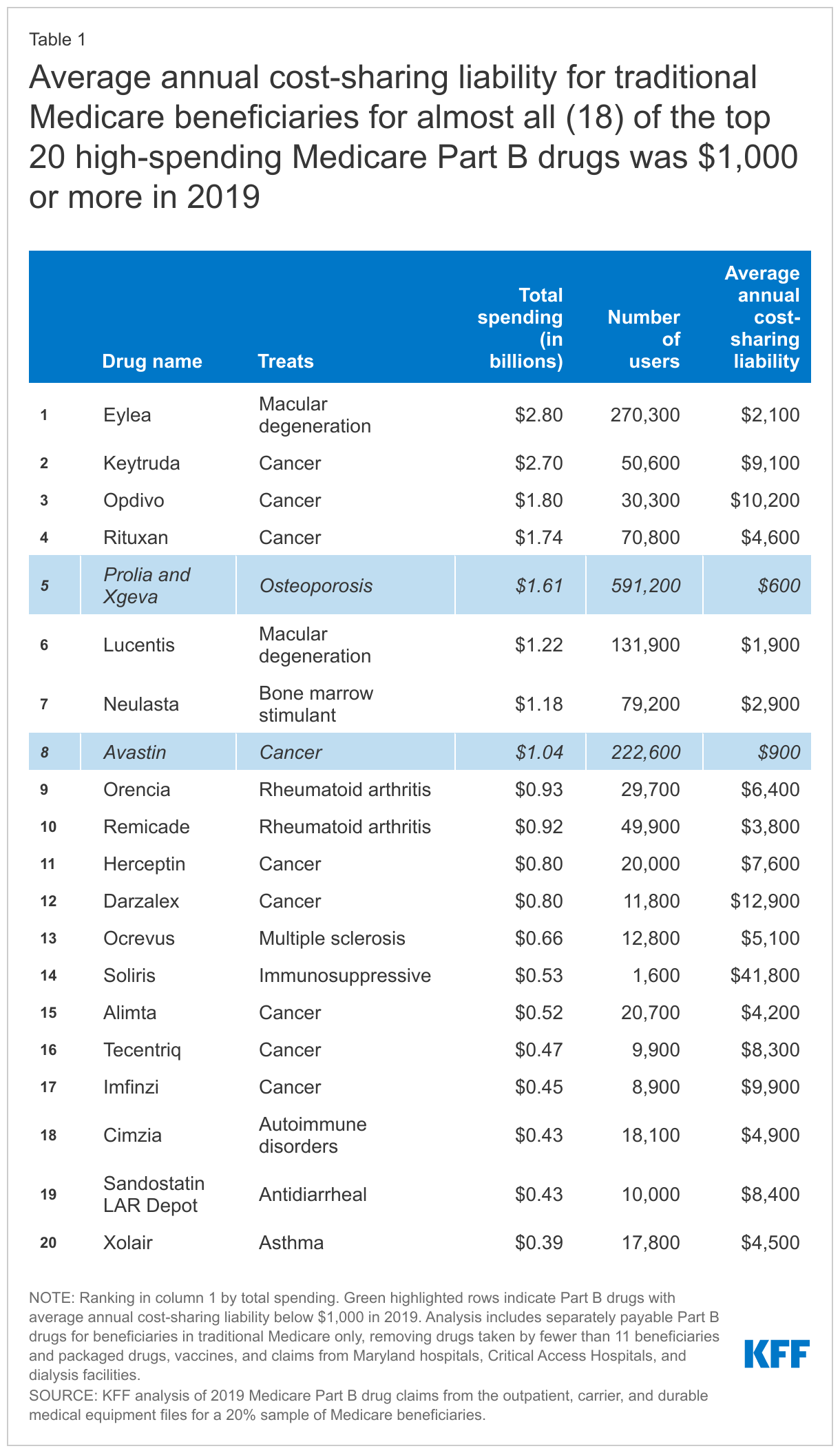
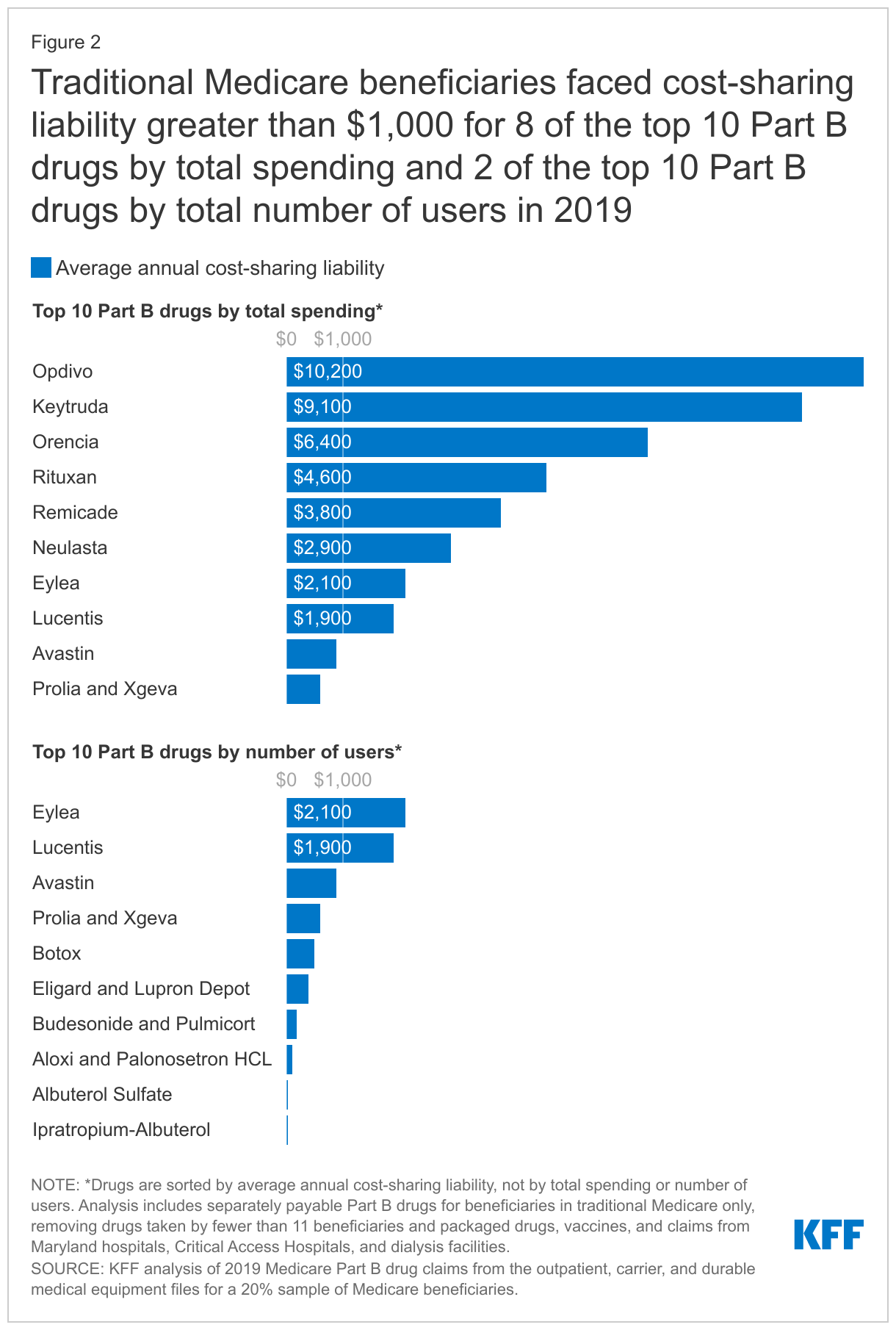
- Eight of the top 10 Part B drugs with the highest total spending, and 18 of the top 20, had average annual cost-sharing liability of at least $1,000 in 2019 (Figure 2, Table 1). For example, average beneficiary liability for Eylea, the top-spending Part B drug in 2019 used by 270,300 traditional Medicare beneficiaries to treat macular degeneration, was $2,100. For the cancer drug Keytruda, second in terms of total Medicare Part B spending, average cost-sharing liability was $9,100.
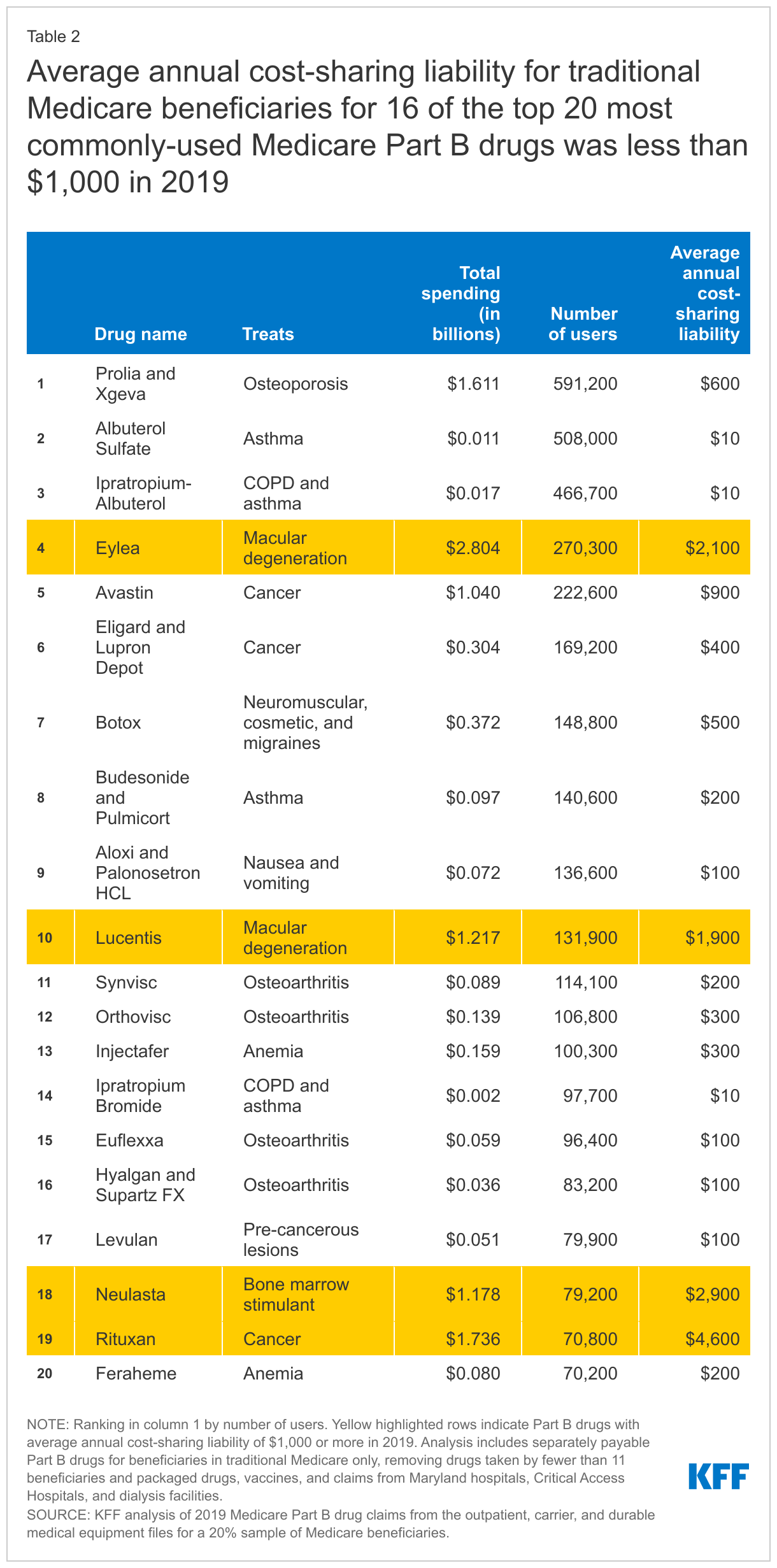
- Conversely, average annual cost-sharing liability for most of the Part B drugs with the highest number of users was below $1,000. Only 2 of the top 10 Part B drugs based on the number of users, and 4 of the top 20, had average annual cost-sharing liability of at least $1,000 in 2019 (Table 2). For example, average beneficiary liability for the most-commonly used (non-vaccine) Part B drug, Prolia (and the equivalent brand Xgeva), an osteoporosis treatment used by nearly 600,000 traditional Medicare beneficiaries in 2019, was $600.
Average annual cost-sharing liability exceeded $10,000 for more than 1 in 10 Part B drugs in this analysis (13% or 36 drugs). While some of the highest-liability drugs were used by relatively few beneficiaries to treat rare conditions, two of these drugs were used by more than 10,000 beneficiaries in 2019: Opdivo, a treatment for several types of cancer used by 30,300 beneficiaries, with average annual cost-sharing liability of $10,200; and Darzalex, a treatment for multiple myeloma used by nearly 12,000 beneficiaries, with average annual cost-sharing liability of $12,900.
Like beneficiaries in traditional Medicare, Medicare Advantage enrollees typically face 20% coinsurance for Part B drugs, but can be exposed to higher cost-sharing requirements for these drugs when administered by an out-of-network provider
Medicare Advantage plans have flexibility to determine cost-sharing amounts for Part B covered drugs, subject to certain limits, and can differentiate cost sharing for chemotherapy from other Part B drugs. In 2022, Medicare Advantage plans are prohibited from charging more than 20% coinsurance, or the equivalent copay amount, for both chemotherapy and other Part B drugs from in-network providers. There are no similar restrictions on out-of-network cost-sharing amounts.
Based on our analysis of Medicare Advantage plan cost-sharing requirements and enrollment as of January 2022:
- Consistent with current requirements, all 22.9 million Medicare Advantage enrollees included in this analysis (excluding enrollees in employer group plans) face coinsurance of 20% or less (or equivalent cost sharing) for chemotherapy and other Part B drugs when provided in-network (Figure 3). Some Medicare Advantage plans always charge less than 20% coinsurance for both types of drugs; for example, 25% of HMO enrollees and 9% of PPO enrollees and other plans that offer out-of-network coverage charge less than 20% coinsurance for Part B drugs administered in network. Other plans vary cost-sharing amounts for Part B drugs (e.g., a $0 copayment or 20% coinsurance) depending on the type of drug (e.g., chemotherapy vs. other Part B drugs) and/or where it is furnished (e.g., a pharmacy or other provider setting).
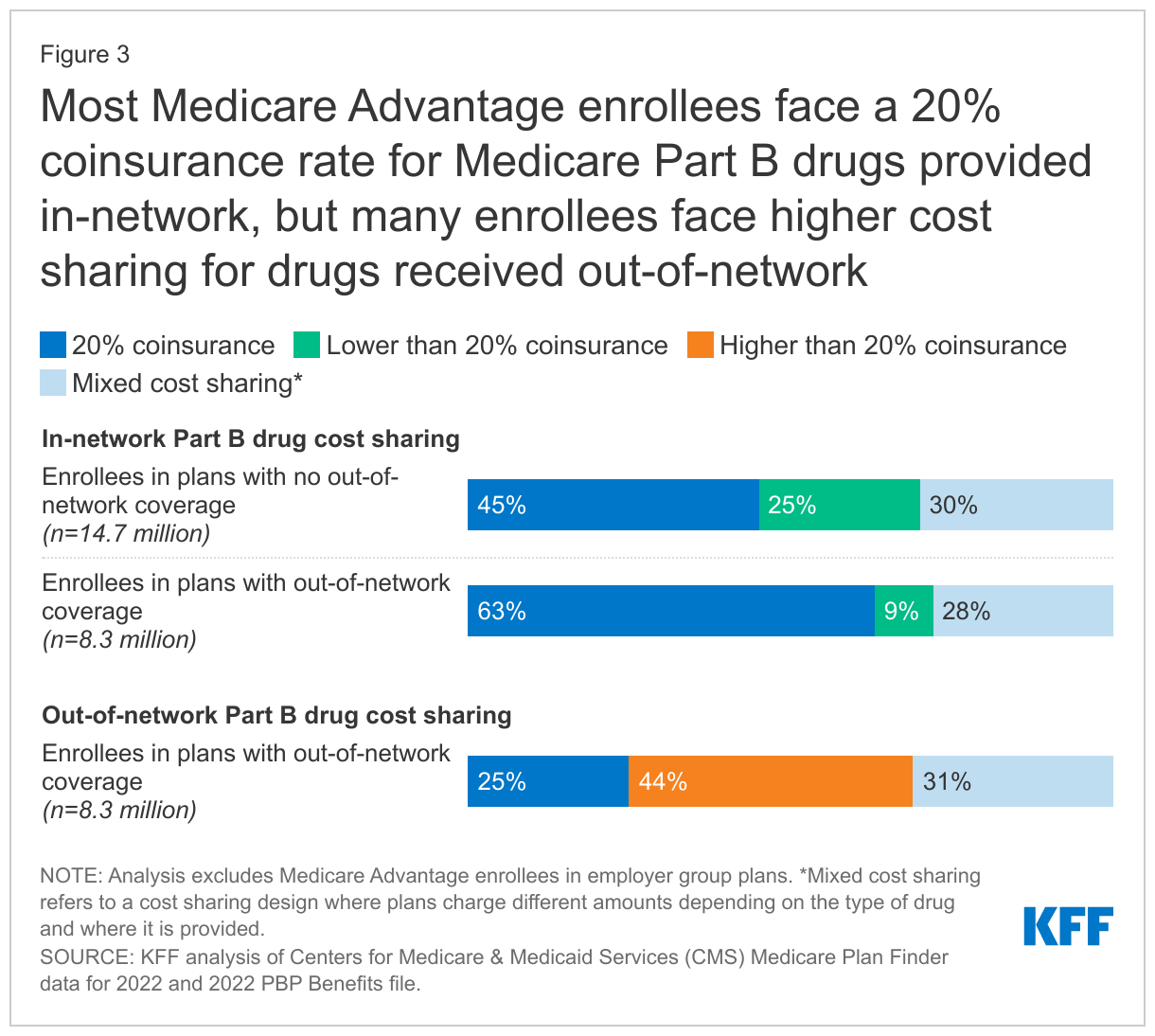
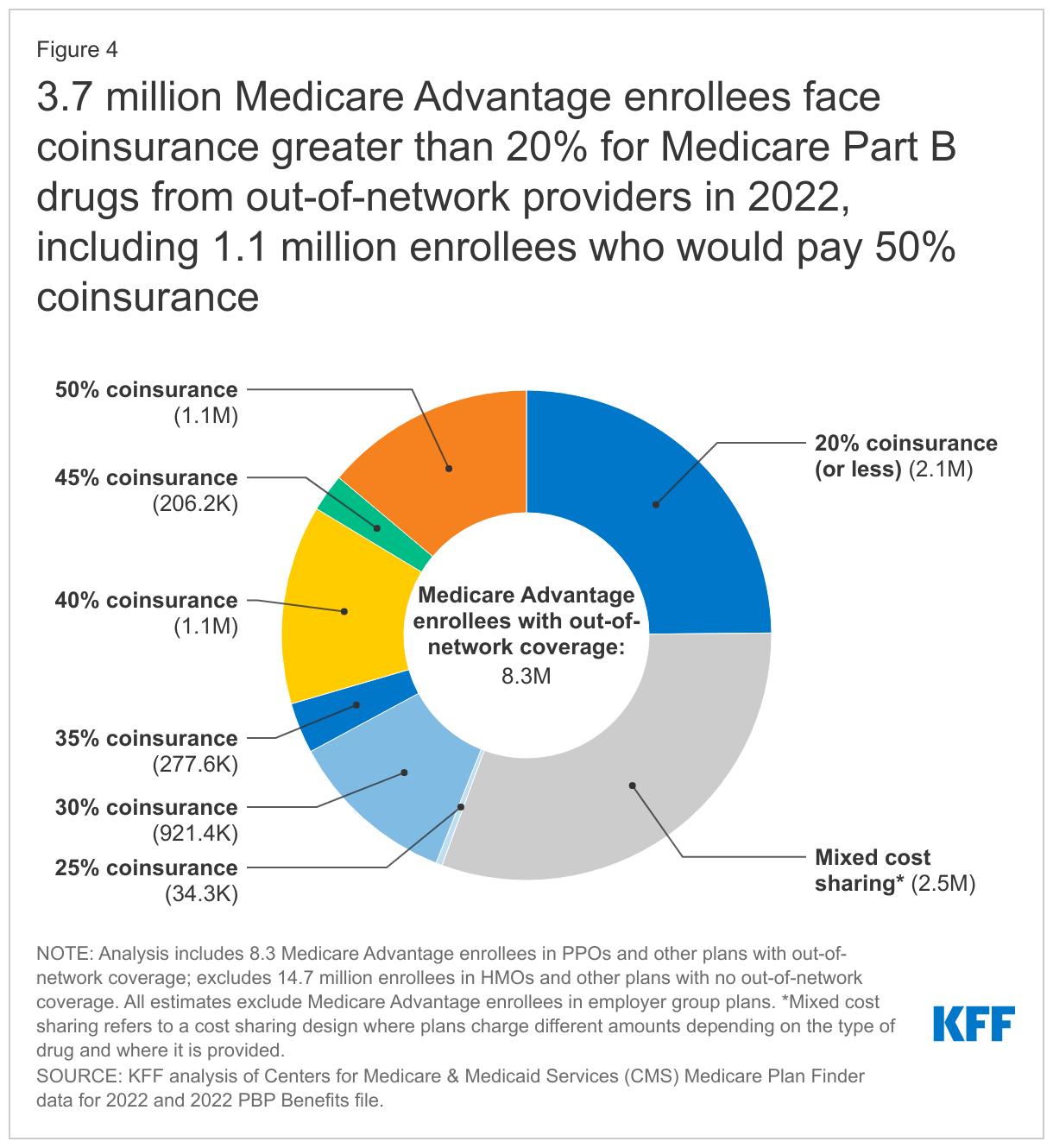
- Among the 8.3 million Medicare Advantage enrollees in PPOs and other types of plans with out-of-network coverage, one-fourth of these enrollees (2.1 million) face 20% coinsurance for Part B drugs received from an out-of-network provider, while close to half (44% or 3.7 million) would be charged more than 20% for these drugs if administered by an out-of-network provider (Figure 4). Among these enrollees, 1.1 million are in plans that charge 50% for out-of-network Part B drugs, 1.1 million are in plans that charge 40% coinsurance, and 0.9 million enrollees are in plans that charge a 30% coinsurance (0.9 million). Another 31% of enrollees with out-of-network coverage (2.5 million) may face coinsurance higher than 20% depending on the type of drug and/or where the drug is administered.
- The 14.7 million Medicare Advantage enrollees in HMOs and other plans with no out-of-network coverage would pay 100% of the cost for Part B drugs administered out-of-network unless they received prior approval from their plan.
Unlike traditional Medicare, Medicare Advantage plans have an out-of-pocket limit, but Medicare Advantage enrollees can still face substantial cost-sharing amounts for some of the higher-priced Part B drugs, especially if administered out-of-network.
- For Eylea, a treatment for macular degeneration, Medicare Advantage enrollees would face average cost-sharing liability of $2,100 at a 20% coinsurance rate and up to $5,200 at a 50% coinsurance rate, assuming the plan pays the same price as traditional Medicare.
- For Rituxan, a cancer and autoimmune treatment, Medicare Advantage enrollees would face average cost-sharing liability of $4,600, based on a 20% coinsurance rate for in-network chemotherapy, but could face costs up to their plan’s maximum out-of-limit for this one drug alone based on higher out-of-network coinsurance rates (up to $11,300 in 2022).
- For Prolia (and the equivalent brand Xgeva), an osteoporosis treatment, Medicare Advantage enrollees would face average cost-sharing liability of $600 at a 20% coinsurance rate and up to $1,400 at a 50% coinsurance rate, assuming the plan pays the same price for these drugs as traditional Medicare.
Discussion
Beneficiaries in both traditional Medicare and Medicare Advantage can be exposed to potentially high out-of-pocket costs for Part B drugs – though data limitations preclude us from analyzing out-of-pocket costs paid directly by beneficiaries who used Part B drugs in either traditional Medicare or Medicare Advantage plans and the share of costs covered by private supplemental insurance or Medicaid. We find that, overall, 1 in 4 beneficiaries in traditional Medicare who used Part B drugs in 2019 faced cost-sharing liability of at least $1,000, and more than half of Part B drugs included in this analysis had average cost-sharing liability of $1,000 or more. Given the absence of an out-of-pocket limit for beneficiaries in traditional Medicare, the costs of chemotherapy and other Part B drugs could represent a substantial financial burden for beneficiaries with no supplemental coverage, or with supplemental coverage that does not cover all cost-sharing requirements for these drugs.
While Medicare Advantage plans are required to have a maximum out-of-pocket limit and can charge no more than 20% for Part B drugs administered by an in-network provider, most Medicare Advantage enrollees would face higher costs for Part B drugs furnished by an out-of-network provider, including close to 4 million enrollees in plans with out-of-network coverage and nearly 15 million enrollees in HMOs and other plans with no out-of-network coverage. Plans with out-of-network coverage typically charge higher cost sharing for Part B drugs and other services received out-of-network to encourage enrollees to receive care from in-network providers where plans have negotiated lower prices. These network arrangements and cost-sharing differences can have potentially large cost implications for Medicare beneficiaries.
Among the set of proposals that policymakers have recently considered to lower prescription drug costs, allowing the federal government to negotiate prices for some drugs covered under Part B and Part D and requiring inflation rebates for Medicare-covered drugs to limit annual increases in drug prices could help to address the spending burden that Medicare beneficiaries could face if they need high-cost drugs, whether covered under Part B or Part D.
This work was supported in part by Arnold Ventures. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
This analysis is based on 2019 Medicare claims data for separately payable (non-packaged) Part B drugs from a 20% sample of Medicare beneficiaries, removing drugs taken by fewer than 11 beneficiaries in the sample. The claims include beneficiaries in traditional Medicare only, excluding beneficiaries enrolled in Medicare Advantage. Using HCPCS codes for Part B drugs, claims were pulled from the outpatient, carrier, and durable medical equipment (DME) files, removing packaged drugs, vaccines, and claims from Maryland hospitals, Critical Access Hospitals, and dialysis facilities.
We calculate beneficiary liability using variables in the claims data corresponding to deductible and coinsurance amounts, but we are not able to determine the amount that a beneficiary actually paid. Beneficiaries may not be responsible for some or all of their cost-sharing liability if they have certain types of supplemental coverage, including most Medigap policies or full benefits through Medicaid.
Medicare Advantage cost-sharing amounts and plan designs are based on the Centers for Medicare & Medicaid Services (CMS) Medicare Plan Finder data for 2022 and 2022 PBP Benefits file. Enrollment numbers are from the CMS January 2022 enrollment files. Plan-county enrollment and plan totals were removed if fewer than 11 beneficiaries were enrolled. Additionally, all employer plans were removed from the analysis as they are not required to submit all the data necessary for this analysis. We also excluded all Medicare-Medicaid plans.
For out-of-network Part B drugs in PPOs, data limitations preclude us from assessing differences in out-of-network cost-sharing amounts for chemotherapy and other Part B drugs because the Medicare Plan Finder does not separate out-of-network cost sharing for these two categories. It is likely that the percentage of enrollees we report as having a mixed cost-sharing structure for out-of-network Part B drugs would be lower if the data allowed us to analyze out-of-network cost sharing separately for chemotherapy and other Part B drugs. For an analogous approach, we estimated combined in-network cost-sharing amounts based on the amounts for chemotherapy and other Part B drugs. If these cost-sharing amounts were analyzed separately, the percentage of enrollees paying 20% coinsurance would be higher for chemotherapy, with a lower percentage of enrollees exposed to a mixed cost-sharing design. The percentages for the separate category of other Part B drugs would be similar to the percentages we report for both chemotherapy and other Part B drugs combined.
Tables