State Actions to Address Nursing Home Staffing During COVID-19
Issue Brief
Key Takeaways
While staffing shortages in nursing homes have existed for decades, the COVID-19 pandemic has highlighted and intensified the need for sufficient, consistent, trained staff to care for residents. Numerous studies have found that high staffing levels are associated with higher care quality. Yet, a recent report concluded that “staffing standards in almost every state remain severely low.” In April 2022, the National Academies of Science, Engineering, and Medicine recommended minimum staffing levels, policies to ensure competitive wages and benefits, and improvements to staff training and opportunities for career advancement, among other reforms, as part of its comprehensive report to improve nursing home quality. The Biden Administration has announced plans to propose new federal minimum staffing adequacy regulations in the next year.
This issue brief summarizes federal and state standards related to nursing home staffing prior to COVID-19 and builds on existing information by identifying changes to state minimum staffing requirements adopted since the onset of the COVID-19 pandemic. We also examine state legislative and regulatory actions since the onset of the pandemic that directly affect worker wages and training requirements. Key findings include the following:
Staffing Requirements: At least five states (AR, CT, MA, NY, RI) adopted permanent increases to nursing home minimum staffing requirements after the onset of the COVID-19 pandemic, while at least one state (GA) adopted a permanent decrease. At least two states (OR, SC) adopted temporary decreases to account for potential staffing issues during the pandemic.
Wages: At least four states (CO, IL, MA, NC) adopted laws or regulations that require increases to nursing home staff wages since the onset of the COVID-19 pandemic. At least three states (MI, NC, OH) adopted temporary increases or one-time bonuses to nursing home staff wages post-COVID. Other states may have adopted or proposed Medicaid provider reimbursement rate changes that do not explicitly require corresponding increases in direct care staff wages.
Training: At least 3 states (KY, MO, WI) adopted permanent changes to staff training requirements post-COVID to expand the pool of staff available to work in nursing homes, while at least 8 states (AK, CT, DE, IA, IN, KS, MO, WI) adopted temporary changes in this area.
Over the next year, policy action is expected on the federal level related to nursing home staffing. Following up on the White House announcement of a package of nursing home reforms, the Centers for Medicare and Medicaid Services (CMS) recently released a request for information to inform its planned development of a federal minimum staffing requirement for nursing homes. While Congress could adopt legislative changes, it is currently unclear whether the nursing home provisions that were included in the Build Back Better legislation that passed the House would be included in a potential budget reconciliation package that could be considered this summer. As passed by the House in November 2021, the Build Back Better provisions would have directed the HHS Secretary to study and report to Congress and propose regulations on any appropriate minimum federal nursing staff to resident ratios. The legislation also would have replaced the current federal requirement for a registered nurse for at least eight consecutive hours per day, 7 days per week, with a new requirement for a registered nurse 24 hours a day. Finally, both federal and state policymakers will likely be considering the recommendations in the National Academies’ comprehensive report on improving nursing home care quality.
Introduction
While staffing shortages in nursing homes have existed for decades, the COVID-19 pandemic has highlighted and intensified the need for sufficient, consistent, trained staff to care for residents. As of March 27, 2022, more than one in four nursing homes nationally reported a shortage of at least one type of staff, though the share of nursing homes reporting staffing shortages varies widely by state. As of March 20, 2022, nursing homes were most likely to report a shortage of aides, followed by nursing staff, and least likely to report a shortage of clinical staff. The pandemic has taken a substantial toll on people living and working in nursing homes. Over 200,000 residents and staff in long-term care facilities have died from COVID-19, comprising more than one in five of all COVID-19 deaths in the U.S.1 Most of these deaths (about 155,000) have occurred in nursing homes that are certified to participate in the Medicare and/or Medicaid programs.2
Numerous studies over several decades have found that high staffing levels are associated with higher care quality for nursing home residents. A December 2021 study reviewed state nursing home staffing standards and concluded that “staffing standards in almost every state remain severely low.” The Medicaid and CHIP Payment and Access Commission (MACPAC) recently reviewed state policies that can help address staffing issues, including increasing Medicaid payment rates, changing Medicaid payment methods to incentivize facilities to devote more revenue to staff, and requiring minimum staffing levels above the federal standard. In April 2022, the National Academies of Science, Engineering and Medicine recommended minimum staffing levels, policies to ensure competitive wages and benefits, and improvements to staff training and opportunities for career advancement, among other reforms, as part of its comprehensive report to improve nursing home quality.
The Biden Administration recently announced plans to propose new federal minimum staffing adequacy regulations in the next year. States can choose to adopt staffing or training requirements that are stricter than federal rules as part of their role in licensing nursing home providers and administering state Medicaid programs, which finance the majority of nursing home care. Nursing home staff shortages and high turnover rates among staff are largely attributed to low wages. While Medicare and Medicaid reimbursement rates to nursing homes can indirectly influence worker wages, states also can adopt policies to require or incentivize providers to raise wages paid to direct care workers.
This issue brief summarizes federal and state standards related to nursing home staffing prior to COVID-19 and builds on existing information by identifying changes to state minimum staffing requirements adopted since the onset of the COVID-19 pandemic. We also examine state legislative and regulatory actions since the onset of the pandemic that directly affect worker wages (other than increases to provider reimbursement rates), and training requirements. Detailed state-level information is included in the Appendix Tables. While we reviewed legislation and regulations in all 50 states and DC, this brief may not capture all relevant policy changes.
What were federal and state staffing requirements pre-COVID?
Federal regulations require nursing homes to provide licensed nursing services 24 hours a day, with a registered nurse on staff for at least eight consecutive hours a day, seven days a week. This equates to 0.30 staffing hours per resident day (hprd).3 Facilities also must designate a full-time registered nurse as a full-time director of nursing. Additionally, the federal regulations include a qualitative standard, which requires nursing homes to provide “sufficient nursing staff … to maintain the highest practicable physical, mental, and psychosocial well-being of each resident.” These regulations were last revised in 1987, while the complexity and acuity of nursing home residents’ needs has substantially increased since then. Federal law authorizes the Health and Human Services (HHS) Secretary to establish requirements relating to nursing home residents’ health, safety and well-being as conditions for facilities to receive payment from the Medicare and Medicaid programs.
A 2001 CMS study recommended a minimum of 4.1 nursing hours per resident per day to prevent harm to residents. However, there has never been a federally required minimum number of staffing hours per resident day, despite repeated calls to establish one from researchers and patient advocates over the last several decades. Additionally, a series of Institute of Medicine reports have recommended that nursing home staff include registered nurses 24 hours a day. The April 2022 National Academies report recommends direct-care registered nurse coverage 24 hours a day, with additional registered nurse “coverage that reflects resident census, acuity, case mix” and residents’ professional nursing needs as determined by their assessments and care plans.
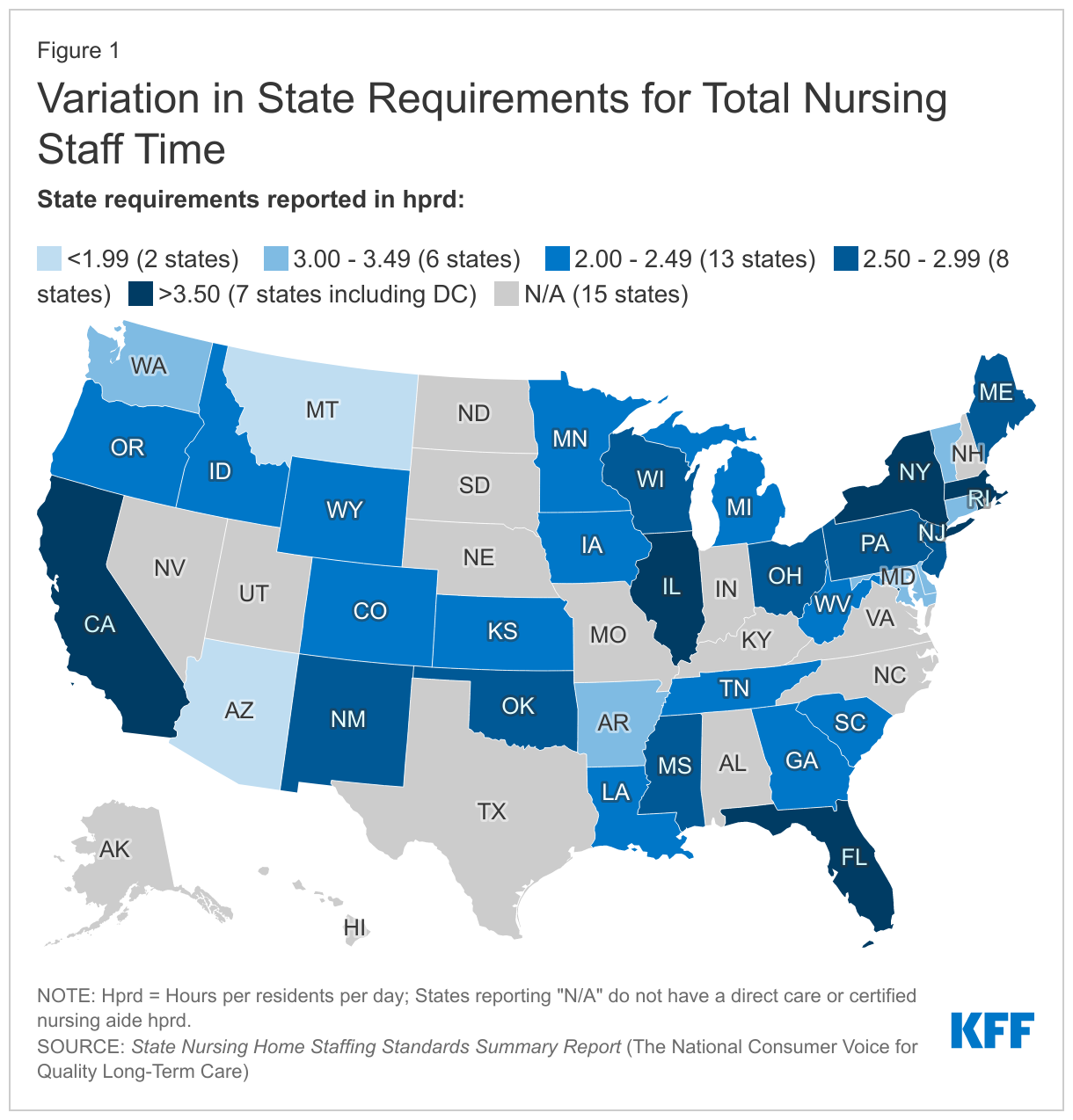
There is substantial variation in state minimum staffing requirements (Figure 1). Compared to the federal minimum of 0.30 hprd, three states have standards below this level, three states adopt the federal minimum, and 45 states have standards above the federal minimum. As of December 2021, only the District of Columbia met or exceeded the minimum of 4.1 hprd recommended to prevent harm to residents. Some states explicitly require a minimum number of staff hours per resident day, while other states call for nursing homes to provide direct care staff 24 hours per day, seven days per week, without an explicit number of hours per resident requirement.
Federal regulations require nursing aides to complete a 75-hour training program and to pass a competency evaluation in order to work in a nursing home longer than four months. Nursing aides (also called nursing assistants) provide the majority of direct care in nursing homes. In response to the COVID-19 public health emergency, CMS temporarily waived the training requirement as a means of addressing potential staffing shortages during the pandemic. However, CMS recently announced that this waiver will sunset on June 6, 2022, citing concerns about care quality. CMS has advised states to reevaluate their training programs and consider allowing some of the time worked by nursing aides during the public health emergency to count toward the 75-hour training requirement after the waiver ends.
How have state staffing requirements changed since COVID-19?
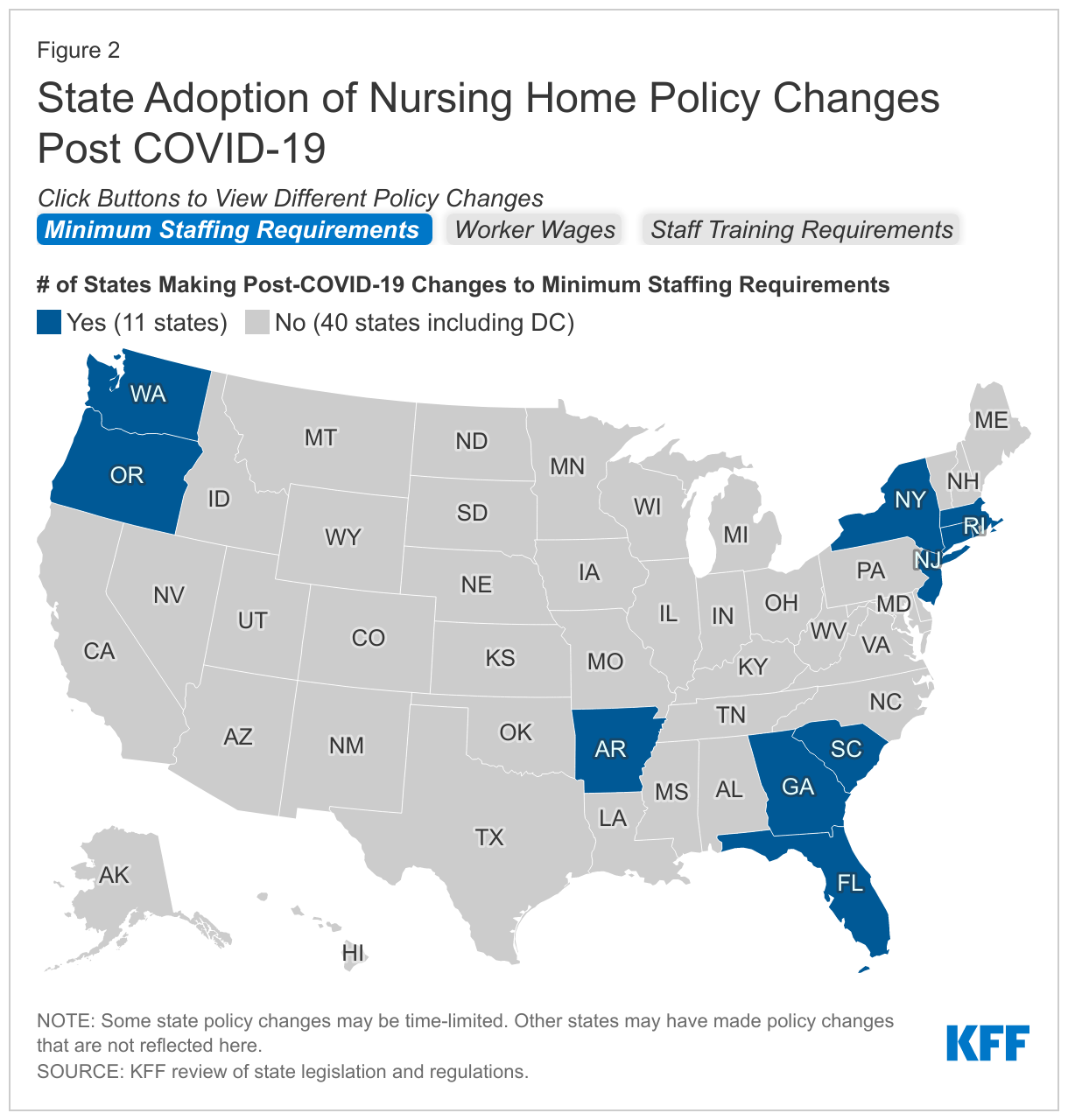
This brief examines state legislative and regulatory actions since the onset of the pandemic to address nursing home staffing, including minimum staffing requirements, policies that directly affect worker wages (other than increases to provider reimbursement rates), and training requirements. We include both permanent and temporary changes to illustrate the types of action states are taking. While we reviewed legislation and regulations in all 50 states and DC, this brief may not capture all relevant policy changes. Figure 2 summarizes state activity post-COVID in the areas of minimum staffing requirements, worker wages, and training requirements. Detailed state-level information is included in the Appendix Tables.
State Changes to Minimum Staffing Requirements
At least five states adopted permanent increases to nursing home minimum staffing requirements after the onset of the COVID-19 pandemic, while at least one state adopted a permanent decrease (Figure 2 and Appendix Table 1). Among the states that adopted increases, the amount ranged from an additional 0.16 hprd in Connecticut to an additional 3.78 hprd in Rhode Island. Other states adopting increases include Arkansas, Massachusetts, and New York. Arkansas also adopted a broader definition of the direct care staff whose hours count toward its new minimum staffing requirement, while Rhode Island no longer allows director of nursing hours to count toward its new minimum staffing requirement. By contrast, Georgia permanently decreased its minimum staffing requirement by 0.24 hprd. All of the states adopting permanent minimum staffing changes post-COVID, including Georgia with its decrease, continue to exceed the federal minimum staffing requirement of 0.30 hours per resident day.
Two states, Florida and New Jersey, retained their total daily minimum staffing hours but restructured how those hours are allocated across staffing types or shifts post-COVID (Appendix Table 1). Specifically, Florida retained its total hprd but increased the number of licensed practical nurse hours and decreased the number of certified nursing assistant hours that count toward the overall total. Florida also amended its definition of direct care staff whose hours can count toward the minimum hprd to include personal care attendants. New Jersey retained its total hprd but now divides the daily minimum to set specific hprd requirements during each of the three shifts in a day.
At least two states adopted temporary decreases to minimum staffing requirements post-COVID to account for potential staffing issues during the pandemic (Appendix Table 1). These states include Oregon and South Carolina. Oregon also authorized facilities to utilize personal care assistants, nursing assistants, physical therapists, and occupational therapists to meet no more than 25 percent of the certified nursing assistant minimum staffing requirement during this time. Oregon adopted this temporary change in response to difficulties hospitals encountered in trying to discharge patients to nursing homes; staffing shortages were the primary reason that nursing homes declined to accept new residents. Although South Carolina’s state agency did not explicitly describe the reasons for the temporary change, South Carolina hospitals are experiencing similar difficulty discharging patients to nursing homes due to staffing shortages. Oregon and South Carolina’s temporary decreases still result in state minimum staffing requirements that exceed the federal minimum level of 0.30 hprd.
Legislation that would have permanently increased minimum staffing requirements post-COVID was proposed but failed to pass in at least two states. Arizona introduced HB 2848 on February 11, 2021, which would have increased its minimum staffing requirement. However, the bill was voted down in the House Rules Committee four days later. Kentucky introduced House Bill 215 on January 8, 2020, which would have increased its minimum staffing requirement. The bill was voted down two days later in the House Health and Family Services Committee. The Kentucky bill was unpopular among nursing home industry representatives, which characterized it as “overregulation” and alleged that it would encourage excessive litigation. Nursing home administrators also opposed the bill due to an increasing statewide staffing shortage, which was exacerbated by the pandemic.
State Changes to Worker Wages
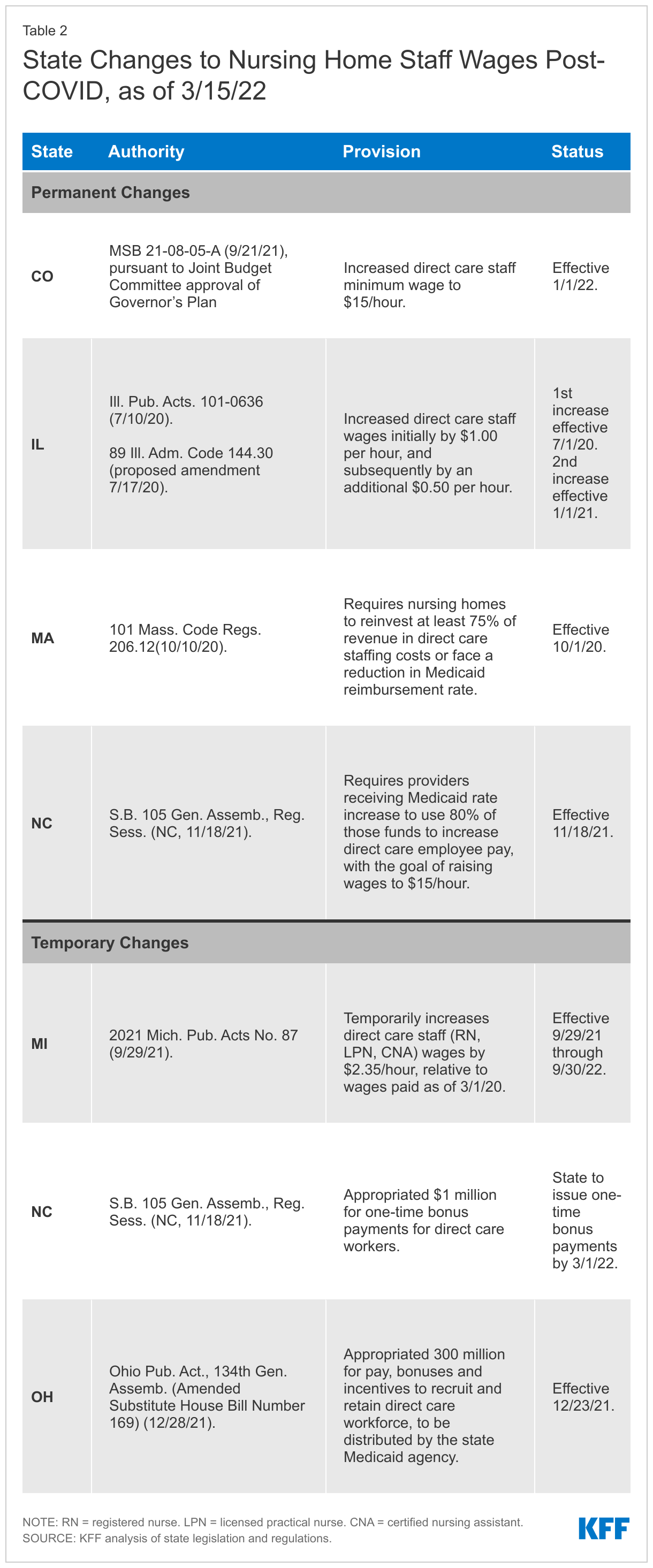
At least four states adopted laws or regulations that require increases to nursing home staff wages since the onset of the COVID-19 pandemic (Figure 2 and Appendix Table 2). One of these states, Colorado, passed legislation that established a $15.00 per hour minimum wage for nursing home direct care staff as of January 2022. At least three other states (IL, MA, and NC) adopted changes that require nursing homes to increase staff wages as a condition of receiving increased Medicaid provider reimbursement rates. Illinois specified that nursing homes must increase direct care staff wages by $1.00 per hour as of July 2020, and an additional 50 cents per hour as of January 2021. Massachusetts and North Carolina both direct nursing homes to devote a certain share of the rate increase to direct care staff wages (75% and 80%, respectively). A goal of North Carolina’s legislation is to raise staff wages to $15.00 per hour; prior to the increase, wages averaged $10.30 per hour. Other states may have adopted or proposed Medicaid provider reimbursement rate changes that do not explicitly require corresponding increases in direct care staff wages.
At least three states adopted temporary wage increases or one-time bonuses for nursing home staff post-COVID. These changes apply to all staff and are not limited to providers that participate in Medicaid. Michigan enacted a temporary one year increase of $2.35 per hour for direct care staff, including nurses and aides. Without the increase, starting wages for aides averaged $11.00 to $12.00 per hour. North Carolina’s legislature appropriated $1 million for one-time bonus payments to direct care staff, while Ohio’s legislature appropriated $300 million for wages, incentives, and bonuses to recruit and retain direct care staff.
State Changes to Staff Training Requirements
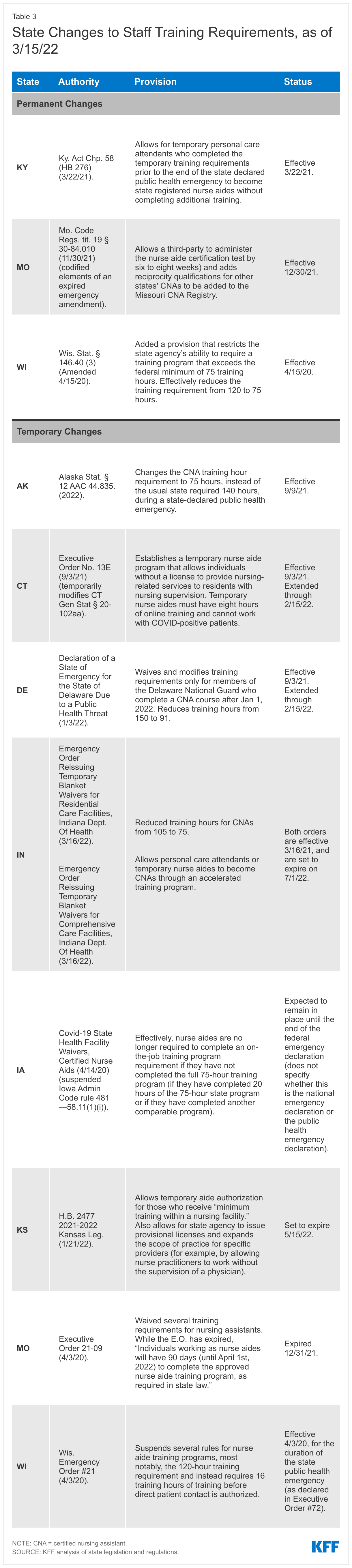
At least three states adopted permanent changes to staff training requirements to expand the pool of staff available to work in nursing homes post-COVID (Figure 2 and Appendix Table 3). One of these states, Wisconsin, lowered the training hour requirement for nurse aides from 120 hours to the federal minimum of 75 hours. Additionally, Missouri now allows third parties to administer the certification test for nursing assistants, which is expected to expedite the process by six to eight weeks. Missouri also established reciprocity standards to allow out-of-state certified nursing assistants (CNAs) to work in Missouri. Also, Kentucky adopted changes that allow for personal care attendants that finished training during the state-declared public health emergency to become state registered nurse aides. Once the state-declared public health emergency ends, these nurse aides are not required to complete additional training.
At least eight states adopted temporary changes to staff training requirements post-COVID to expand the pool of staff available to work in nursing homes (Appendix Table 3). Four of these states (AK, DE, IN, and WI) lowered the training hour requirements for CNAs during the pandemic, in efforts to address staffing issues. Alaska’s temporary reduction applies during any state-declared public health emergency, not just during the COVID public health emergency. Missouri waived its training requirements, and Iowa temporarily suspended an additional on-the-job training requirement for CNAs. Connecticut and Kansas adopted changes that allow temporary nurse aides to work, though Connecticut’s temporary executive order has expired.
Looking Ahead
Over the next year, policy action is expected on the federal level related to nursing home staffing. Following up on the White House announcement of a package of nursing home reforms, CMS recently released a request for information to inform its planned development of a federal minimum staffing requirement for nursing homes. Responses are due on June 10, 2022. CMS also plans to conduct a research study, noting that resident acuity has increased in recent years, and to issue proposed regulations within one year.
In addition to administrative agency action, Congress could adopt legislative changes, though it is currently unclear whether the nursing home provisions that were included in the Build Back Better legislation would be included in another budget reconciliation package that is possible this summer. As passed by the House in November 2021, the Build Back Better provisions would have directed the HHS Secretary to study and report to Congress and propose regulations on any appropriate minimum federal nursing staff to resident ratios. The legislation also would have replaced the current federal requirement for a registered nurse for at least eight consecutive hours per day, 7 days per week, with a new requirement for a registered nurse 24 hours a day.
Finally, both federal and state policymakers will likely be considering the recommendations in the National Academies’ comprehensive report on improving nursing home care quality. Specifically, that report notes the need to improve worker wages, benefits, training, and working conditions as an integral part of improving nursing home resident health and quality of life.
KFF appreciates the contributions of Emma Childress, law/master of health administration student at St. Louis University, and Belle Harris, law student at Georgetown University, who worked as contractors on this project. We also are grateful for the dedicated work of Meghana Ammula, KFF research assistant.
Appendix

Endnotes
- KFF analysis of CDC COVID data tracker, CMS COVID-19 Nursing Home data, and state-reported deaths in long-term care facilities (week ending April 17, 2022). ↩︎
- Id. ↩︎
- Expressed numerically for a 100-bed facility, the federal standard equates to 0.30 staffing hours per resident day (hprd), including a full-time director of nursing (0.06 hprd), a registered nurse for 8 consecutive hours per day (0.08 hprd), and a registered nurse or licensed nurse during the other two shifts (0.16 hprd). The National Consumer Voice for Quality Long-Term Care report provides a detailed explanation of this calculation for purposes of comparing standardized federal and state staffing requirements. ↩︎