Potential Impact of the Federal Pause on Immigrant Visas From 75 Countries on the U.S. Health Care Workforce
As part of broader efforts to reduce immigration, the U.S. Department of State (DOS) recently announced that it will pause issuance of all immigrant visas for individuals from 75 countries. This analysis shows that workers from 69 of the 75 countries affected by the pause for which data are available make up nearly one in ten (8%) of the U.S. health care workforce. The pause will likely reduce the supply of workers and particularly health care workers in the U.S., which could exacerbate existing health care worker shortages. Shortages are likely to be compounded by other policies limiting immigration into the U.S. as well as ongoing deportation efforts. Estimates suggest the Trump administration’s policies could reduce legal immigration to the U.S. by 33% to 50% over four years.
On January 14, 2026, the DOS announced that it will pause processing of immigrant visas for individuals from 75 countries who it identified as at, “high risk for use of public benefits” and becoming a public charge. (See Methods for full list of impacted countries). This policy is part of broader efforts to expand public charge policies.The DOS indicates that the pause is being implemented to ensure “immigrants must be financially self-sufficient and not be a financial burden to Americans”. However, the DOS has not provided details about the process used to identify countries subject to the pause. Moreover, few immigrants are eligible for federal benefits due to longstanding restrictions. For example, most lawfully present immigrants have to wait five years after obtaining a “qualified” immigration status to be eligible for federal programs including Medicaid and the Supplemental Nutrition Assistance Program (SNAP).
The pause went into effect on January 21, 2026, for nationals from the 75 countries applying for immigrant visas. Immigrant visas allow an individual to live and work in the U.S. on a permanent basis and can provide a pathway to citizenship. Examples of immigrant visas include family-based visas (when a U.S. citizen or lawful permanent resident (LPR or “green card” holder) sponsors a family member for permanent residency), certain types of employment-based visas, as well as refugee visas (although entry of refugees to the U.S. has already largely been eliminated through executive action). Individuals applying for non-immigrant visas such as a student visa, tourist visa, or temporary work visa like H-1B are not impacted by the pause. The DOS states that, during this pause, applicants from impacted countries may submit visa applications and attend visa interviews, but that it will not issue any immigrant visas. The pause does not impact immigrants from the 75 countries who are already present in the U.S.
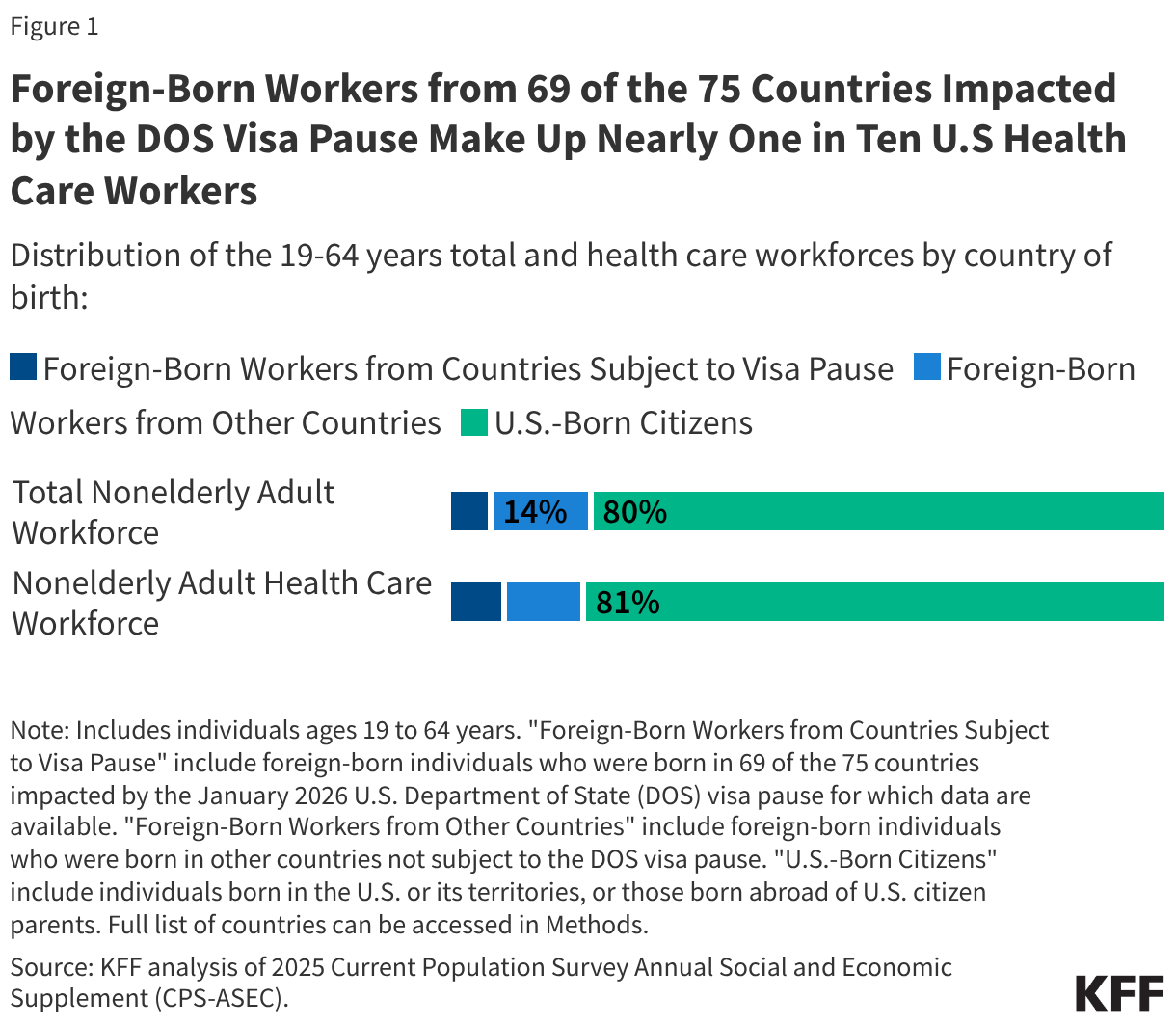
Foreign-born workers from 69 of the 75 countries impacted by the DOS visa pause for which data are available make up nearly one in ten (8%) of health care workers in the U.S. Based on KFF analysis of 2025 Current Population Survey data, there were 7.8 million foreign-born workers (ages 19 to 64) from 69 of the 75 countries impacted by the visa pause as of 2025, including 1.2 million health care workers. A little over half (55%) of health care workers from these countries are employed in health care support occupations such as home health aides and nursing aides, and the remaining 45% are in health care practitioner and technical occupations such as physicians, surgeons, and nurses. These workers include individuals who may have arrived on immigrant or non-immigrant visas since the data do not include information on visa type. Separate data for the remaining six countries affected by the pause (The Gambia, Kosovo, Kyrgyz Republic, Rwanda, South Sudan, and Tunisia) were not available. Among foreign-born workers from the 69 countries, those from Haiti (13%), Jamaica (10%), and Nigeria (9%) made up about one in three (32%), or the highest shares, of health care workers. Workers from 69 of the 75 countries affected by the DOS visa pause accounted for 6% of the total U.S. adult workforce and 8% of health care workers under age 65 (Figure 1). Immigrants from other countries not impacted by the pause accounted for 14% of the U.S. adult workforce and 11% of health care workers, and U.S.-born citizens accounted for the remaining eight in ten workers.
Methods
Data source: These findings are based on KFF analysis of the 2025 Current Population Survey Annual Social and Economic Supplement (CPS-ASEC). The CPS is a nationally representative U.S. household survey sponsored jointly by the U.S. Census Bureau and the U.S. Bureau of Labor Statistics and is the “primary source of labor force statistics for the population of the United States”.
Identifying foreign-born workers from impacted countries in CPS-ASEC: Foreign-born workers are identified as those between ages 19 and 64 who report their citizenship group as either “foreign born, US cit by naturalization” or “foreign born, not a US citizen”. Those who further indicate their country of birth as being one of the 75 countries impacted by the DOS visa pause (listed below) are included in the sample of foreign-born workers from countries subject to the visa pause. Of note, CPS does not include country of birth data separately for 6 of the 75 countries impacted by the DOS visa pause, namely The Gambia, Kosovo, Kyrgyz Republic (Kyrgyztan), Rwanda, South Sudan, and Tunisia.
List of impacted countries: Afghanistan, Albania, Algeria, Antigua and Barbuda, Armenia, Azerbaijan, Bahamas, Bangladesh, Barbados, Belarus, Belize, Bhutan, Bosnia and Herzegovina, Brazil, Burma, Cambodia, Cameroon, Cape Verde, Colombia, Cote d’Ivoire, Cuba, Democratic Republic of the Congo, Dominica, Egypt, Eritrea, Ethiopia, Fiji, The Gambia, Georgia, Ghana, Grenada, Guatemala, Guinea, Haiti, Iran, Iraq, Jamaica, Jordan, Kazakhstan, Kosovo, Kuwait, Kyrgyz Republic, Laos, Lebanon, Liberia, Libya, Moldova, Mongolia, Montenegro, Morocco, Nepal, Nicaragua, Nigeria, North Macedonia, Pakistan, Republic of the Congo, Russia, Rwanda, Saint Kitts and Nevis, Saint Lucia, Saint Vincent and the Grenadines, Senegal, Sierra Leone, Somalia, South Sudan, Sudan, Syria, Tanzania, Thailand, Togo, Tunisia, Uganda, Uruguay, Uzbekistan, and Yemen(Source: DOS).
Identifying health care workers in CPS-ASEC: Health care workers are identified as those whose detailed occupation in CPS-ASEC is reported as either “healthcare practitioner and technical occupations” or “healthcare support occupations”.