Untold KFF History Volume 1: South Africa
Everyone who knows KFF today thinks of us as the independent source of health policy analysis, polling, and in-depth news coverage. As we head to a leadership transition next year from me to Larry Levitt and Molly Brodie, I plan to write about some of the other things we have done over the years that are part of our history and the soul of the organization, but may not be remembered by our current audiences. Our decades long commitment to South Africa is the place to start.
We made a huge commitment to South Africa at the time when divestiture of investments in the country during apartheid was the main international response. We decided to get directly and heavily involved instead, helping South Africa prepare for and then build a democracy and a health system for the whole population. We trained leaders, built institutions, and supported a free press. Later, when HIV hit there and the post-Mandela government wouldn’t deal with it, we developed the largest HIV prevention program in the world called loveLife, aimed at mobilizing teens and young adults (where most new infections were) to prevent HIV. Even today, we still feel the opportunity costs of undertaking such a big effort financially, but we believed everything we had done previously in South Africa was at risk if the epidemic there was not checked. The greatest privilege of my life was to be able to work with Nelson Mandela, and I sometimes wonder what he would make of today’s state of affairs here and in South Africa.
Because we got involved when others left, we came to play an outsized role there that at times made me somewhat uncomfortable and certainly had to be handled dutifully. Then, we were still called the Kaiser Family Foundation, and Mandela pronounced it “Ky-eezer”. His words when he would greet me still come back to me: “Ah Drew, the Kyeezer Foundation. You are everywhere”. Ambulances in rural areas – the “independent homelands” black South Africans were banished to – sometimes bore our name, with various spellings, because they felt patients they transported to overwhelmed hospitals would be more likely to get treated if the ambulance had our name on it. (I was never certain that was true.)
A great deal of the credit goes to the head of our South Africa program, a South African named Dr. Michael Sinclair. Possibly the most mission-driven person I have known, Michael relentlessly organized our strategies and programs on the ground with the credibility with Mandela and his oldest allies of an anti-apartheid activist and the cunning of an experienced MI6 operative. An outstanding speaker, Michael would stand in the back of the room and not say much, but almost every word spoken by the highest-level leaders from South Africa and around the world, every bit of choreography, and the outcome of important meetings had been arranged painstakingly over months of negotiation facilitated by him (the way foreign policy used to be practiced).
The main goal of our South Africa program was to develop the people, plans and programs to help establish a successful democracy and a more equitable health system. We called it the Program for Health and Development in South Africa, signaling that our purposes were broader than health care. In the early years that meant building the institutions and leaders South Africa would need after apartheid fell, including primary care systems in rural areas that the black population had been banished to, advocacy organizations (South Africa’s only national advocacy organization, which gave rise to several future leaders), research organizations such as the Health Systems Trust, and much more. It meant acting as a go between, sometimes sitting in meetings with Fredrik DeKlerk blowing unfiltered cigarette smoke in our faces to broker deals with funders, or the African National Congress (ANC), or its rival then the Inkhata Freedom Party headed by a conservative Zulu leader named Mangosuthu Buthelezi who brought a food taster to our meetings.
In the early years, government security followed us everywhere we went. It led to one of my favorite moments. Michael Sinclair, and two senior board members, former Congresswoman Barbara Jordan and former HHS Secretary Joe Califano, and I were asked to meet with a top general in the South African armed forces. The meeting took place in a hotel. After explaining their position on their nuclear weapons they had developed and eventually destroyed so as to not incinerate their country along with the ANC and its allies, and covering other territory distasteful to the general, he abruptly said, “Look, I want you to know that I don’t like what you people are doing in my country, and I am prepared to give my life to stop the blacks from taking over our country.” Barbara, the great orator, sitting in her wheelchair, had not said a word in the meeting. She answered, “Well sir, we may just need to take you up on that kind offer,” and wheeled from the room, ending the meeting. It’s a little piece of Barbara Jordan history now recorded here.
Later, after Mandela was released from prison, our role shifted. We helped to train parliamentary committees and a free press and establish professional health journalism there and a nonprofit news organization long before we did so at KFF itself. One example, Health-E News, continues to operate today.
We wanted to raise the profile of health on the agenda, and so did Mandela, which we did partly by establishing the Mandela Award for Health and Human Rights, at Mandela’s request, as well as an award for global health journalism with CNN International.
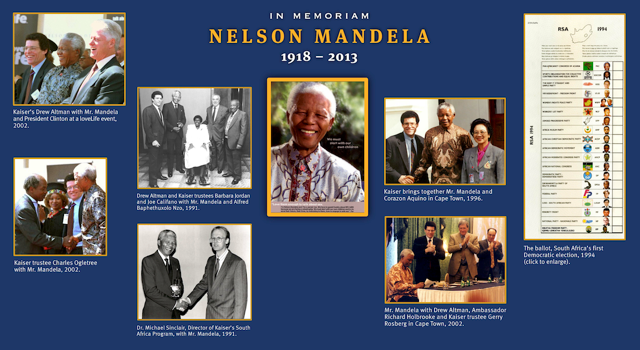
Through our polling program we conducted a survey in many languages about how the South African people were feeling about their new democracy, one of our now 37 joint survey projects with the Washington Post. We held retreats for the new South African leadership in the Philippines and in Mexico to plan their health system and at Mandela’s request brought Philippines President Corazon Aquino to South Africa.
As the toll mounted, leaders from all over the globe implored South Africa’s second democratically elected president Thabo Mbeki to do more about its raging HIV epidemic, feeling South Africa uniquely could lead Africa’s response. His response was tepid at best, some believe because he saw mounting Western criticism as an affront to African men. His Minister of Health, Mantu Tshabala- Msmang, a high ranking woman in the ANC who had actually come up through one of our regional programs, the Progressive Primary Care Network, and with whom we had a good working relationship, was ineffective and scorned worldwide for pushing alternative treatments such as beet root and garlic. We tried to step into the vacuum with loveLife.
We launched the program in September 1999, working with a consortium of leading South African organizations and more than 100 community-based organizations, the South African government, major South African media groups, including the South Africa Broadcasting Corporation (SABC), and private foundations. loveLife combined a highly visible and sustained national multi-media HIV education and awareness campaign with countrywide adolescent-friendly service development in government clinics, and a national network of outreach and support programs for youth. We set it up as an independent non-profit organization governed by its own board so it could eventually be folded into the operations of a friendlier government.
It was a massive undertaking and included:
- A big and hard hitting national multi-media campaign Including television, radio, outdoor media, print and music – educating young people about HIV and promoting dialogue about sexual health issues. loveLife messages were everywhere in South Africa. Developed by young people, they were “out there” and highly controversial, but they broke through. loveLife still exists in an evolved and smaller form, and its messaging remains powerful.
- A National Adolescent-Friendly Clinic Initiative, a major drive to establish adolescent health services in South Africa’s 5,000 public clinics.
- A national network of 16 multi-purpose youth facilities, known as “Y-Centers.” These were large regional centers providing recreation and skills training, as well as sexual health education and medical care in non-clinical settings. Many included community radio stations broadcasting programming about HIV. As the architect of New Jersey’s school-based services programs when I was in charge of human services there, I have never seen anything as impressive as the Y Centers.
- A countrywide program of community-level outreach and support to young people (including 3,500 schools) led by a revolving national volunteer corps of more than 1,500 young adults each year, known as loveLife Groundbreakers, with a corps of Groundbreakers in training called Impinchis, creating a steady stream of thousands of youth leaders. Many become future leaders in communities and in the country.
- Grandmothers organized in rural villages and urban communities the South Africans called Granny Gogogetters. (Gogo is a term of endearment.)
- A nationally accessible toll-free telephone helpline for young people providing sexual health information, counselling and referrals averaging 300,000 calls per month.
- The loveLife Games, the largest school sports competition in South Africa, promoting healthy living, self-motivation and personal achievement to more than 400,000 school students annually.
- There were even two big trains decked out in loveLife purple crossing the country with the messaging stopping for events.

At its height, loveLife and our other South Africa programs represented more than a quarter of our annual spending, with big contributions from European partners and the South African government. It was a non-traditional program, focusing on youth and community empowerment and mobilization, led by young people. For this reason, and its “out there” media campaign, it was anything but the darling of the mainstream HIV response organizations such as the Global Fund. Their perspective was understandable to me. Sure, it distributed millions of condoms, but it was not a by-the-book prevention program or solely focused on HIV. The South Africans felt the deeper and more insidious impact of apartheid on young people and communities also had to be addressed to counter HIV there by giving teens and young adults hope and agency, and by dealing with tough underlying issues fueling the epidemic such as older men infecting young women and girls. To do that, the South Africans felt the program had to break through in entirely new and uniquely South African ways. Evaluations were very positive, but South Africa continues to have a very significant HIV epidemic although now also a more fulsome government response. When HIV drugs came along treatment became integral to prevention and that also changed the thrust of prevention efforts worldwide.
It may be that the lasting benefits of loveLife have been more on leadership development and demonstrating how the country can mobilize, with a little help, when government falls short. In a private discussion we have not previously disclosed, Mandela sadly acknowledged to us that he felt he had failed on HIV, largely because it required dealing with issues of sexuality that he was not comfortable with (he had a lot on his plate!). One of the great heroes of the HIV prevention effort was loveLife’s first Executive Director Dr David Harrison. He went on to head a leading South African foundation, the DG Murray Trust . Michael Sinclair also went on to great further success at Harvard leading a Ministerial Leadership Program for health and finance ministers from across the globe he developed there.
In 2008 when the Great recession hit, it hit us too. We were operating programs all over the world that we no longer could sustain. We transitioned out of our global operations and our South Africa program, focusing exclusively on the role you see us playing today, domestic health policy, which we have considered our core business from the start. We called it our “narrower but deeper” strategy. In retrospect, the roughly $100 million of our own funds we put into loveLife (matched more than three to one by others) on top of our already substantial South Africa spending meant fewer resources for our core U.S. work if instead those funds had remained in our endowment generating our usual investment return. We might instead have operated more surgically in South Africa. It’s also fair to say that, by 2008, South Africa had opened up and faced new challenges, including inside the ANC. While we could still be helpful, we could no longer play the special role we had played early on. It’s always hard for organizations to stop doing things they value deeply, but there is a time for it and we did. Even so, there is nothing we have done I am more proud of. As one of our trustees, Michael Sovern. former President of Columbia University, said at the time, “how could we not do everything we can” (even if it eroded assets). And the work inspired other big initiatives, the Global Media AIDS Initiative, and our Social Impact Media Program in the U.S. that we operated until very recently, which garnered seven Emmy and two Peabody awards for targeted, cutting edge domestic HIV campaigns. Those and other past KFF programs will be the subject of future columns over the next six months.
