The Trump Administration Moves Forward with Medicare Site-Neutral Payment Reform
Published: November 24, 2025
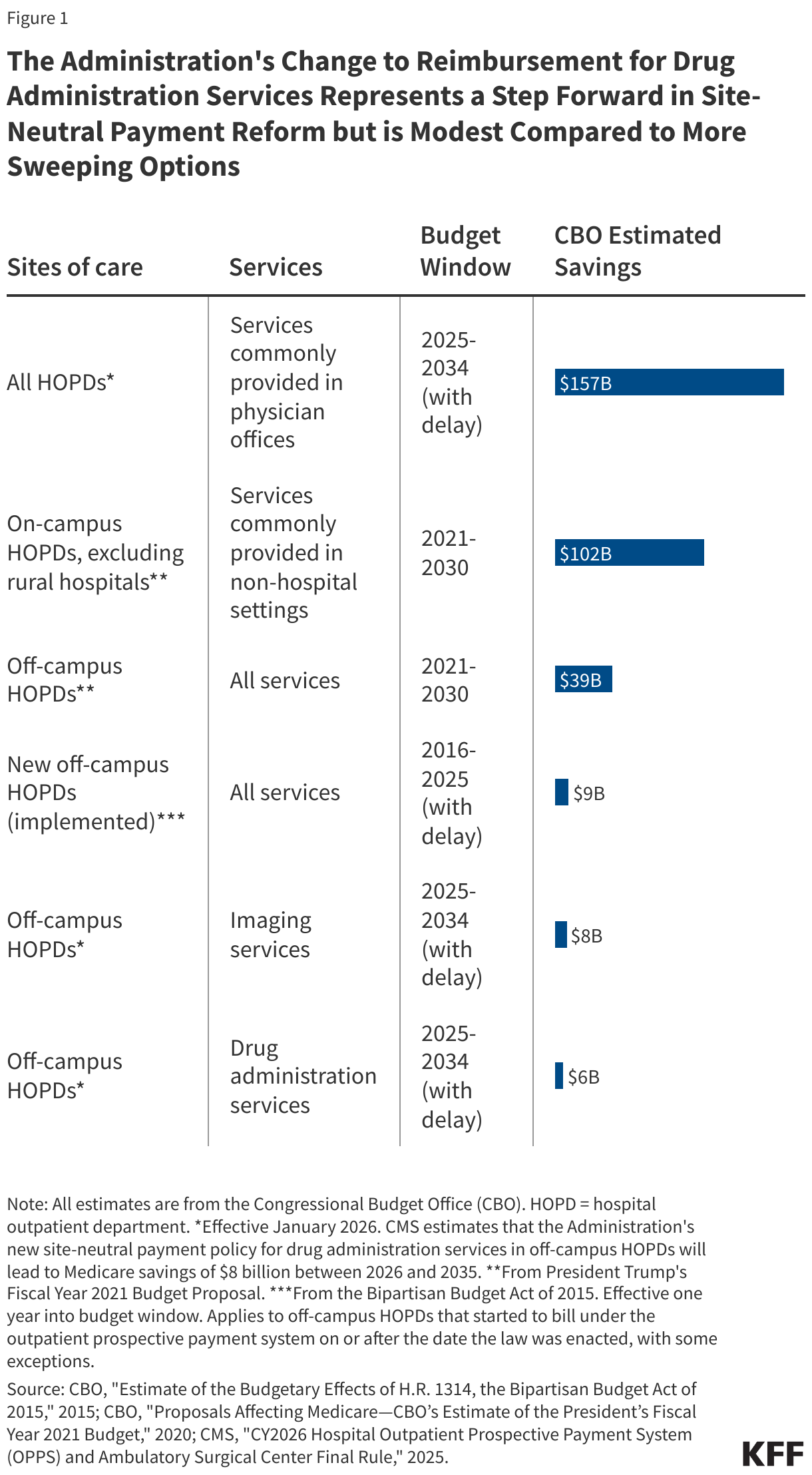
On November 21, 2025, the Centers for Medicare & Medicaid Services (CMS) released the 2026 final rule for the hospital outpatient prospective payment system (OPPS) under the traditional Medicare program. Among other things, CMS announced that it will reduce OPPS reimbursement for drug administration services (such as chemotherapy) when provided in off-campus hospital outpatient departments (HOPDs), i.e., those that are not part of the main hospital campus. The Administration’s change to reimbursement for drug administration services represents a step forward in implementing site neutral payment reforms but is modest compared to some of the more sweeping options raised by MedPAC and others.
The idea behind site-neutral payments is for Medicare to align reimbursement for outpatient services across care settings. Traditional Medicare often pays more for outpatient services when provided in hospital outpatient departments versus other care settings, like freestanding physician offices. Medicare has reduced payments for services provided in relatively new off-campus HOPDs (beginning in 2017) and for clinic visits provided in all other off-campus HOPDs (beginning in 2019) to align with what it pays for the same services in physician offices. The Administration’s new rule extends site-neutral payments to drug administration services at all off-campus HOPDs by reducing rates by 60% beginning in 2026. This approach is similar to legislation passed by the House in 2023 but not signed into law.
Supporters of site neutral payment reforms say that Medicare should not pay more for services provided in HOPDs when they can be provided safely and effectively in lower-cost settings. Moreover, they argue that reforms would reduce Medicare spending and beneficiary cost sharing and premiums, lead to spillover effects that reduce spending in commercial markets, and reduce the incentive for hospitals to acquire physician practices, a practice that can lead to higher prices through market consolidation.
Opponents, principally the hospital industry, counter that the higher payments for services in HOPDs are reasonable because of the level of care patients need, the costs of maintaining emergency care and standby capacity, and other factors. Further, they argue that payment reductions could harm patients’ access to care by threatening hospital finances. It’s not yet clear whether the hospital industry will challenge the legality of the payment rule, as they did for a prior reform introduced through regulation.
The Trump Administration’s new site neutral payment policy represents a relatively modest change in comparison to some of the other potential site-neutral payment reforms (See Figure 1). For example, the Congressional Budget Office (CBO) projected that site-neutral payment reforms for off-campus drug administration services would reduce federal spending by $6 billion between 2025 and 2034 (less than CMS’s estimate of $8 billion in Medicare savings between 2025 and 2034 under the Administration’s new policy). In contrast, CBO estimated that aligning payments for services commonly provided in physician offices for both on-campus and off-campus HOPDs—similar to an approach raised by MedPAC—would save $157 billion between 2025 and 2034.
The Administration estimates that new site-neutral payment reforms for drug administration services will have a larger effect on urban than rural hospitals in 2026. The reforms will not apply to sole community hospitals (which are carved out under the rule) or critical access hospitals (which are not reimbursed under the OPPS), which together make up the majority (79%) of rural hospitals. The Administration also estimates that the policy change will have a disproportionate effect on hospitals that care for large numbers of Medicaid and other low-income patients. These facilities may also see larger reductions in revenues as a result of Medicaid cuts under the reconciliation law, also known as the One Big Beautiful Bill.