KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
A project by National Public Radio, the Kaiser Family Foundation, and Harvard University’s Kennedy School of Government examines the public’s views on immigration in America. The survey reviews native-born Americans’ and immigrants’ attitudes towards legal immigration; how immigration affects the American culture and economy; attitudes towards illegal immigration and government regulations; and how immigrants’ views differ from those of non-immigrants.
A project by National Public Radio, the Kaiser Family Foundation, and Harvard University’s Kennedy School of Government examines the public’s views on immigration in America. The survey reviews native-born Americans’ and immigrants’ attitudes towards legal immigration; how immigration affects the American culture and economy; attitudes towards illegal immigration and government regulations; and how immigrants’ views differ from those of non-immigrants.
The annual 50-state survey of enrollment and eligibility policies in Medicaid and SCHIP for low-income families reveals that nearly half of states (23) took actions that made it more difficult to secure and retain health coverage for children and families from April 2003 until July 2004.
A project by National Public Radio, the Kaiser Family Foundation, and Harvard University’s Kennedy School of Government examines the public’s views on immigration in America. The survey reviews native-born Americans’ and immigrants’ attitudes towards legal immigration; how immigration affects the American culture and economy; attitudes towards illegal immigration and government regulations; and how immigrants’ views differ from those of non-immigrants.
HIV/AIDS is a critical issue to many who may have questions for candidates concerning their positions on the U.S. response to the epidemic at home and abroad. The U.S. is faced with numerous challenges in addressing the epidemic, including: funding levels for global and domestic HIV/AIDS efforts; differing approaches to prevention, care, treatment, and research; and questions about the role of the U.S. as a leader in the global fight against the epidemic.
Background
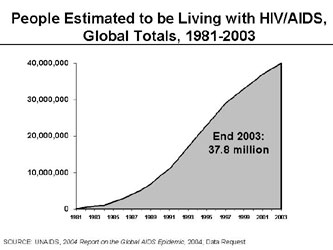
The Global EpidemicIn the more than two decades since the beginning of the HIV/AIDS epidemic, over 60 million people worldwide have become infected, including more than 20 million who have already died. 1 The number of people living with HIV/AIDS has grown significantly over time, with an estimated 37.8 million living with HIV/AIDS today (see Figure). Women now comprise almost half of adults living with HIV/AIDS and young people continue to bear the brunt of the epidemic, especially young women. Sub-Saharan Africa has been particularly affected, accounting for two-thirds of all people living with HIV/AIDS. 1 There are also growing concerns about “next wave” countries, those on the verge of major epidemics, particularly Russia, India, and China. Complicating the response worldwide is that most people with HIV/AIDS do not know they are infected. In addition, only eight percent of those in need of antiretroviral therapy are estimated to have access 2 and fewer than one in five are reached by prevention programs. 1 Finally, global funding for HIV/AIDS from governments and other donors falls far short of projected need. 1
The U.S. Epidemic
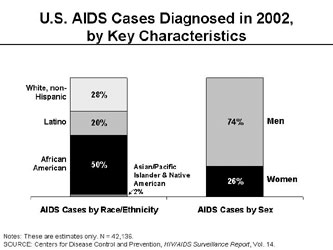
Almost one million people are estimated to be living with HIV/AIDS in the U.S. A significant proportion is not receiving regular HIV care, including medications for HIV, and an estimated one in four people with HIV do not know they are infected.3 Minority communities, young people, women, and men who have sex with men have been particularly hard hit. African Americans, for example, represent a growing proportion of new HIV infections and AIDS diagnoses, accounting for half of AIDS cases diagnosed in 2002. Women also represent an increasing proportion of AIDS diagnoses, accounting for about one quarter of new diagnoses in 2002 (see Figure). The number of new HIV infections each year – about 40,000 – has remained constant for more than a decade, but there are troubling signs that the incidence of HIV may be on the rise. 4,5 In addition, many of the critical programs that provide care, treatment, support, and prevention to people at risk for and living with HIV in the U.S. are facing resource constraints and, because of funding shortages, there are waiting lists for AIDS medications in several states.
Global HIV/AIDSU.S. Global HIV/AIDS Leadership. In 2003, the Administration announced the President’s Emergency Plan for AIDS Relief (PEPFAR), a new 5-year, $15 billion global HIV/AIDS initiative later enacted into law, which includes almost $10 billion in new funding. The bulk of the new funds ($9 billion) is targeted to 15 hard hit “priority” countries; up to $1 billion would be contributed to the Global Fund to Fight AIDS, Tuberculosis, and Malaria (Global Fund), an international partnership of governments and private organizations created to help finance the response to HIV/AIDS, TB, and malaria. The remaining $5 billion will go to continuing U.S. efforts in other countries.6
Global AIDS legislation and Administration policy include requirements for where and how the money gets spent, including targeting a subset of countries, limiting Global Fund contributions, and allocating specific funding percentages to prevention, including abstinence-only prevention, care, and treatment. Many have called for increased funding for global AIDS, and some policymakers support doubling U.S. assistance to $30 billion over five years and allocating a greater share to the Global Fund. Much of this discussion has centered on what should be the U.S. government’s “fair share” in the fight against the global epidemic. There have also been calls to expand beyond the 15 PEPFAR priority countries to include large, next wave countries, where more resources now could help prevent millions of infections. Other concerns have been raised about the need to get money to the front lines as quickly as possible and the importance of coordinating with other governments and donors and those in affected countries themselves.
Affordable Access to Treatment and Role of Generic Drugs. The high cost and complexity of combination antiretroviral therapy is an obstacle to HIV/AIDS treatment, particularly in poor countries but also within the U.S. Fixed-dose combination and co-packaged antiretroviral drugs, including those with generics, are seen as one way to expand access to treatment in highly affected countries because they are often more affordable and are easier for patients because they require fewer pills. The Administration has decided to allow PEPFAR funds to be used to purchase such medications for international use, but only if these drugs receive approval from the U.S. Food and Drug Administration (FDA) through an expedited process , stating that this is the only way to ensure that they are safe and effective. Critics of this approach argue that an existing World Health Organization (WHO) pre-qualification process is sufficient to ensure drug safety and quality, and is already used by other countries.
Immigration and Travel Ban. Longstanding U.S. policy prohibits people with HIV from immigrating to the U.S., as well as traveling to the U.S. (with limited exceptions). Some want the ban to be lifted, arguing that this policy is not based on public health principles but is instead a form of discrimination.
U.S. Epidemic
Care, Treatment, and Waiting Lists for Medications. Even in the U.S., not everyone with HIV/AIDS who needs medications can get them, and access to care and treatment varies significantly across the country – what you get depends on where you live. The Ryan White CARE Act, the nation’s largest program designed for people with HIV/AIDS, faces funding constraints in many parts of the country. The AIDS Drug Assistance Program (ADAP) of the Ryan White CARE Act in particular, which funds states to provide HIV medications to those who cannot get them elsewhere, faces continual funding shortages resulting in waiting lists for medications – as of August 2004, 9 state ADAPs had waiting lists, totaling more than 1,500 people. 7 ADAP funding constraints also lead to significant disparities in access to different HIV medications across states. 8 Medicaid and Medicare also play a critical role for people with HIV/AIDS, providing insurance coverage to about half of those receiving care.9 As people live longer with HIV/AIDS these programs will become even more important, raising important issues concerning the rising cost of prescription drugs, current eligibility rules for these programs, and state and federal funding constraints.10,11
Preventing New Infections. Because HIV incidence in the U.S. has remained steady for so long, current policy and program debates center on how to expand access to HIV testing, the role of community-based organizations vs. government in designing HIV prevention interventions, and how to balance prevention efforts between those who are at risk and those who are already HIV-positive. In both global and domestic HIV/AIDS debates, there are differing opinions about approaches to HIV prevention. The Administration, while endorsing an “ABC” approach (“Abstinence, Be faithful and when appropriate, use Condoms”), emphasizes abstinence as the only sure way to prevent sexual transmission of HIV and other sexually transmitted diseases. Others say that a comprehensive approach, one that includes but does not prioritize abstinence over condoms, is needed. U.S. global AIDS legislation requires a certain amount of funding to go to abstinence-only programs. For the U.S., President Bush has called for doubling funding for abstinence-only programs, which affects HIV prevention activities.
Minorities and Other Hard-Hit Populations. Specific challenges face policymakers in addressing the epidemic’s growing impact on minority populations, including how best to support existing efforts focused on minorities, such as the Minority AIDS Initiative 12 , as well as strengthen other programs that also serve minorities at risk for and living with HIV, and whether new approaches are also needed. There are also challenges about how best to address the U.S. epidemic’s impact on women and other vulnerable groups.
Assessing Candidate Positions
The following questions are intended to help evaluate candidate positions on HIV/AIDS:
What should the U.S. role be in addressing the global HIV/AIDS epidemic? How much funding should be provided to the overall effort and to the Global Fund specifically?
Should the U.S. require that funds used to purchase low-cost generic HIV/AIDS drugs for people in other countries be limited to FDA-approved drugs or will certification by international bodies such as the World Health Organization be sufficient?
Should people with HIV be barred from immigrating or traveling to the United States?
What should be the balance in domestic and global HIV/AIDS prevention programs between emphasizing abstinence-only prevention or a comprehensive approach that includes abstinence?
What level of support should be provided to programs that deliver care and treatment to people with HIV/AIDS in the United States? With the growing concentration of HIV/AIDS in minority populations, what new approaches are needed and what programs should be strengthened?
1 UNAIDS, 2004 Report on the Global AIDS Epidemic, July 2004.2 World Health Organization, “Coverage of Adults in Developing Countries on Antiretroviral Treatment, by WHO Region, Situation as of June 2004”.3 Fleming, P., et al., “HIV Prevalence in the United States 2000”, 9th Conference on Retroviruses and Opportunistic Infections, 2002.4 Centers for Disease Control and Prevention, MMWR, “Advancing HIV Prevention: New Strategies for a Changing Epidemic – United States, 2003”, Vol. 52, No. 47, November 2003.5 Centers for Disease Control and Prevention, MMWR, “Increases in HIV Diagnoses – 29 States, 1999 – 2002”, Vol. 52, No. 15, April 2003.6 State Department, Fact Sheet: The President’s Emergency Plan for AIDS Relief Five-Year Strategy, September 2004.7 National Alliance of State and Territorial AIDS Directors, The ADAP Watch, August 2004.8 National Alliance of State and Territorial AIDS Directors, Kaiser Family Foundation, AIDS Treatment Data Network, National ADAP Monitoring Project – Annual Report, May 2004.9 Bozzette, et al., “The Care of HIV-Infected Adults in the United States.” NEJM, Vol. 339, No. 26. December, 1998.10 Kaiser Family Foundation, Fact Sheet: Medicaid and HIV/AIDS, September 2004.11 Kaiser Family Foundation, Fact Sheet: Medicare and HIV/AIDS, September 2004.12 Kaiser Family Foundation, Policy Brief: The Minority AIDS Initiative, June 2004.
This paper, by Joy Pritts of the Health Policy Institute at Georgetown University, looks at issues related to drug plan marketing activities and privacy under the MMA.
Health care costs in general have grown faster than the economy. Although still only a modest part of total health care spending in the United States (11% in 2002), the growth in pharmaceutical spending has outpaced other categories of health care services over the last few years. What, if anything, should the government do to make prescription drugs more affordable?
Background
Developments in pharmaceuticals have transformed health care over the last several decades. Today, many diseases are prevented, cured, or managed effectively for years through the use of prescription drugs. In some cases the use of prescription drugs keeps people from needing other expensive health care such as being hospitalized or having surgery.
These advances have not come without a price. In 2002, spending on prescription drugs in the U.S. grew 15 percent compared to a 9 percent increase for all health care. 1 This growth in spending on prescription drugs is due to three factors: increased use of prescription drugs in general, the higher costs for new products coming to market and replacing existing drugs, and increases in drug prices. In 2002, the average price of a retail prescription grew almost 6 percent, reflecting the influence of newer, higher priced prescription products in the market. 2
The prices for prescription drugs reflect the consumer demand, or willingness to pay for medications, and the patent system, which encourages manufacturers to invest in developing new drugs. Consumer demand has been affected by the growth in private third-party payment for pharmaceutical products, which means that consumers directly see only a small part of increasing drug costs when they fill a prescription. 3 Another possible factor has been the growth in direct-to-consumer marketing of pharmaceutical products, which encourages consumers to ask their doctors about new medications 4,while increasing their knowledge about drug options.
Patents affect prices by providing manufacturers who develop new pharmaceutical products an exclusive right to sell the drug for 20 years from the date of the patent filing. 5 The actual costs for making most prescription drug products are relatively small (although such costs may be significantly higher in some cases, such as for biotechnology products), and thus, the prices for a drug are usually considerably lower once the patent expires and generic competition enters the market. Therefore, the company that developed the drug must recoup its investment and make most of its profit on a product during the period it has the patent. Once the patent expires, the drug may be manufactured in generic versions by any number of manufacturers. 6 Even during the patent years, other products to treat the same condition may come to market, producing price competition among therapeutic options.
Manufacturers make substantial investments in the products that they bring to market, and to be profitable, they must recoup not only the development costs of successful drugs and devices, but also, the costs for research and development for products that never make it to market. Only one in five medicines that enter the clinical testing process ever gain Food and Drug Administration (FDA) approval and enter the market. 7 Thus far, however, drug makers have been able to make a profit. From 1995 through 2002, pharmaceutical manufacturing was the most profitable industry in the U.S. Profitability declined somewhat in 2002, and in 2003 it ranked third with profits after taxes of about 14 percent. 8
The cost of prescription drugs has commanded considerable public attention over the last decade. People with coverage for their prescription expenses have seen their cost-sharing for brand products increase substantially as employers and health plans move to arrangements which provide financial incentives for consumers to use lower cost drugs. 9 People without drug coverage, including many Medicare beneficiaries, often pay the highest prices for prescription medications, and must confront rapid cost increases directly. In response to concerns over the out-of-pocket cost burdens on the elderly and disabled, Congress passed a law last year that provides new Medicare outpatient prescription drug benefits that will be available beginning on January 1, 2006. While government assistance will be comprehensive for low-income beneficiaries, the benefits for others are such that many Medicare beneficiaries will still be paying large amounts out-of-pocket for their medicines.
Options for for making prescription drugs more affordable
While there are a number of policy options under consideration for addressing rising drug costs, the two that are currently receiving the most political attention are reimportation and the government’s role concerning drug prices in the Medicare program.
Importation. Proposals that would allow Americans to purchase drugs from other countries are referred to under the terms “importation” or “reimportation”. 10 It is currently illegal to import prescription drugs into the U.S. from other countries, and only the original manufacturer may reimport a pharmaceutical product, subject to meeting certain standards on how they are handled and labeled. In practice, however, the FDA, which is the federal agency responsible for overseeing pharmaceutical products, does not enforce the law banning importation in certain circumstances where drugs are imported for personal use.
The significantly lower prices available for common prescription drugs in bordering countries, Canada and Mexico, has led some Americans to import drugs from those countries and has encouraged politicians of both parties to propose lifting the import ban. Congress has passed legislation allowing for expanded importation of drugs on several occasions but the laws were never implemented because they required that the Secretary of the Department of Health and Human Services (HHS) conclude that safety could be maintained and that costs would significantly be reduced. Both HHS Secretary Shalala in the Clinton Administration, and Secretary Thompson in the Bush Administration concluded that they could not meet these standards.
A number of bills on importation have been introduced in the current Congress. The bills differ in a number of ways. Some would allow drugs to be imported only for personal use while others would allow imports for commercial purposes. The bills also differ in terms of the countries from which drugs could be imported, safety standards, regulatory requirements, and fees that would be levied to help pay the costs of increased government regulation. In addition, a number of states, including Illinois, Iowa, Michigan, Minnesota, and Ohio, as well as a number of cities, have undertaken efforts to get lower drug prices for their residents through purchase from other countries. They are doing this in order to reduce state costs for providing drug benefits to state employees, or to make it easier for their residents to import drugs. Although the FDA has not approved these efforts, it also as yet has not stopped them.
Would allowing importation result in lower prescription drug costs for American consumers? There are varying opinions on this issue, but most experts caution that savings cannot be guaranteed, especially if importation is limited to only certain countries, such as Canada. 11 The Congressional Budget Office (CBO), the agency responsible for estimating the financial impact of federal policy changes, concludes that the effect would be small. 12 It acknowledges that prices for drugs still under patent protections (as opposed to generic products) are 35 percent to 55 percent lower in other countries than in the U.S. However, it cautions that responses by foreign governments and by the pharmaceutical industry to such a change in policy could erode most savings. For example, foreign governments could restrict the supply of drugs leaving their borders; or pharmaceutical manufacturers could limit the supply of drugs sold to foreign nations that facilitate sales to U.S. purchasers.
On the other hand, those who advocate in favor of allowing importation acknowledge that drug importation limited only to Canada would not be a long-term solution. 13 They believe that if importation were legal from other countries, including the Asian and European markets, as well as from Canada, there would be enough volume to significantly affect prices in the U.S. market. 14 They also believe that the potential of lower prices from foreign countries will cause U.S. pharmacies to cut their prices in order to be competitive. At the very least, they feel that the debate around importation makes people aware of the fact that prices are lower in other countries and puts continued pressure on drug makers to keep their U.S. prices in check.
Supporters of importation also argue that the safety issue can be addressed. For example, legislation which passed the U.S. House of Representatives with bipartisan support would limit reimportation to FDA-approved drugs manufactured in FDA-approved facilities in 25 countries, require the use of counterfeit-resistant packaging (or testing of each pharmaceutical shipment that does not use such packaging), and give the Secretary of Health and Human Services the power to immediately halt importation if a product violates the law. 15 Opponents argue that these safeguards are not adequate. Bills on importation that have been introduced in the Senate are still awaiting action and may not be debated before Congress adjourns.
Government’s role in Medicare drug prices. The second visible issue in the 2004 campaign relating to drug prices involves the appropriate role for government regarding drug prices for Medicare beneficiaries. The Medicare Modernization Act of 2003, which establishes outpatient prescription drug coverage for Medicare beneficiaries beginning in 2006, relies on competition among private health plans to make drugs available to beneficiaries at reasonable prices. Medicare beneficiaries who wish to participate in the new program will have to enroll in one of the Medicare drug plans available to them in their area of residence. Each plan will be responsible for negotiating with drug manufacturers and pharmacies to determine the prices for medicines that will apply under the plan. Because the drug benefits are limited for beneficiaries who are not low-income, many seniors will have access to lower prices, but will also still have significant out-of-pocket costs for their medicines. The law specifically prohibits the government from interfering in the negotiations between the drug plan sponsors and drug manufacturers and pharmacies. It also prohibits the government from establishing any specific list of drugs that will be covered (formulary) or imposing any price controls on drugs.
Supporters of the market-based approach in the new Medicare law believe that the competition for enrollees will cause plans to negotiate with drug manufacturers and pharmacies to offer drugs at the lowest possible prices. They believe that permitting the government to set prices for Medicare would not necessarily guarantee lower prices, may have unintended consequences on the rest of the market, and would negatively affect patients because government price controls would stifle industry incentives to invest in research and development of new therapies.
Some people argue that the current market-based tools being used by health plans and pharmaceutical benefit managers (PBMs) have not been effective, and that prices for brand pharmaceutical products are considerably higher in the U.S. than in other countries where governments take a more active role in negotiating prices and rates of return with manufacturers. It should be noted that the federal government regulates prescription drug prices in the fee-for-service Medicaid program and the veterans’ health program. 16 Opponents of market-based tools also suggest that in cases where manufacturers have exclusive rights for drugs with few or no competitors, competition may have little or no impact on price. They support removing from the law the ban on government interference and price setting, and granting the government the authority to directly negotiate prices with manufacturers. Some advocate that this authority not be used unless the private plans are not able to achieve lower prices. Other options include using this power only for certain drugs for which there is no competition.
Assessing Candidate Positions
While there is no clear partisan division between Republicans and Democrats on the issue of importation, candidates tend to be more divided regarding government intervention in drug pricing, aligning themselves with those who support a market-based approach versus those who favor more government intervention. Included below are a series of questions to help evaluate candidate positions on prescription drug costs.
Should the U.S. allow people to buy prescription drugs from other countries? Under what circumstances?
What can be done to assure the quality and safety of prescription medicines imported into the U.S.?
If people in the U.S. are allowed to import drugs, will drug companies invest less in research and development? If so, are there any measures the government can take to encourage companies to do research and development?
Is a market-based system or government intervention the most effective way to control drug costs for seniors? If prescription medicines remain unaffordable for many seniors after the Medicare drug law goes into effect, what approach should be taken?
Prepared by Health Policy Alternatives, Inc.
1 National Health Expenditures Tables. http://www.cms.hhs.gov/statistics/nhe/historical/t2.asp.2 Lundy, Janet, Benjamin Finder, and Gary Claxton. Trends and Indicators in the Changing Health Care Marketplace, 2004 Update. Kaiser Family Foundation. April 2004. Exhibit 1.18.3 The percentage of prescription drug costs paid for by private health insurance increased from 24 percent in 1990 to 47 percent in 2001. Fact Sheet: Prescription Drug Trends, Kaiser Family Foundation, May 2003. Figure 2.4 Rosenthal, Meredith B., et al. Demand Effects of Recent Changes in Prescription Drug Promotion, Kaiser Family Foundation, June 2003. Direct to consumer advertising rose by 28 percent annually between 1996 and 2001. The study found that increases in direct-to-consumer advertising between 1999 and 2000 accounted for 12 percent of drug sales growth during that period.5 However, the effective patent period is usually shorter because patents are obtained before the products are approved for marketing.6 Often, in order to extend their favorable market situation, a company may get a new patent on a slightly different version of a drug about to go off patent.7 Di Masi, Joseph A. “Success Rates for New Drugs Entering Clinical Testing in the United States,” 58 Clinical Pharmacology and Therapeutics, 1995, p. 1-14.8 Lundy, Janet, Benjamin Finder, and Gary Claxton. Trends and Indicators in the Changing Health Care Marketplace, 2004 Update. Kaiser Family Foundation. April 2004. Exhibit 1.21.9 Between 2000 and 2004, copayments in multi-tier arrangements increased by 62 percent for preferred brand drugs and by 94 percent for non-preferred brand drugs. Henry J. Kaiser Family Foundation and Health Research and Educational Trust, Employer Health Benefits Annual Survey, 2000 and 2004.10 Importation refers to bringing products into the U.S. from other countries, whereas reimportation means bringing back into the U.S. products that were produced here and exported to another country.11 Schuler, Kate. Weighing Promise and Perils of Drug Importation. CQ Weekly, July 24, 2004. p. 1791.12 CBO. Would Prescription Drug Importation Reduce U.S. Drug Spending, April 29, 2004. http://www.cbo.gov/showdoc.cfm?index=5406&sequence=013 Families USA. Written testimony submitted to the U.S. Committee on Finance, Hearing on International Trade and Pharmaceuticals, April 27, 2004.14 Schuler, Kate. Weighing Promise and Perils of Drug Importation. CQ Weekly, July 24, 2004. p. 1790.15 See H.R. 2427 (108th Congress).16 For example, in Medicaid, the government requires manufacturers to provide rebates to state governments for outpatient drugs, effectively reducing the price the state pays for the drug.
Papers on Issues For People With Medicare Raised By Proposed Drug Benefit Regulations
The Kaiser Family Foundation has commissioned a series of papers to explore key issues that may be of concern for Medicare beneficiaries as the new Medicare drug benefit is implemented. These papers focus on specific areas of potential concern for people with Medicare. In addition, the Foundation also has produced a timeline of upcoming important dates leading up to the implementation of the new drug benefit.
Issue Paper — Marketing and Privacy Issues: An Analysis of the MMA and Proposed Regulations
Issue Paper — Issues for Medicare Beneficiaries in Long-Term Care Facilities: An Analysis of the MMA and Proposed Regulations
Issue Paper — Grievance and Appeals Procedures: An Analysis of the MMA and Proposed Regulations
Issue Paper — The Effect of Formularies and Other Cost Management Tools on Access to Medications: An Analysis of the MMA and Proposed Regulations
Timeline — Medicare Prescription Drug Improvement and Modernization Act Implementation Timeline: June 2004 – December 2006 Key Dates
This comprehensive survey of people on Medicare, conducted in June and July 2004, assesses their attitudes toward the new Medicare drug law. This chartpack, issued in September 2004, presents additional analysis on the survey data, looking at key findings broken down by income group.