Mental Health Care Needs and Experiences Among LGBT+ People
Issue Brief
Key Findings
There has been rising attention to the scope of mental health challenges in the United States, including a desire to better understand the experiences and needs of those who may be most heavily impacted. The LGBT+ community is one such group, having faced lifelong mental health challenges beginning in adolescence and persisting through adulthood. While in some cases, LGBT+ people are accessing mental health care more frequently than non-LGBT+ people, their need for services is greater, and gaps remain. Today, policies seeking to curtail access and rights of LGBT+ people threaten to worsen these disparities, and continuing to monitor the wellbeing of the community will be important.
With this report, we examine LGBT+ people’s needs for and experiences accessing mental health care by analyzing data from a nationally representative 2022 KFF survey with a large sample of LGBT+ adults. Key findings include:
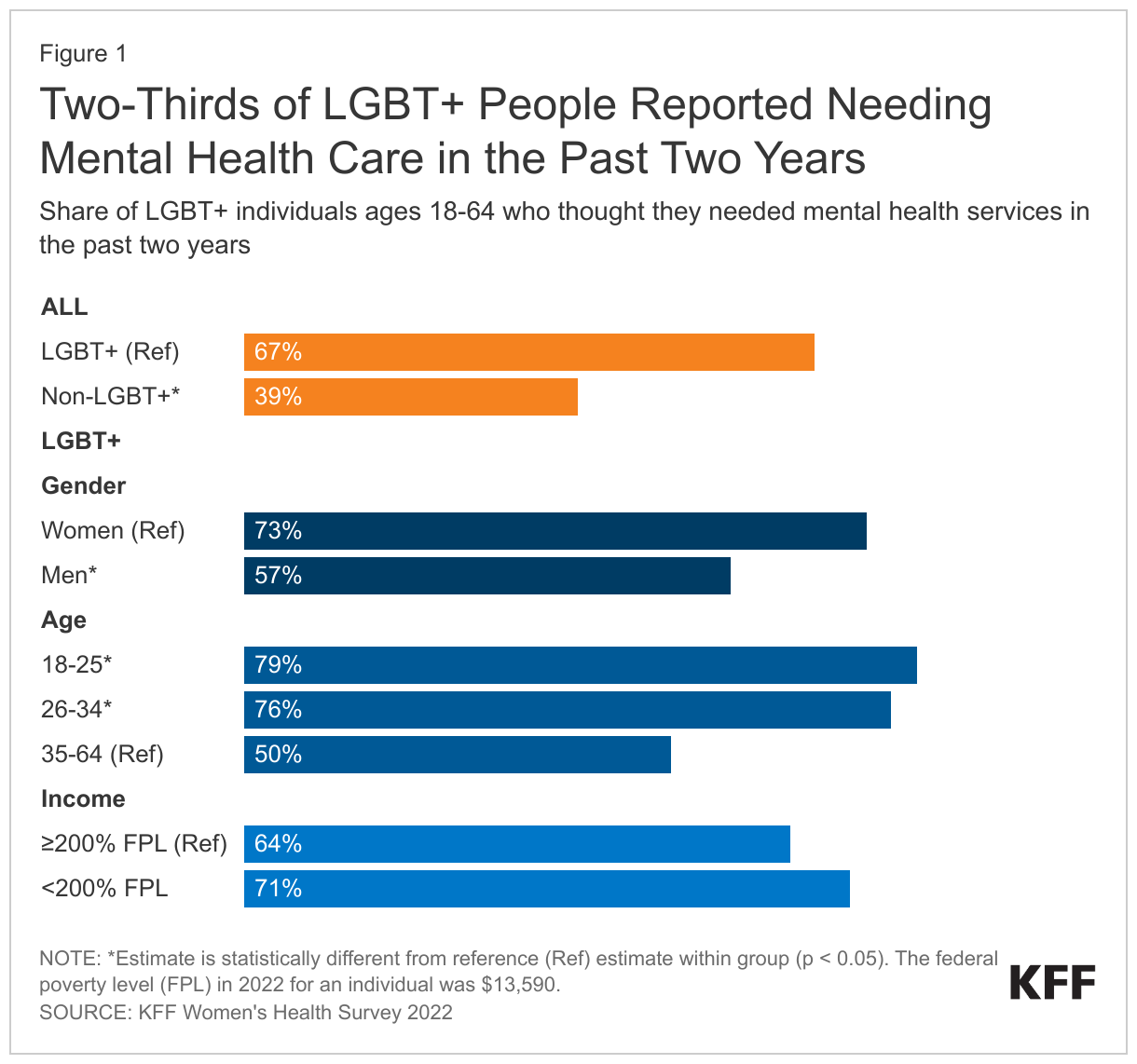
- Two-thirds of LGBT+ people (67%) reported needing a mental health service over the past two years, a considerably higher share than for non-LGBT+ people (39%).
- Yet, only about half of LGBT+ people with a reported need sought and received mental health services (similar to the share among non-LGBT+ people).
- Barriers to care can include:
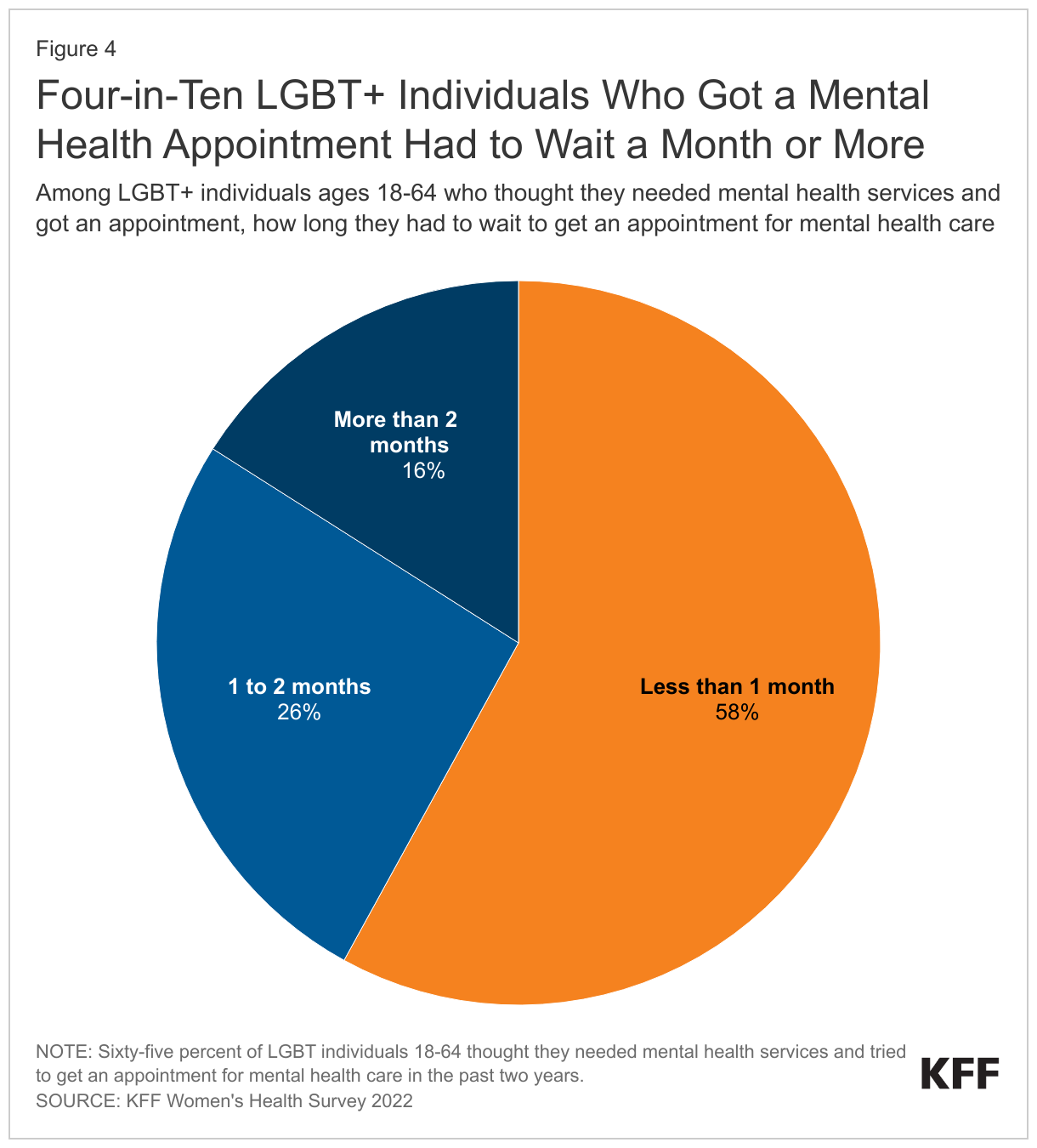
- Wait times: Four-in-ten LGBT+ people reported having to wait at least a month for services.
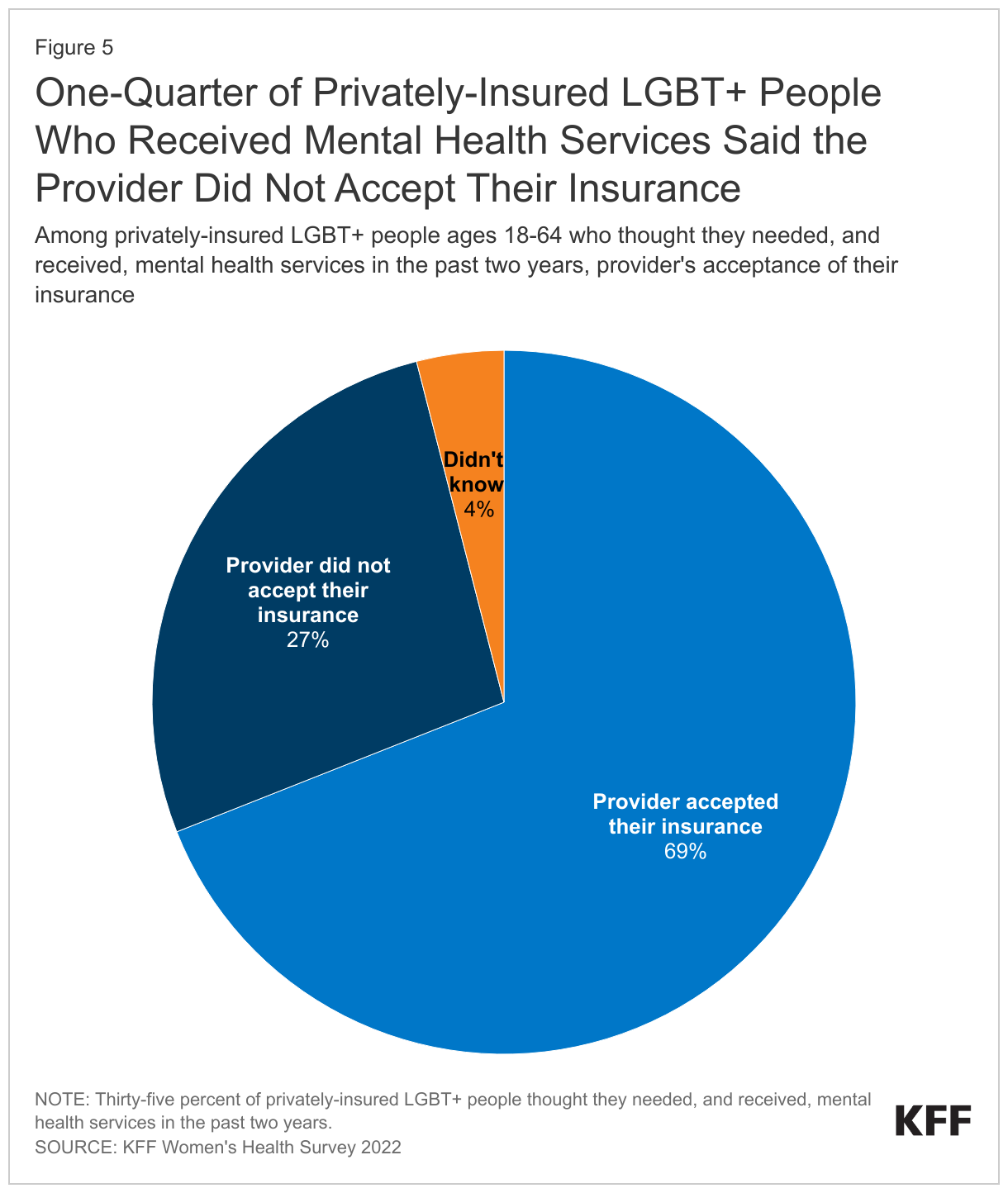
- Insurance: One-quarter of privately insured LGBT+ people who received mental health services said their provider did not take their insurance.
Introduction
There has been rising attention to the depth and breadth of mental health challenges in the United States, including a desire to better understand the experiences and needs of those most heavily impacted. A recent KFF/CNN poll found that nearly all (90%) Americans believe there is a mental health crisis today and that LGBT+ adults consistently reported poorer mental health outcomes on almost all measures throughout the survey.
Indeed, the LGBT+ community has faced lifelong mental health challenges beginning in adolescence and persisting through adulthood at higher rates compared to non-LGBT+ people. Additionally, while in some cases, LGBT+ people are accessing mental health care more frequently than non-LGBT+ people, their need for services is greater and gaps remain. Addressing systemic factors that drive stigma and discrimination within the community could play a key role in mitigating these challenges alongside improving access more generally.
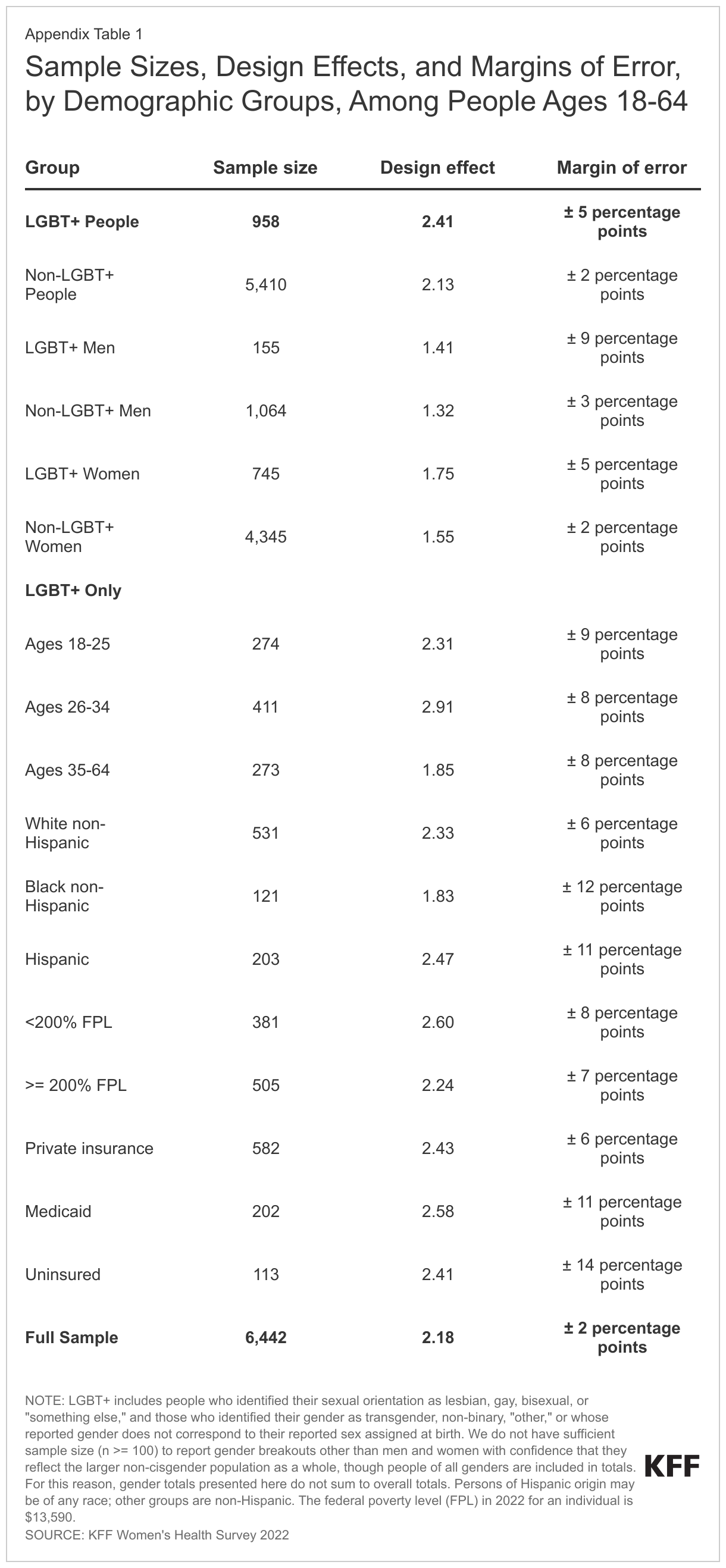
With this report, we provide an update on LGBT+ people’s needs for and experiences of accessing mental health care by analyzing data from a nationally-representative 2022 KFF survey of 6,442 adults ages 18 to 64, including 958 LGBT+ people, conducted primarily online from May 10, 2022, to June 7, 2022. For this survey, LGBT+ people include those who identified their sexual orientation as lesbian, gay, bisexual, or “something else,” and those who identified their gender as transgender, non-binary, “other,” or whose reported gender does not correspond to their reported sex assigned at birth. (See the Methodology for additional detail.) Beyond issues related to mental health and access to care, the survey collected data on a range of demographic characteristics and issues from general well-being to experiences engaging in the health system, use of preventive services including HIV and STI testing, and reproductive health. A separate companion issue brief, LGBT+ People’s Health Status and Experiences Accessing to Care, provides these additional findings.
Findings
Experiences with Mental Health Problems
Surveys regularly find that LGBT+ people face greater mental health challenges than non-LGBT+ people, including for common conditions like depression and anxiety, as found in a recent KFF/CNN poll.
Here we find that two-thirds of LGBT+ people (67%) reported needing a mental health service over the past two years, a considerably higher share than the one-in-four non-LGBT+ people (39%). Self-reported need for mental health care was highest among younger LGBT+ people under age 35 (77%) and for women, nearly three-quarters of whom (73%) reported the need for mental health care (Figure 1).
Accessing Mental Health Care
The higher rates of stigma, discrimination, and violence experienced by LGBT+ populations can translate into mental health and substance use challenges. For many who are part of this community, these challenges highlight the need for behavioral health care.
While reported need for mental health services was high among LGBT+ people, not all of those with a need for services sought or received them. Notably, a higher share of LGBT+ people have both a need for mental health service than non-LGBT+ people, and higher shares sought and received mental health services than their non-LGBT+ counterparts. Yet, unmet need persisted for many in both groups.
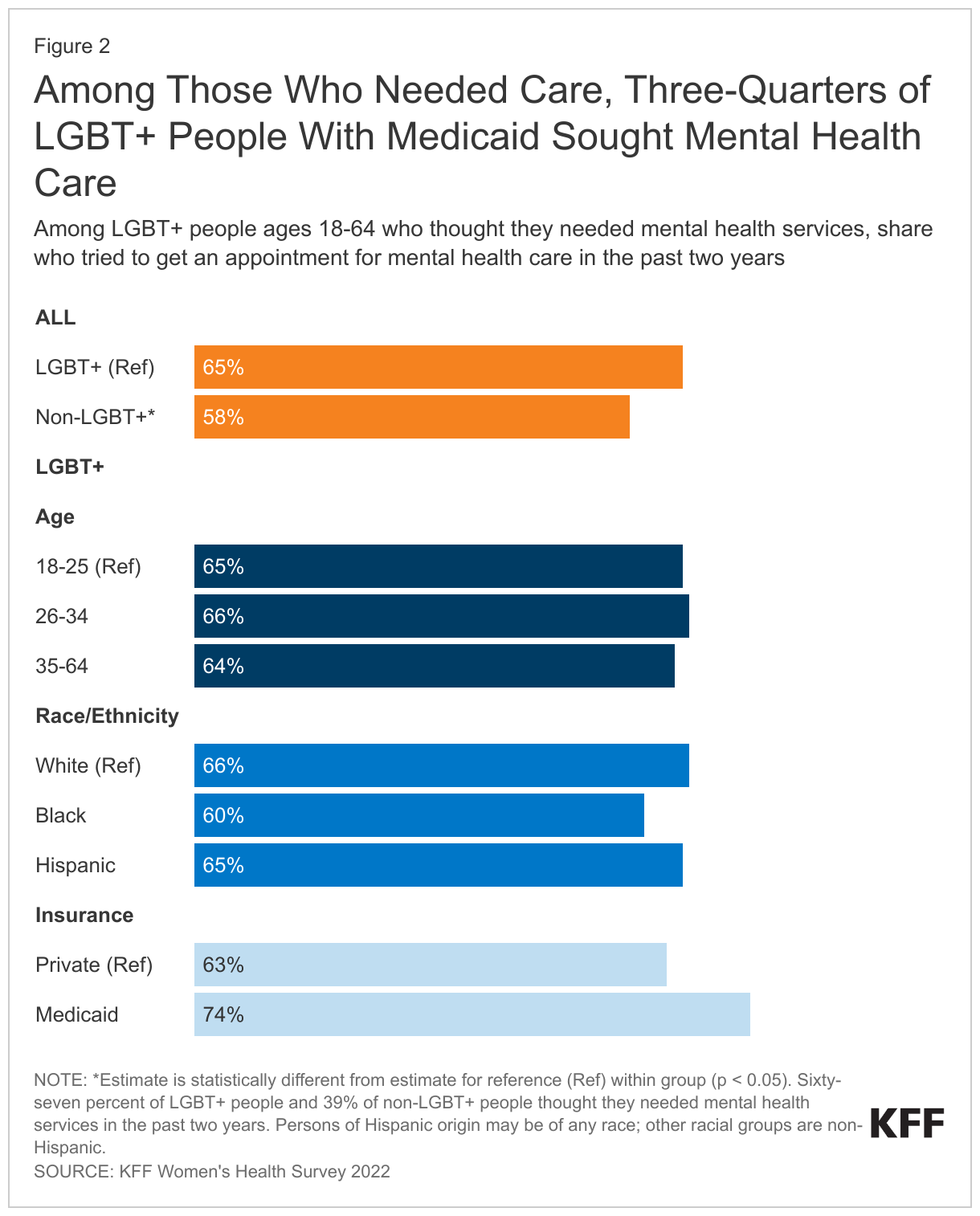
Two-thirds (65%) of LGBT+ people who reported needing a mental health service sought one, compared to 58% of non-LGBT+ people, still leaving many without desired services (Figure 2). There were no statistical differences in the share that sought services by age, race/ethnicity, or insurance status among LGBT+ people. Limited uptake could be due to being a lower-income group, having lower rates of private coverage, or experience of stigma, discrimination shame and trauma, including within medical settings. See the issue brief LGBT+ People’s Health Status and Experiences Accessing to Care for more details.
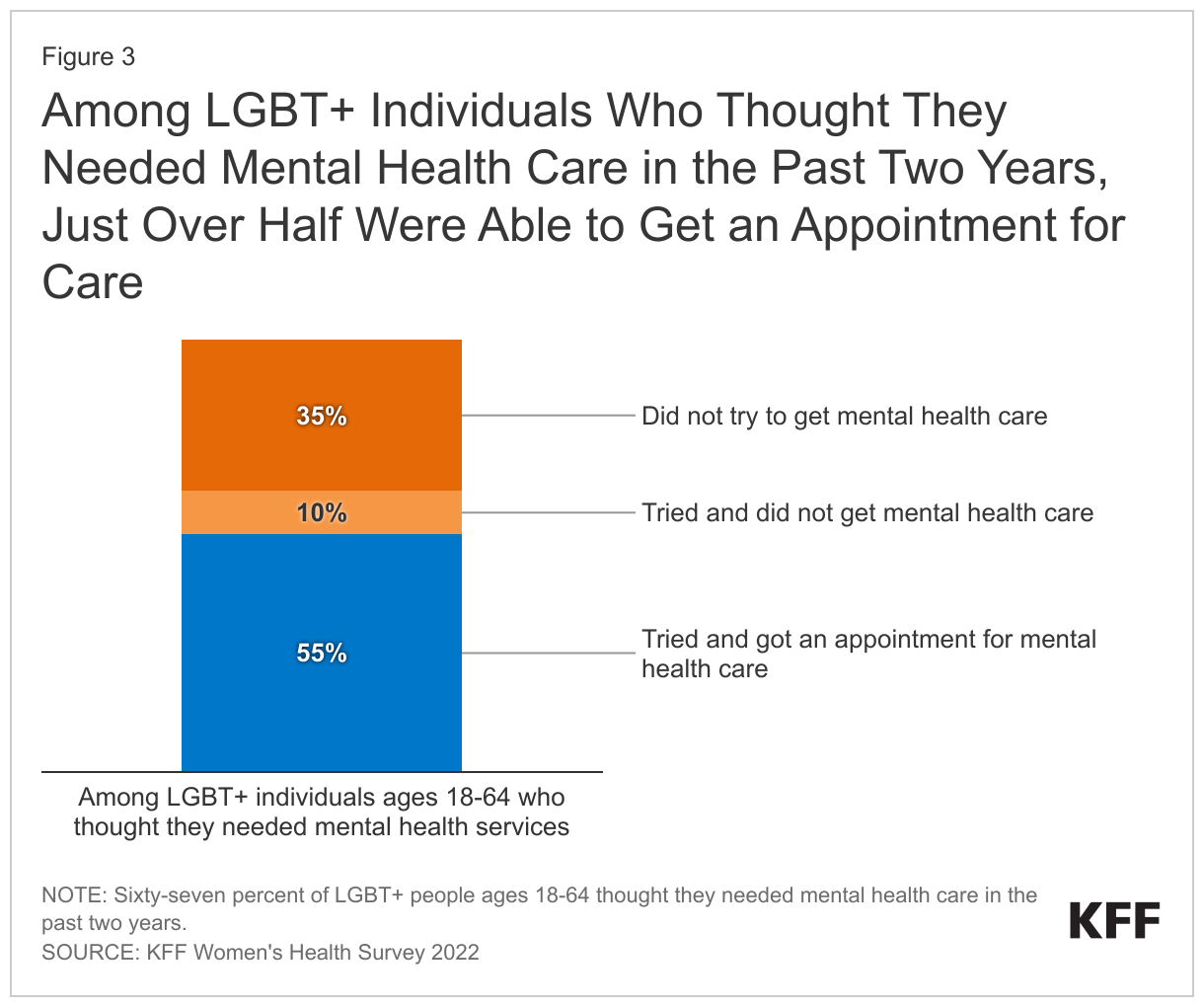
Only about half of LGBT+ people (55%) and non-LGBT+ people (49%) who reported a need for mental health services over the past two years received care, pointing to substantial unmet need in this area regardless of gender identity or sexual orientation. One-in-ten (10%) LGBT+ who reported a need for these services said they tried to get but did not receive care, also similar to non-LGBT+ people. One-third (35%) with a need did not try to get mental health care (Figure 3). A smaller share of LGBT+ individuals with a need did not try to get mental health care compared to non-LGBT+ individuals (35% vs. 42%).
Since the COVID-19 pandemic, telehealth has emerged as an important avenue for people to access health care, including mental health services. Almost two-thirds of LGBT+ people (63%) reported having had a telehealth visit in the last year and mental health services was the leading reason for their most recent telehealth visit – 28% received mental health services, followed by an annual check-up or well-visit (21%). Telehealth can increase access to mental health services, including for those who might not otherwise get or want in-person care (data not shown in figure).
Barriers to Mental Health Care
Among LGBT+ people who were able to get a mental health appointment, about six-in-ten (58%) were able to get one in less than a month, but four-in-ten (42%) had to wait one month or more, with 16% waiting more than two months. These were similar to the shares among non-LGBT+ people. Such delays can be a barrier to getting people into care, particularly when those who have to wait may end up not seeking care at all if that wait is for a substantial period. These delays can prolong suffering and lead to worsening of symptoms (Figure 4).
Seven-in-ten (69%) privately insured LGBT+ people reported their mental health provider accepted their insurance plan, but 27% said they did not, and 4% didn’t know, shares similar to privately insured non-LGBT+ people (Figure 5).
Conclusion
LGBT+ people experience significantly higher rates of mental health challenges and need for mental health services than non-LGBT+ people, as well as higher rates of health care discrimination. While they also reported accessing mental health care at slightly higher rates than non-LGBT+ people, nearly half who said they could benefit from such services went without. The findings presented here suggest that in addition to inability to secure appointments, wait times may also be a barrier to care. A facilitator to mental health care appears to be telehealth, with more than one-quarter of LGBT+ people accessing telehealth care doing so for mental health services.
The reasons that LGBT+ people are more likely to face mental health challenges are complex and may relate, in part, to widespread experiences of stigma and discrimination. Current attempts to institute anti-LGBTQ policies in many states and communities may contribute to poor mental health outcomes and increase the need for care. Targeted and culturally appropriate policy solutions aimed at improving the well-being of the LGBT+ community and addressing their access challenges to mental health care could help to meet their mental health care needs, as would efforts to address systemic factors that drive stigma and discrimination within the community.
Methods
Methods
Data for this issue brief come from the 2022 KFF Women’s Health Survey, a nationally representative survey of 6,442 people of all genders ages 18 to 64, including 958 LGBT+ people, conducted from May 10, 2022, to June 7, 2022. The objective of the survey is to help better understand respondents’ experiences with contraception, potential barriers to health care access, and other issues related to reproductive health. The survey was designed and analyzed by researchers at KFF (Kaiser Family Foundation) and fielded online and by telephone by SSRS using its Opinion Panel, supplemented with sample from IPSOS’s KnowledgePanel.
The survey asked respondents which sex they were assigned at birth, on their original birth certificate (male or female). They were then asked what their current gender is (man, woman, transgender, non-binary, or other). Those who identified as transgender men are coded as men and transgender women are coded as women. While we attempted to be as inclusive as possible and recognize the importance of better understanding the health of non-cisgendered people, as is common in many nationally representative surveys, we did not have a sufficient sample size (n >= 100) to report gender breakouts other than men and women with confidence that they reflect the larger non-cisgender population as a whole. The data in our reproductive health analyses use the respondent’s sex assigned at birth (inclusive of all genders) to account for reproductive health needs/capacity (e.g., ever been pregnant) while other analyses use the respondent’s gender (inclusive of males and females).
For this survey, LGBT+ people include those who identified their sexual orientation as lesbian, gay, bisexual, or “something else,” and those who identified their gender as transgender, non-binary, “other,” or whose reported gender does not correspond to their reported sex assigned at birth.
Questionnaire design
KFF developed the survey instrument with SSRS feedback regarding question wording, order, clarity, and other issues pertaining to questionnaire quality. The survey was conducted in English and Spanish. The survey instrument is available upon request.
Sample design
The majority of respondents completed the survey using the SSRS Opinion Panel (n=5,202), a nationally representative probability-based panel where panel members are recruited in one of two ways: (1) through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Group through the U.S. Postal Service’s Computerized Delivery Sequence. (2) from a dual-framed random digit dial (RDD) sample provided by Marketing Systems Group.
In order to have large enough sample sizes for certain subgroups (females ages 18 to 35, particularly females in the following subgroups: lesbian/gay/bisexual; Asian; Black; Hispanic; Medicaid enrollees; low-income; and rural), an additional 1,240 surveys were conducted using the IPSOS KnowledgePanel, a nationally representative probability-based panel recruited using a stratified ABS design. (Note that due to small sample sizes, data for LGBT+ people who are Asian or Pacific Islanders are not presented in this report.)
Data collection
The majority of surveys completed using the SSRS Opinion Panel (n=5,056) and all of the surveys completed using the KnowledgePanel (n=1,240) were self-administered web surveys. Panelists were emailed an invitation, which included a unique passcode-embedded link, to complete the survey online. In appreciation for their participation, panelists received a modest incentive in the form of a $5 or $10 electronic gift card. In addition to the self-administered web survey, n=146 surveys were completed by telephone with SSRS Opinion Panelists who are web reluctant.
Weighting
The data are weighted to represent U.S. adults ages 18 to 64. The data include oversamples of females ages 18 to 35 and females ages 36 to 64. Due to this oversampling, the data were classified into three subgroups: females 18 to 35, females 36 to 64, and males 18 to 64. The weighting consisted of two stages: 1) application of base weights and 2) calibration to population parameters. Each subgroup was calibrated separately, then the groups were put into their proper proportions relative to their size in the population.
Calibration to Population Benchmarks
The total sample for the Women’s Health Survey was balanced to match estimates of each of the three subgroups (females ages 18 to 35, females ages 36 to 64, and males ages 18 to 64) along the following dimensions: age; education (less than a high school graduate, high school graduate, some college, four-year college or more); region (Northeast, Midwest, South, West); and race/ethnicity (White non-Hispanic, Black non-Hispanic, Hispanic-born in U.S., Hispanic-born Outside the U.S., Asian non-Hispanic, Other non-Hispanic). The sample was weighted within race (White, non-Hispanic; Black, non-Hispanic; Hispanic; and Asian) to match population estimates. Benchmark distributions were derived from 2021 Current Population Survey (CPS) data. Although the LGBT+ sample in this survey is not weighted separately to match population benchmarks, the full sample is. Comparisons to the available demographic data for the LGBT population from the 2021 Behavioral Risk Factor Surveillance System (BRFSS) found the demographics from our sample closely align with the federal data source.
Margin of Sampling Error
The margin of sampling error, including the design effect for subgroups, is presented in Table 1 below. It is important to remember that the sampling fluctuations captured in the margin of error are only one possible source of error in a survey estimate and there may be other unmeasured error in this or any other survey.
The KFF Women’s Health Survey sample includes people of all genders; however, our sample design is more heavily focused on women. While our survey weights take this gender imbalance into account and we use additional data control measures to ensure the data we present are as reliable and as representative of the population as possible, some data points for certain subgroups with larger margins of error may be more heavily weighted by women than men. Caution should be exercised in interpreting findings among LGBT+ subpopulations due to smaller sample sizes and larger margins of error. Our issue briefs do not present data for subgroups where data limitations precluded us from developing reliable estimates.
STATISTICAL SIGNIFICANCE
All statistical tests are performed at the .05 confidence level. Statistical tests for a given subgroup are tested against the reference group (Ref.) unless otherwise indicated. For example, White is the standard reference for race/ethnicity comparisons and private insurance is the standard reference for types of insurance coverage. Some breakouts by subsets have a large standard error, meaning that sometimes even large differences between estimates are not statistically different.
See the full 2022 KFF Women’s Health Survey methodology for more details. The full survey instrument is available upon request.
