Maryland’s Money Follows the Person Demonstration: Support Transitions Through Enhanced Services and Technology
MFP Program Features in Maryland
Outreach and Enrollment
Maryland utilizes several statewide outreach efforts for its MFP program, including peer outreach and support, peer mentoring, options counseling, and marketing materials, described below. State officials noted that the number of HCBS waiver applicants has increased tremendously as a result of the outreach, options counseling, and application assistance services available through MFP.
Peer Outreach and Mentoring: Maryland uses peers (individuals with a disability or with non-professional life experience with Medicaid LTSS) to provide outreach to NF residents and others, such as facility social workers, nursing staff, family, administrators, and resident councils. Peers have an ongoing presence in NFs and are encouraged to share their personal experiences with community living and mentor residents throughout the decision-making and transition process. Once a resident indicates he or she is interested in learning more about community-based options, peers make referrals for options counseling and follow up via the LTSS web-based tracking system (described below). At the request of a resident, the peer will maintain the relationship throughout the HCBS waiver application process. The state agency for people with disabilities and its peer support contractors are responsible for recruiting and training peers, monitoring peers’ activities, and collecting and reporting data.
Options Counseling: In addition to the peer outreach and support program, Maryland offers options counseling services to NF residents through its MFP demonstration. The Area Agencies on Aging (AAAs) and Centers for Independent Living (CILs) receive referrals from residents and their families, guardians, and advocates, peer outreach workers, facility staff, ombudsman, and the Minimum Data Set (MDS) 3.0 Section Q assessments1 and then provide in-depth education on the services and supports available in the community. For Medicaid beneficiaries who desire additional help, options counseling can include HCBS waiver or CFC application assistance. Once a resident applies for HCBS waiver or CFC services, a supports planner2 (a case manager from an AAA or non-profit HCBS provider) coordinates the medical and financial eligibility determination process, starts the person-centered planning process, and if needed, connects with the housing specialist within their agency or the MFP housing specialist.
Marketing Materials: In Maryland, MFP outreach methods have included marketing materials developed by the state, letters to facility administrators, educational articles in industry publications such as the Health Facilities Association of Maryland and LifeSpan Network newsletters, and trainings for HCBS providers. Marketing has been targeted to AAAs, CILs, local health departments, social service departments, advocacy groups, NF trade associations, county/senior expos, local/state/national conferences, senior provider networks, and housing organizations. Outreach materials illustrate the experiences of individuals with physical disabilities with transitioning from an institutional setting and living successfully in the community. Other state-generated materials provide information on services and supports available through HCBS waivers, basic financial and functional eligibility criteria, and guidance on how to request additional information and application assistance.3 MFP staff frequently provide presentations to local and statewide groups about MFP-specific initiatives, as well as broader rebalancing reform efforts.
Key MFP Services and Supports
Home and Community-Based State Plan and Waiver Services: Once enrolled in MFP, beneficiaries can access HCBS through the Medicaid state plan benefits package and/or one of Maryland’s Section 1915(c) waivers for seniors and people with physical disabilities, people with brain injuries, and people with intellectual/developmental disabilities. As noted above, although HCBS waiver enrollment slots are limited, Maryland’s MFI state law allows Medicaid beneficiaries residing in an institution to apply to receive HCBS through a waiver, regardless of waiver enrollment caps or waiting lists. Once enrolled in a HCBS waiver, beneficiaries may access any of the services in the waiver’s benefits package as well as the services available through the state plan benefits package, as medically necessary. Common HCBS that Maryland’s MFP participants may receive include personal assistance, supports planning, assistive technology, environmental accessibility modifications, medical day care, personal emergency response systems, and transition services.
MFP Demonstration and Supplemental Services: In addition, MFP demonstration and supplemental services are available during beneficiaries’ 365-day participation period. MFP demonstration services are HCBS that are not available to non-MFP participants; demonstration services receive enhanced federal matching funds. Maryland’s MFP participants receive post-transition peer mentoring as a demonstration service.
Maryland’s MFP supplemental services are one-time services that are not otherwise allowable, may not be long-term in nature, and are designed to help support the participant’s initial transition; supplemental services are reimbursed at the state’s regular federal matching rate. Maryland offers flexible funds (up to $700 per enrollee) as an MFP supplemental service, which can be used to cover an initial supply of groceries, security deposits, rental application fees, and/or other needed goods and services that could not otherwise be funded by Medicaid.
Stakeholders and state officials identified flexible funds and transitional case management as two critical services that contribute to the success of the Maryland’s demonstration. Prior to funding transitional case management as a waiver service, MFP paid for the service as a demonstration service to applicants who did not otherwise have access to this service.
New Home and Community-Based Waiver Services That Originated in MFP: Maryland’s MFP program was the catalyst for adding services to two of the state’s existing Section 1915(c) waivers. For example, transitional case management services (which include housing assistance) previously was covered as a demonstration service only for MFP participants transitioning to the HCBS waiver for seniors, and in 2012, was added to the waiver benefits package. In addition, as a result of recommendations made by the stakeholder advisory group, environmental assessments, nutritionist/dietitian services, and home delivered meals were added to the HCBS waiver benefits package for people with physical disabilities and transition services were added to the waiver for seniors in 2009. The added services are now available to all participants in the HCBS waiver for seniors and people with physical disabilities, regardless of MFP enrollment status.
Beneficiary Self-Direction of HCBS: Nearly all MFP demonstrations nationwide promote beneficiary self-direction of services and supports as an alternative to the provider management service delivery model. Self-direction promotes personal choice and allows the beneficiary to control a service budget and/or the selection, training, and dismissal of providers. Nationally, about 19 percent of MFP participants are enrolled in a self-directed model.4 Currently, there are limited options for beneficiary self-direction of HCBS in Maryland; only MFP participants who receive services through one of the state’s HCBS waivers have the ability to self-direct their services, but none currently exercise this option. The state plans to expand access to self-direction for beneficiaries receiving attendant care services and supports through the CFC state plan option in 2014 and will offer voluntary self-direction training to these beneficiaries. More opportunities for self-direction now exist under the new Home and Community-based Options (CO) Waiver (which combined the Living at Home Waiver (LAH) and the Waiver for Older Adults (WOA)), e.g., setting rates for personal assistant services, taking a more active role in hiring and firing workers, acting as one’s own supports planner/case manager.
Housing Assistance
Because finding accessible affordable housing is often the biggest challenge to transitioning to the community, Maryland provides housing assistance to MFP participants through a number of strategies:
Housing Location Assistance as a Home and Community-Based Waiver Service: One of the major components of transitional case management is the provision of housing assistance. Supports planners/case managers provide information about types of housing options, the availability of housing, and the housing subsidy systems, and will also provide intensive support to complete applications, acquire needed documentation, and secure housing. Housing assistance may also include opportunities for MFP participants to visit different housing options using their supplemental service funds. Housing assistance will be available to residents of state residential centers who indicate a preference for independent community housing instead of an Alternative Living Unit and will be provided by their Service Coordinators. Through MFP, DHMH maintains four housing specialists who accept referrals from transitional case managers and provide enhanced housing assistance when the case manager is unable to secure community housing. These specialists are also tasked with establishing and maintaining relationships with local public housing authorities (PHAs) to advocate for additional resources and providing training to MFP partners.
Expansion of Subsidized Community Housing: MFP’s housing specialists participate in statewide housing policy development. For example, in February 2011, MFP staff worked with partners to help secure 112 federal category 2 Housing Choice vouchers from the U.S. Department of Housing and Urban Development (HUD) for non-elderly individuals with disabilities transitioning from institutions. Since then, all of these vouchers have been awarded to beneficiaries.
Additionally, in February 2013, Maryland received $10.9 million in grant funding from HUD for a Section 811 Project-based Rental Assistance program (PRA). The Maryland Partnership for Affordable Housing (MPAH), a grant project obtained through a Centers for Medicare and Medicaid Services (CMS)-sponsored Real Choice System Change grant, enabled MPAH to successfully create an inter-agency agreement between the state housing, Medicaid, and disability agencies and together apply for the Section 811 PRA grant. Maryland’s Section 811 PRA demonstration will support 150 units for the non-elderly persons with disabilities. To underscore their commitment to the goals of Maryland’s Section 811 demonstration, local PHAs committed an additional 102 vouchers or rental units for MFP participants with disabilities age 62 or younger. Maryland’s MFP housing director works with state and local partners to develop and implement the PRA program, while MPAH develops the infrastructure required by the PRA demonstration, including coordination of services and supports between agencies and an efficient and timely unit referral system.
Maryland’s MFP grant also funds the following activities to support the Section 811 PRA demonstration:
- Person-Centered Planning Training – MFP funded this training, with an emphasis on housing, for case managers, service providers, and other professionals.
- Housing Subsidies – One million dollars in MFP funds are being held in trust by the state housing agency to fund housing subsidies for demonstration participants for a period of up to six months if the PRA demonstration is not renewed and housing funding is no longer available from HUD.
- Support to Help Beneficiaries Maintain Community Housing – The MFP housing director and housing specialists will be responsible for training and supporting case managers who will help PRA beneficiaries navigate landlord/tenant issues and maintain stable community housing.
- Streamlining Eligibility Determinations – The state Medicaid agency is contracting with a non-profit to administer the PRA demonstration’s web-based eligibility and unit identification system.
Staff Dedicated to Housing for People with Disabilities: Maryland’s MFP program currently funds two positions through an agreement with the state agency for people with disabilities, a housing specialist and an interagency housing liaison. This housing specialist administers the MPAH program described above, provides technical assistance to waiver supports planners/case managers and landlords participating in the PRA Section 811 demonstration, maintains housing waiting lists, and manages waiting list preferences and the selection process. The housing specialist also is the state disability agency’s liaison to other state agencies, advocacy groups, stakeholders, and the public for housing outreach initiatives related to MFP.
In addition, the state disability agency housing specialist administers the Weinberg Affordable Housing program. Since 2011, the state housing, Medicaid and disability agencies have had a joint venture with the Weinberg Foundation to work together to finance affordable, quality, independent, and integrated housing opportunities for people with disabilities and very low incomes. To qualify for these units, participants must be between the ages of 18-61 at the time of occupancy, receiving Supplemental Security Income or Social Security Disability Insurance with income between 15-30 percent of the area’s median income, and willing to live in the identified project location.
The interagency housing liaison coordinates special MFP projects related to housing between the state Medicaid and disability agencies, such as the MFP bridge subsidy5 and transit-oriented development and sustainable community planning initiatives to create affordable accessible housing for people with disabilities transitioning out of NFs. The liaison also is responsible for developing and maintaining key relationships with affordable housing stakeholders including PHAs, developers, and local municipalities.
State Staffing and Key Partnerships
Maryland’s MFP program has 13 full-time staff members within the state’s Medicaid agency: a project director (who also currently oversees the state’s BIP implementation); an associate project director; a housing director; three housing specialists; a data specialist; a policy analyst/behavioral health specialist (who also works on implementing the state’s CFC state plan option and acts as the MFP liaison with state and local mental health agencies); three staff members who focus on transitioning individuals with developmental disabilities and work closely with the state’s agency for people with developmental disabilities; a finance specialist; and an Aging and Disability Resource Center (ADRC) specialist. All of these positions are fully funded by federal MFP administrative dollars. Key partnerships with Maryland’s MFP program include:
ADRCs – Like other states nationally, Maryland has received ADRC funding from the federal Administration for Community Living and CMS to develop a program to streamline access to information about LTSS, especially HCBS options. Maryland’s program, called Maryland Access Point (MAP), began in 2004,6 and is led by the state department of aging; twenty local MAP sites make up the statewide “no wrong door/single entry point” information and referral system.7 MAP staff assist individuals with navigating the state’s LTSS system and application processes and make referrals to service providers.
Collaborations between the state Medicaid agency and the MAP program have expanded significantly as a result of MFP. The MAP program receives MFP funding to assist with MFP functions and to support staffing, marketing, and training to expand the MAP program. MFP and state Medicaid agency staff participate on steering committees for all MAP initiatives, such as the Person Centered Hospital Discharge Program and the Community Options Counseling Program.
AAAs – AAAs are the lead agency for the MAP sites (with the exception of the Worcester County Health Department) and have a key role in developing partnerships with other local agencies such as CILs, local social services departments, county health departments, and public housing authorities, and help with options counseling and application assistance for NF residents pursuing community LTSS options. Outside of the MAP sites, AAAs also provide supports planning for the CO Waiver.
CILs – CILs are a state-mandated MAP partner and provide peer outreach and ongoing supports to NF residents. CILs also provide peer mentoring to NF residents through, for example, community integration activities, during the final stages of the transition process and post-transition. CILs also partner with the AAAs in providing options counseling.
State Housing Financing Agency and Local Public Housing Authorities – MFP staff are working to strengthen relationships with the state housing financing agency and the local PHAs, as described above. State officials report that continued education and advocacy are the key steps towards an increased supply of safe, affordable, and accessible housing for people with LTSS needs in Maryland.
Long-Term Care Ombudsman– The state Long-Term Care Ombudsman programs are available as a resource for NF residents and their relatives and advocates. Ombudsmen investigate complaints, provide mediation, and assist with residents’ issues concerning rights, payments, guardianship, and NF placement. Ombudsmen are also knowledgeable about transition services and about Medicaid HCBS and they refer people to MFP that express a desire to return to the community.
MFP Stakeholder Workgroup – This workgroup meets bi-monthly with attendance ranging from 34 to 50 beneficiaries, agency staff, providers, and advocates from the aging and disability communities. This group provides input on demonstration activities and priorities for rebalancing investment.
State Departments of Aging and Disabilities – These state agencies administer the options counseling and peer support programs for MFP beneficiaries, respectively, and provide additional quality oversight and monitoring.
Maryland Disability Law Center – This is Maryland’s protection and advocacy agency for people with disabilities. They provide input on how MFP activities impact NF residents and make recommendations to improve the process.
State University Systems – The state Medicaid agency funds the University of Baltimore’s Schaefer Center to administer the Quality of Life (QoL) Survey to MFP participants and The Hilltop Institute at the University of Maryland, Baltimore County to provide ongoing IT support, data management, and analysis to assist with CMS reporting requirements and provide analysis to assist state staff in the policy making process. Hilltop also developed Maryland’s initial web-based MFP tracking system (described below).
Quality and Evaluation
QoL Survey: As noted above, Maryland administers the CMS QoL survey to MFP participants. The survey is given to participants during three specific timeframes: prior to discharge from the institution, twelve months post discharge date, and twenty-four months post discharge date.
Web-Based Tracking System: As noted above, Maryland uses a web-based system to track potential and enrolled MFP participants from initial contact through transition. The tracking system is accessible by peer outreach contractors, options counselors at the AAAs and CILs, waiver case managers, and the various state agencies involved in MFP. The system initially was built to track the QoL survey administration and assist state staff in monitoring contractor activities (such as peer outreach and options counseling), the number of application assistance referrals, and the administration of flexible funds (an MFP supplemental service).
The tracking system combines administrative data from the state’s Medicaid Management Information System, MDS 3.0 nursing home assessments, and other data sources to help the MFP program director and staff appropriately identify specific characteristics associated with successful or unsuccessful transitioning and promote person-center transition planning. In 2013, the state’s multiple web-based Medicaid LTSS tracking systems were integrated into one system. Maryland’s medical assessment tool and new time-keeping system for attendant care providers also were added. A reportable events module went live in 2014, and there are future plans to add a client portal and include tracking capabilities for other community-based supports such as CFC.
In addition to tracking associated specifically with MFP, each of the Section 1915(c) waivers in which MFP participants may enroll has a comprehensive quality management system that includes emergency back-up systems and incident reporting and management strategies.
Transition Progress
As of March 2014, 1,931 people have transitioned to the community through Maryland’s MFP program (Figure 1). Seniors and people with physical disabilities are the target groups most likely to transition as MFP participants. The average age of an MFP participant is 61 years old. State officials report that Maryland is on pace with its annual transition goals and expect the MFP enrollment rate to stay the same in the year ahead. The oldest beneficiary to transition via MFP was 106 and the youngest was 19.
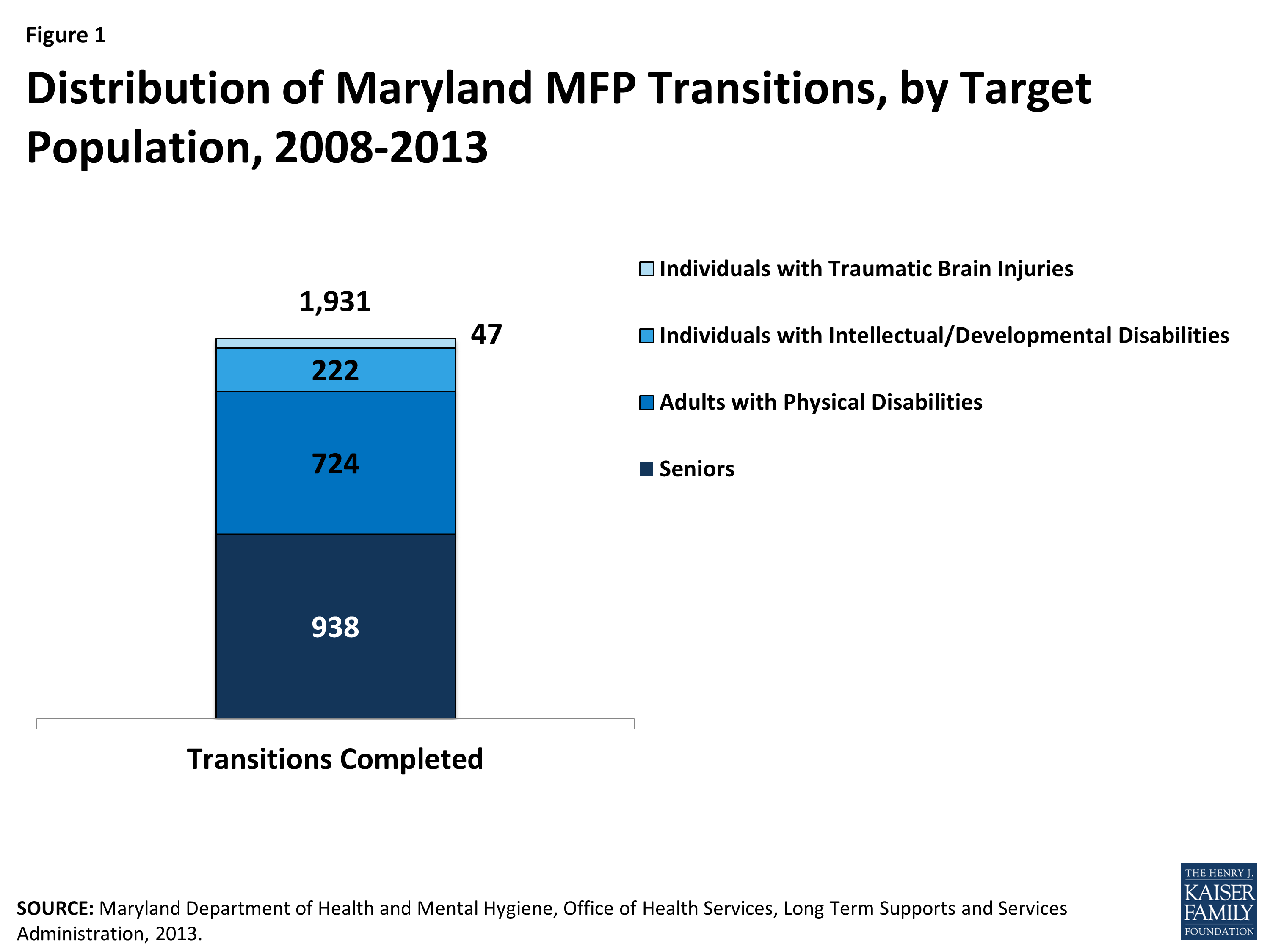
Figure 1: Distribution of Maryland MFP Transitions, by Target Population, 2008-2013
On average, it cost $4,618 per month to serve an MFP participant in the community in calendar year (CY) 2011 (Figure 2). The per participant per month cost of serving seniors in Maryland’s HCBS waiver ($3,333) was lower than the cost of serving adults with physical disabilities in in Maryland’s HCBS waiver ($5,904). Across all MFP populations, the average costs are comparable to other Medicaid HCBS beneficiary expenditures across the state and are lower than the average costs of serving Medicaid beneficiaries in institutional settings ($6,082). For individuals who enrolled in MFP in CY 2011, average monthly Medicaid expenditures decreased after transition across all waiver programs, except for the Older Adults waiver program (expenditures remained the same) (Figure 3). Per member per month Medicaid HCBS expenditures were highest among traumatic brain injury (TBI) waiver participants ($16,891).8
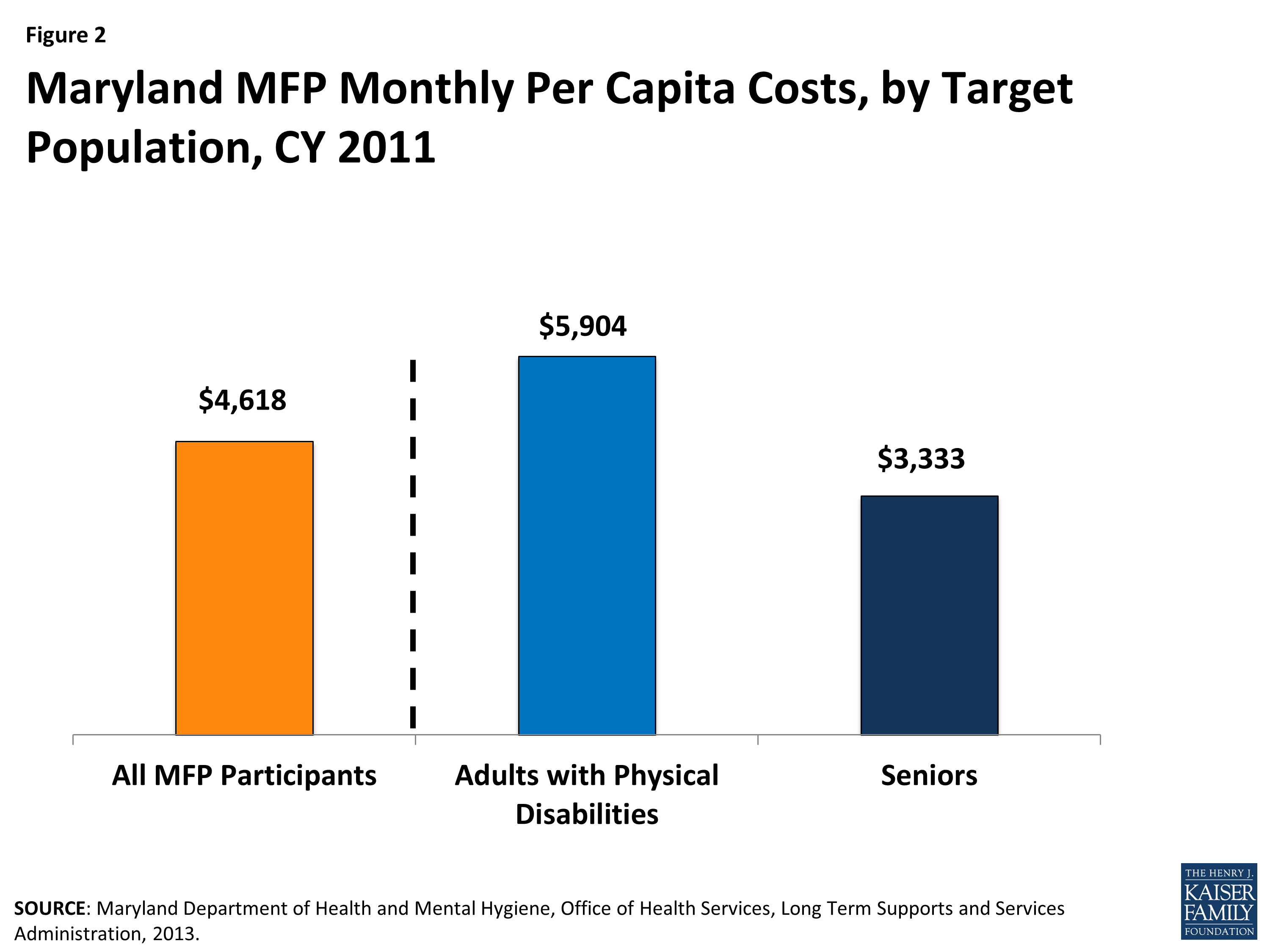
Figure 2: Maryland MFP Monthly Per Capita Costs, by Target Population, CY 2011

Figure 3: Pre- and Post-Transition MFP Participant Monthly Costs for All Medicaid Expenditures, by Waiver Program, CY 2011 Transitions
On average, Maryland’s MFP participants took 6 months to transition to the community. This compares to a national average of 3.5 months.9 Under MFP, there are three types of community-based residences in which MFP participants can choose to reside: a house owned or leased by the beneficiary (or a relative), an apartment leased by the beneficiary, or a group home in which no more than four unrelated individuals reside.10 In Maryland, senior MFP participants most often transition to a house whereas individuals with physical disabilities most often transition to an apartment. Most individuals with intellectual/developmental disabilities and individuals with TBI transitioned to a group home.
About five percent of Maryland’s MFP participants have been reinstitutionalized either in a hospital, NF, or ICF/ID. Nationally, states reported an average reinstitutionalization rate of 11 percent across all MFP populations.11
MFP and ACA LTSS Options
MFP contributes to ongoing LTSS rebalancing efforts in Maryland as well as supports the research, development, and implementation of the ACA’s new and expanded opportunities to increase access to Medicaid HCBS. When the state needed to revise its MFP Operational Protocol in 2011, following the ACA’s extension of the MFP demonstration, Maryland engaged an active stakeholder group (comprised of consumers, advocates, consumer protection agencies, Legal Aid, AAAs, CILs, state agencies, case management providers, and NF associations) to solicit ideas about potential changes to MFP. The group decided MFP should support rebalancing initiatives by reinvesting savings into CFC, BIP, implementation of a universal assessment tool, and MAP sites. As of March 2014 Maryland had implemented the BIP program, a Section 1915(k) CFC state plan option for attendant care services and supports with enhanced federal funding, and the new state plan option to provide health home services. Alongside the CFC implementation, the two Section 1915(c) waivers that serve most MFP participants (i.e., LAH and WOA) were combined to create the new CO Waiver as mentioned above. All services allowable under CFC were removed from the CO Waiver and covered through the state plan option. These state plan services are available to CO participants that live in a community-based setting, including MFP participants.
MFP and BIP: The state utilized lessons learned from MFP when applying for BIP, a new ACA option that provides financial incentives to states that implement certain structural reforms to increase access to community-based LTSS. BIP requires states to create a conflict-free case management system, develop a no wrong door/single entry point system, and utilize a statewide core standardized assessment. States, such as Maryland, that spent 25 to 50 percent of their fiscal year 2009 Medicaid LTSS dollars on community-based LTSS are eligible to receive a two percent increase in their federal matching rate through September 2015 by participating in BIP.
Maryland’s MFP demonstration helped finance the structural changes required under BIP. In order to do this, the MFP Operational Protocol was revised in January 2012 to explicitly define programs and activities that help Maryland develop a more balanced system of LTSS in home or community-based settings, such as research and implementation of a core standardized assessment (the interRAI) and staff funding for MAP sites that serve as Maryland’s Single Entry Point/No Wrong Door system. Maryland was approved for its BIP grant in March 2012.
MFP and CFC: The ACA established CFC, a new Medicaid state plan option that allows states to provide expanded statewide home and community-based attendant supports and other waiver-like services to individuals who require an institutional level of care. States taking up this option receive a permanent six percent increase in their federal matching rate for CFC services. CFC is designed to assist individuals with activities of daily living, instrumental activities of daily living, and health-related tasks and with acquiring, maintaining, and enhancing their own skills to accomplish these tasks. CFC services include “self-direction” training; backup systems; and at state option, other services and supports linked to an assessed need or goal in the person-centered service plan.
Maryland implemented the CFC option in January 2014.12 The state has utilized CFC to consolidate, under one program, personal assistance services that were previously available as three separate programs: the state plan personal care services benefit, the Section 1915(c) waiver for persons with physical disabilities, and the Section 1915(c) waiver for seniors. By consolidating personal assistance services under one program, the state is able to standardize rates, providers, and regulations and to provide participants with increased self-direction opportunities. The state reports that initial CFC start-up costs such as staffing, technology, training, and outreach will be financed using MFP and BIP funding, and CFC will be sustained through the six percent enhanced federal match on CFC services.13
Looking Ahead
The goal of Maryland’s MFP demonstration is to encourage LTSS rebalancing by improving the transition process, increasing outreach, and decreasing barriers. To accomplish this, Maryland uses federal MFP funding to provide peer mentoring services, options counseling, and application assistance to NF residents, improve information technology, offer housing assistance, provide flexible transition funds, and add services to existing HCBS waivers. In addition, the state leveraged MFP funding to accelerate LTSS rebalancing efforts through new and expanded ACA LTSS options. MFP has helped finance the structural changes required in BIP and helped to fund the start-up costs associated with the CFC state plan option. Additional funding has been approved in Maryland’s MFP Operational Protocol to support specific rebalancing efforts, including housing partnerships with the state agency for people with disabilities, training initiatives, a Bridge Subsidy Rental Assistance program, provider registry, and enhanced peer support for ICF/ID residents who wish to transition to the community.14
Maryland officials report housing as the number one challenge facing LTSS beneficiaries who want to transition from institutions to the community. With Maryland’s housing costs among the highest in the nation, finding affordable housing can be difficult for potential MFP participants. MFP staff continue to be concerned that participants entering a NF have given up their previous housing, making it harder to transition back into the community. Therefore, assistance with locating housing, provided through the supports planners or MFP housing staff, and ongoing training to develop housing expertise among waiver case managers and MAP partners continue to be a focus of Maryland’s MFP program. At a systems level, MFP will continue to support collaborations with developers, landlords, property managers, and the state and local housing authorities to advocate for safe, affordable, accessible, and integrated housing for persons with LTSS needs. Other ongoing efforts include continuing to improve how BIP and MFP work together (through funding structural changes and the expansion of services); strengthening MAP sites through BIP funding; planning for program sustainability; standardizing services and supports, provider requirements, and rates across the various HCBS waiver programs; supporting NF diversion programs; and determining how the January 2014 definition of home and community-based setting affects Maryland’s CFC option and Section 1915(c) waivers.15
This Kaiser Commission on Medicaid and the Uninsured brief was prepared by Molly O’Malley Watts with Watts Health Policy Consulting and Erica L. Reaves and MaryBeth Musumeci from the Kaiser Family Foundation. Special thanks to Devon Mayer with the Maryland Department of Health and Mental Hygiene who contributed to the content and review of this case study.