Donor Government Assistance for Family Planning in 2013
Introduction
Access to family planning (FP) services has a significant impact on the health and wellbeing of women and girls, and on global health and development more broadly. Family planning – the ability of individuals and couples to determine their desired number of children as well as the timing of and spacing between births – can help prevent pregnancy-related health risks, reduce infant mortality, and help in the prevention of sexually transmitted diseases such as HIV/AIDS.1 Currently, it is estimated that more than 200 million women worldwide would like to delay or stop childbearing, but they do not have access to contraceptives.2
In July 2012, the U.K. Government and the Bill & Melinda Gates Foundation, in partnership with UNFPA, civil society organizations, developing countries, donor governments, the private sector, and multilateral organizations met at the London Summit on Family Planning (FP2020) and made commitments aimed at providing voluntary family planning services to an additional 120 million women and girls in developing countries by 2020. The London Summit built on prior efforts, such as the International Conference on Population and Development (ICPD) in 1994 and inclusion of family planning related goals under Millennium Development Goal (MDG) 5, and brought renewed attention to international efforts to support family planning programs in low- and middle-income countries. Additionally, the London Summit resulted in stated commitments totaling $2.6 billion in additional funding for family planning activities from all sources (donor governments, non-governmental organizations, philanthropies, multilateral organizations, and domestic resources).
While funding from all sources – domestic public and private spending, donor government bilateral assistance, multilateral organizations and private philanthropic (see Box 1) – is needed to help fulfill international goals and commitments, donor governments provide a significant share of global funding for family planning services.3 Following the London Summit, the Kaiser Family Foundation conducted an analysis of donor government funding for family planning activities in 2012 to establish a FP funding baseline that could be used to track funding levels over time as well as specific donor government progress in meeting the London Summit on Family Planning commitments.
Box 1: Other Sources of Funding for FP in Low- & Middle-Income Countries
While this report focuses on donor governments, there are three other major funding streams for FP assistance: multilateral organizations, the private sector, and domestic resources.
Multilateral Organizations: Provide assistance for FP using pooled funds from member contributions and other means. The primary multilateral organization addressing FP is the United Nations Population Fund (UNFPA). Contributions to multilateral organizations are usually made by governments, but can be provided by private organizations and individuals, as in the case of UNFPA. Some multilateral organizations are designed to address specific issues (such as UNFPA, which also finances reproductive health and other population related activities); donor government contributions to UNFPA are highlighted as part of the donor government’s financing effort in this analysis. Donor government contributions to multilateral organizations that are not specifically designed to address population activities, but may include such activities within their broader portfolio (such as the World Bank), are not included in this analysis.
Private Sector: Foundations (charitable and corporate philanthropic organizations), corporations, faith-based organizations, and international non-governmental organizations (NGOs) provide support for FP activities in low- and middle-income countries not only in terms of funding, but through in-kind support; commodity donations; and co-investment strategies with government and other sectors.
Domestic Resources: Including both spending by country governments that also receive international assistance for FP and by households/individuals within these countries, represent a significant and critical part of the response.
This report provides donor government funding for family planning activities in 2013 compared to 2012 levels. It includes an analysis of funding provided by the 26 governments who were members of the OECD DAC in 2013 and had reported ODA totals to the DAC.4 Data were collected directly from ten donors, who represent approximately 98% of bilateral family planning funding, and are profiled in this report: Australia, Canada, Denmark, France, Germany, Netherlands, Norway, Sweden, the U.K., and the U.S. Data for the remaining DAC members was obtained from the OECD CRS. For purposes of this analysis, family planning services were defined to include the following activities as specified in the CRS: counseling; information, education and communication (IEC) activities; delivery of contraceptives; capacity building and training.5 Where bilateral family planning funding was included as part of broader reproductive and maternal health activities or other non-health-sector activities, we worked directly with donor governments to identify family planning specific amounts to the extent possible (see Methodology for more information).
Findings
Bilateral Assistance
In 2013, donor governments are estimated to have disbursed6 US$1,307.8 million in bilateral funding for family planning activities (see Table & Annex 1), an increase of $211.4 million (19%) above 2012 levels (US$1,096.4 million). This includes both actual funding amounts provided (e.g., cash transfers) as well as other types of transactions and activities (e.g., technical assistance) and products (e.g., commodities).
| Table: Donor Government Family Planning Disbursements, 2012-2013 (US$ millions) | ||||
| Country | 2012 | 2013 | ||
| Bilateral Disbursements | UNFPA – Core Contributions | Bilateral Disbursements | UNFPA – Core Contributions | |
| Australia | $43.2 | $14.9 | $39.5 | $15.6 |
| Canada | $41.5 | $17.4 | $45.6 | $16.0 |
| Denmark | $13.0 | $44.0 | $18.8 | $40.4 |
| France | $49.6 | $0.5 | $37.2 | $0.0 |
| Germany | $47.6 | $20.7 | $38.2 | $24.0 |
| Netherlands | $105.4 | $49.0 | $153.7 | $52.4 |
| Norway | $3.3 | $59.4 | $20.4 | $70.6 |
| Sweden | $41.2 | $66.3 | $50.4 | $65.8 |
| U.K. | $252.8 | $31.8 | $305.2 | $31.5 |
| U.S. | $485.0 | $30.2 | $585.0 | $28.9 |
| Other DAC Countries | $13.8 | $98.0 | $13.8 | $108.8 |
| Total | $1,096.4 | $432.2 | $1,307.8 | $454.0 |
Most donor governments profiled (7) (Canada, Denmark, Netherlands, Norway, Sweden, U.S., and U.K.) increased bilateral funding in 2013 (after exchange rate fluctuations are taken into account); one donor (Australia) remained essentially flat and two donors (France and Germany) decreased funding for family planning in 2013. Most of the overall increase was due to increases in funding by the U.S., the U.K., and the Netherlands.
The United States (US$585.0 million) was the largest bilateral donor in 2013 accounting for almost half (45%) of total bilateral assistance (see Figure 1). The U.K. (US$305.2 million, 23%) was the second largest bilateral donor followed by the Netherlands (US$153.7 million, 12%), Sweden (US$50.4 million, 4%), and Canada (US$45.6 million, 3%).
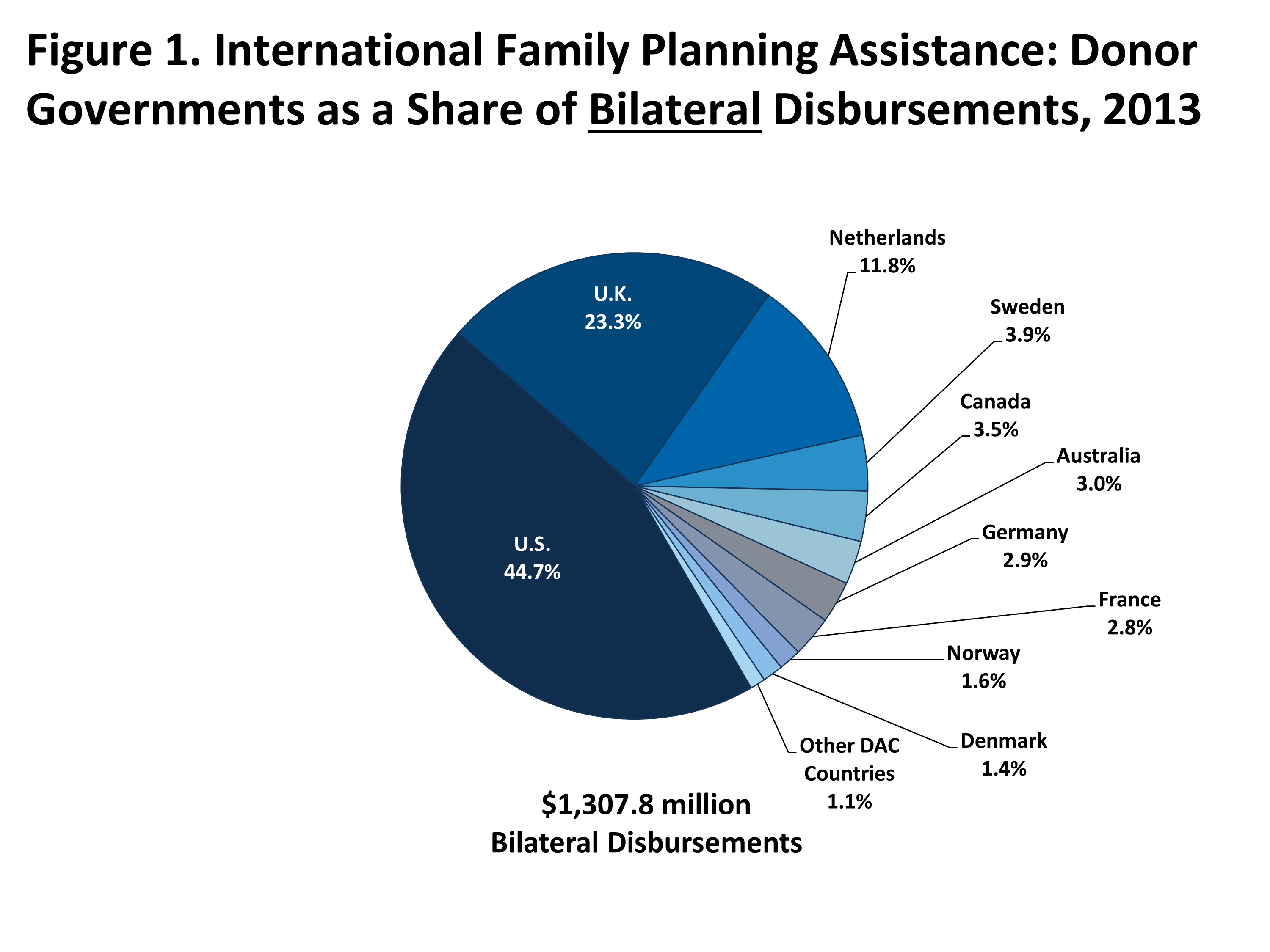
Figure 1: International Family Planning Assistance: Donor Governments as a Share of Bilateral Disbursements, 2013
Multilateral Assistance
While the majority of donor government assistance for family planning is provided bilaterally, donors also provide support for family planning activities through multilateral contributions to the United Nations Population Fund (UNFPA) (see Box 2).7
Box 2: United Nations Population Fund (UNFPA) Mission, Goals, & London Summit on Family Planning Commitment
- Achieve universal access to sexual and reproductive health (including family planning)
- Promoting reproductive rights;
- Reducing maternal mortality; and
- Accelerate progress on the ICPD agenda and MDG 5.
In 2013, donor governments provided US$454.0 million in core contributions to UNFPA, an increase of US$21.8 million (5%) above 2012 levels (US$432.2 million).8 UNFPA uses core contributions to support a variety of activities including family planning, but also in support of maternal and child health, education, human rights, and capacity building efforts.
Norway was the largest donor to UNFPA (US$70.6 million, 16%) and drove most of the increase in 2013. Sweden was the second largest donor (US$65.8 million, 14%) followed by the Netherlands (US$52.4 million, 12%), Denmark (US$40.4 million, 9%), the U.K. (US$31.5 million, 7%), and the U.S. (US$28.9 million, 6%) (see Figure 2).9
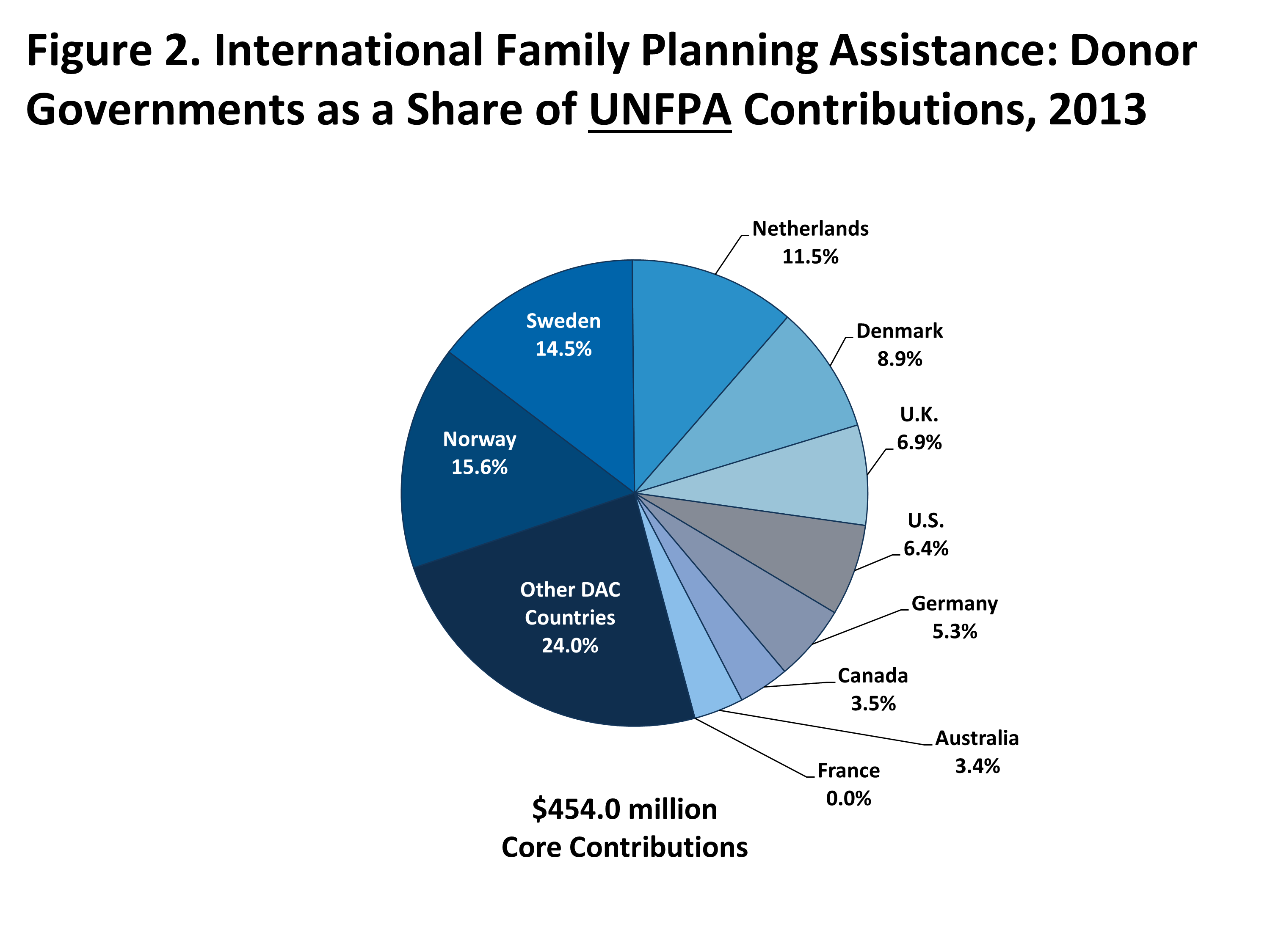
Figure 2: International Family Planning Assistance: Donor Governments as a Share of UNFPA Contributions, 2013
While it was not possible to calculate an adjusted “family planning share” of UNFPA’s 2013 budget and therefore to attribute a portion of each donor government’s UNFPA contribution to family planning-specific activities,10 it is important to note the relative balance between a donor’s core-contributions to UNFPA and its bilateral funding for family planning. For instance, three of the ten donor governments profiled provided a larger contribution to UNFPA than their bilateral disbursement: Denmark, Norway, & Sweden.
Progress Towards FP2020 Commitments
Eight of the donor governments surveyed directly made multi-year commitments at the FP2020 Summit in 2012 (see Appendix 2). While it is not possible to know what funding amounts would have been provided by donors in the absence of the Summit, data collected for 2012-2013 indicate that if current trends continue, all eight have made progress toward their stated commitments. Future analyses will continue to monitor funding disbursed towards these commitments.
Conclusion
Overall donor government funding for family planning activities increased in 2013, driven primarily by a subset of donors. In addition, preliminary data indicate that donors are making progress toward their FP2020 commitments. Looking ahead, however, it is not yet certain if these trends will continue, or if ongoing fiscal pressures will affect family planning budgets, as they have in some other sectors. It will therefore be important to continue tracking funding for family planning activities to assess progress towards addressing ongoing family planning needs in low- and middle-income countries.