A Closer Look at the Final Nursing Facility Rule and Which Facilities Might Meet New Staffing Requirements
On April 22, 2024, the Centers for Medicare and Medicaid Services (CMS) released a highly-anticipated final rule that creates new requirements for nurse staffing levels in nursing facilities, settings that provide medical and personal care services for 1.2 million Americans. CMS received nearly 50,000 comments on the proposed rule, ranging from comments that strongly supported the proposed standards to those that strongly opposed them. Among those comments, the nursing home industry suggested the rule was too strict and could lead to nursing facility closures, while resident and family advocates suggested the proposed standards were too weak to address well-documented concerns about substandard facility conditions, unattended residents, and poor patient care. The adequacy of staffing in nursing homes has been a longstanding issue, and the high mortality rate in nursing facilities during the COVID-19 pandemic highlighted and intensified the consequences of inadequate staffing levels.
This analysis discusses the provisions of the final rule, including changes made by the Administration from the proposed rule, and examines the percentage and characteristics of nursing facilities that currently meet the minimum staffing requirements in the final rule, which takes effect beginning in May 2026 for some facilities. The analysis estimates the percentage of facilities that could meet the requirements based on current staffing levels, examining the percent of facilities that meet all requirements—including 3.48 hours per resident day (HPRD), with 0.55 HPRD for RNs and 2.45 HPRD for nurse aides—and the percent that meet each requirement individually. In practice, facilities have several years to comply with the new requirements: the requirement to have overall staffing levels of 3.48 HPRD takes effect in 2026 for urban facilities and in 2027 for rural facilities, and the RN and nurse aide HPRD requirements take effect in 2027 for urban facilities and in 2029 for rural facilities. Facilities will also be allowed to apply for temporary exemptions from part or all of the final requirements if they meet certain conditions. The federal government estimates that a quarter of all 15,000 nursing facilities could end up obtaining an exemption.
This analysis uses Nursing Home Compare data from April 2024, which includes 14,448 nursing facilities (97% of all facilities, serving 1.18 million or 99% of all residents), and reflects staffing levels from October to December 2023. Due to data limitations, the analysis does not evaluate facilities’ ability to comply with other requirements in the final rule, including the requirement to always have a registered nurse on duty 24/7 or the ability to meet the new reporting and assessment requirements (see Methods).
Key takeaways include:
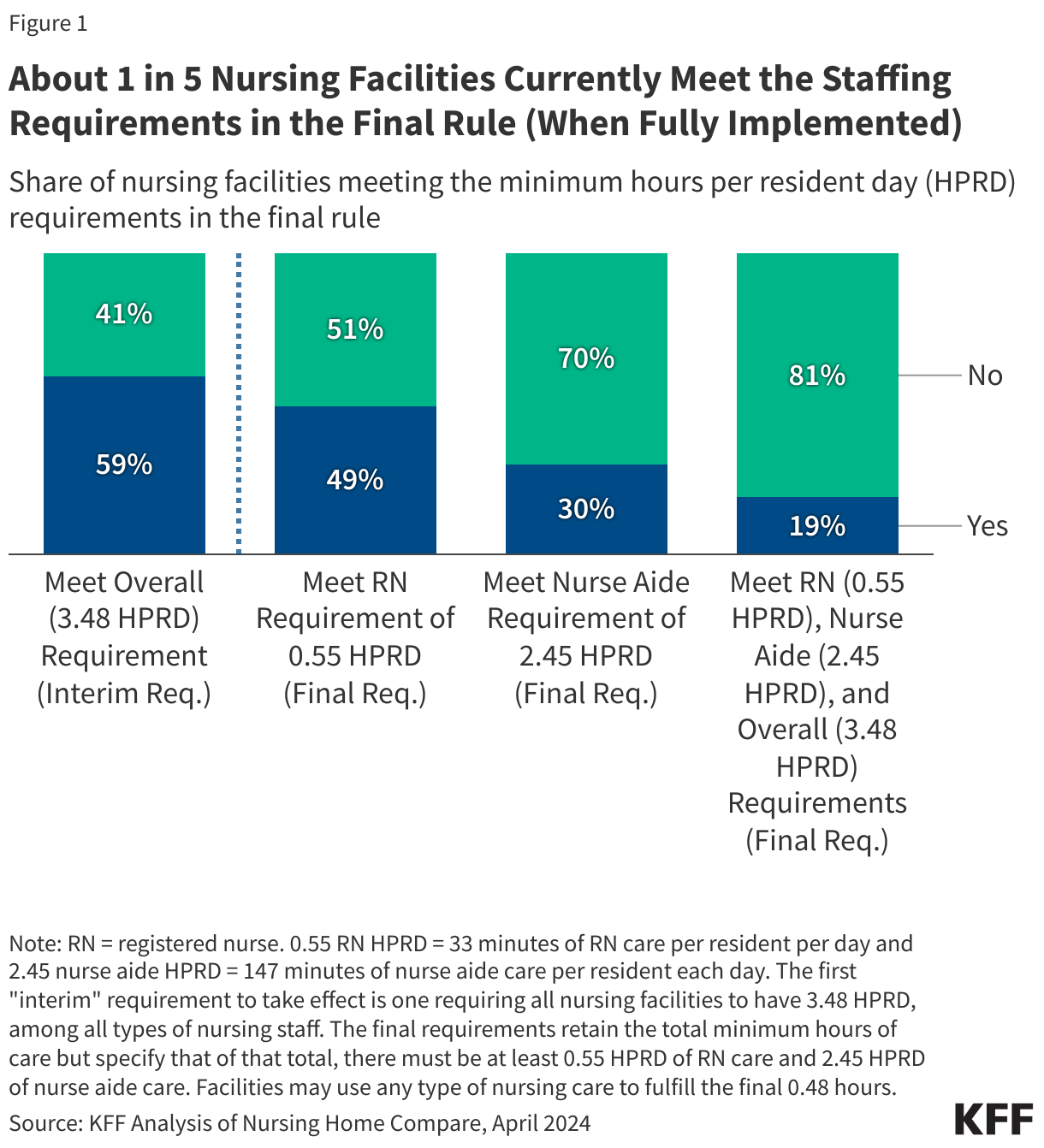
- Less than one in five (19%) of nursing facilities currently meet all three staffing minimums required in the final rule (Figure 1), which include 3.48 HPRD overall, 0.55 RN HPRD, and 2.45 NA HPRD. Nearly 60% of facilities would meet the interim requirement of an overall requirement of 3.48 HPRD.
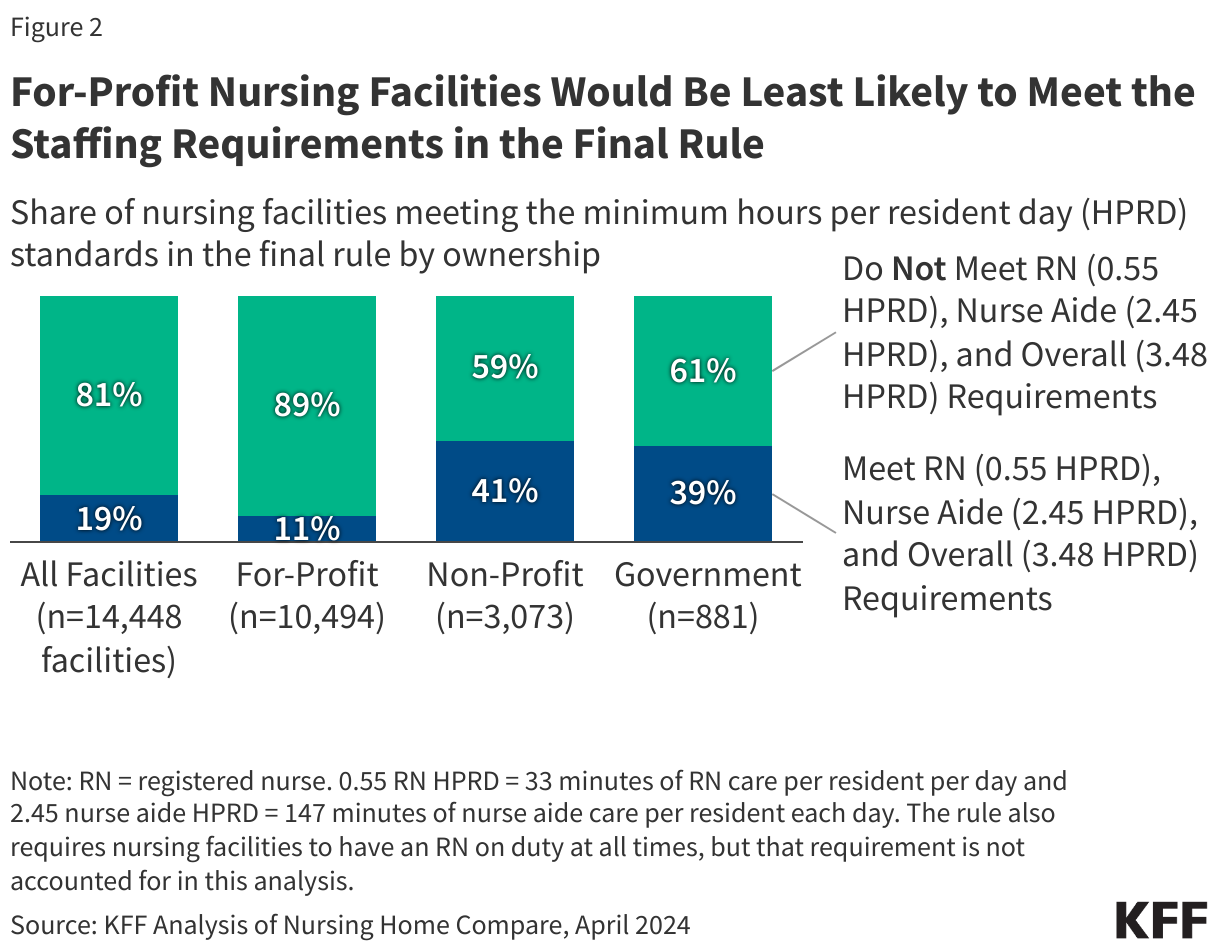
- A smaller share of for-profit facilities currently meet all requirements in the final rule than non-profit and government facilities (11% versus 41% and 39%, respectively).
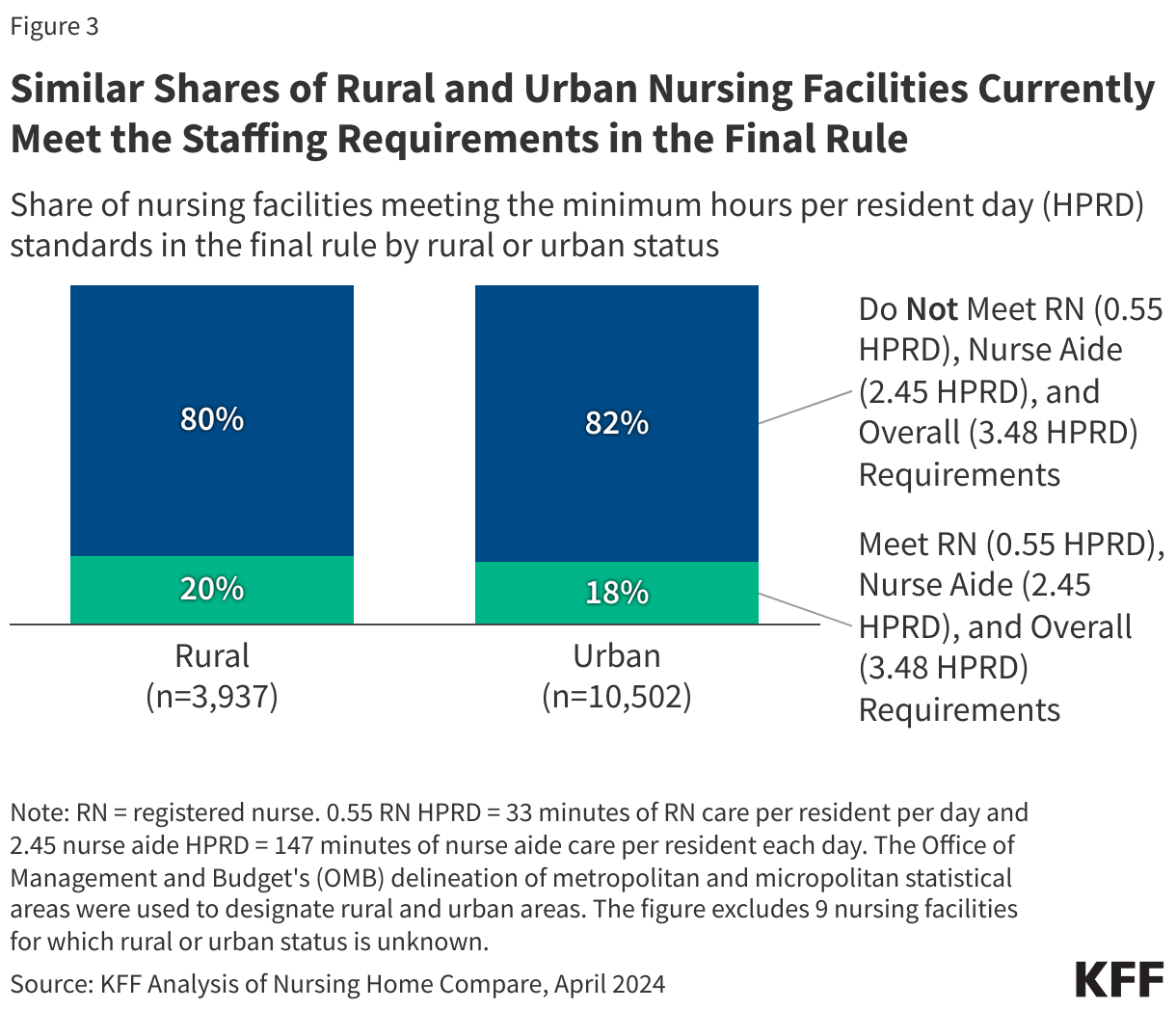
- Rural nursing homes are as likely as urban facilities to meet the final rule’s requirements based on current staffing levels, but rural facilities will have longer to comply with the new requirements.
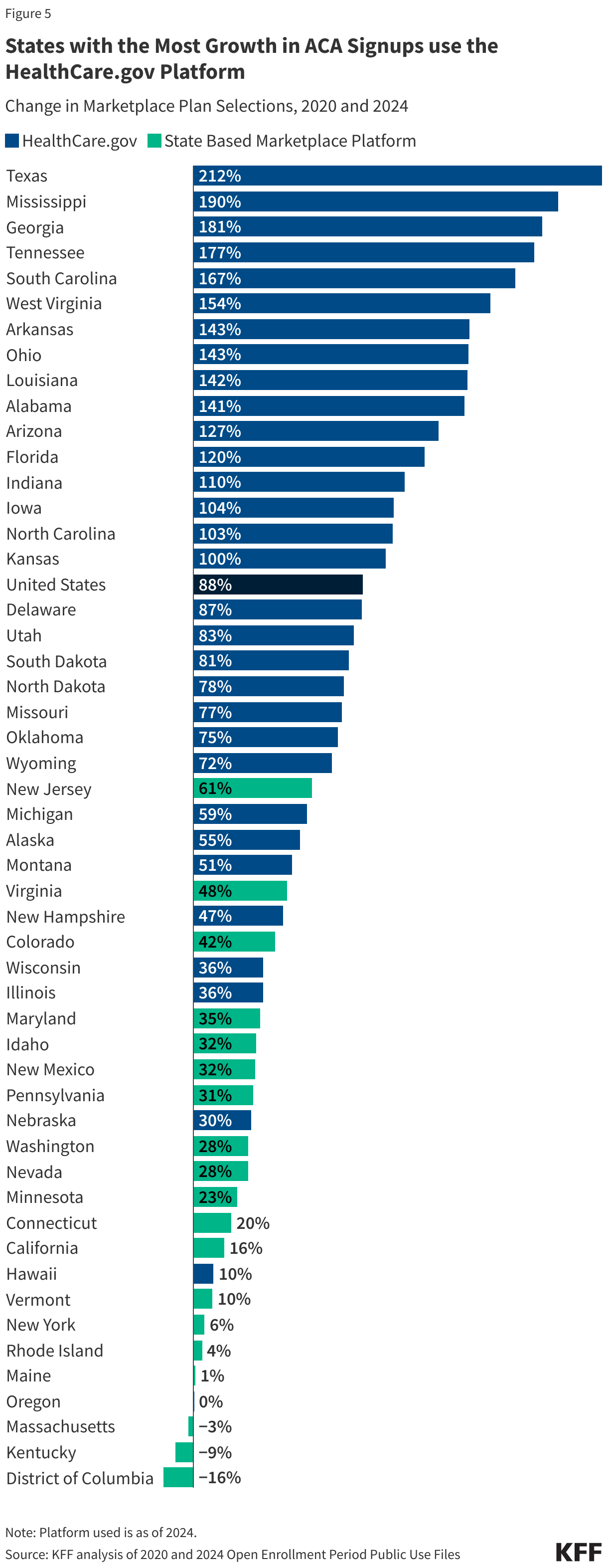
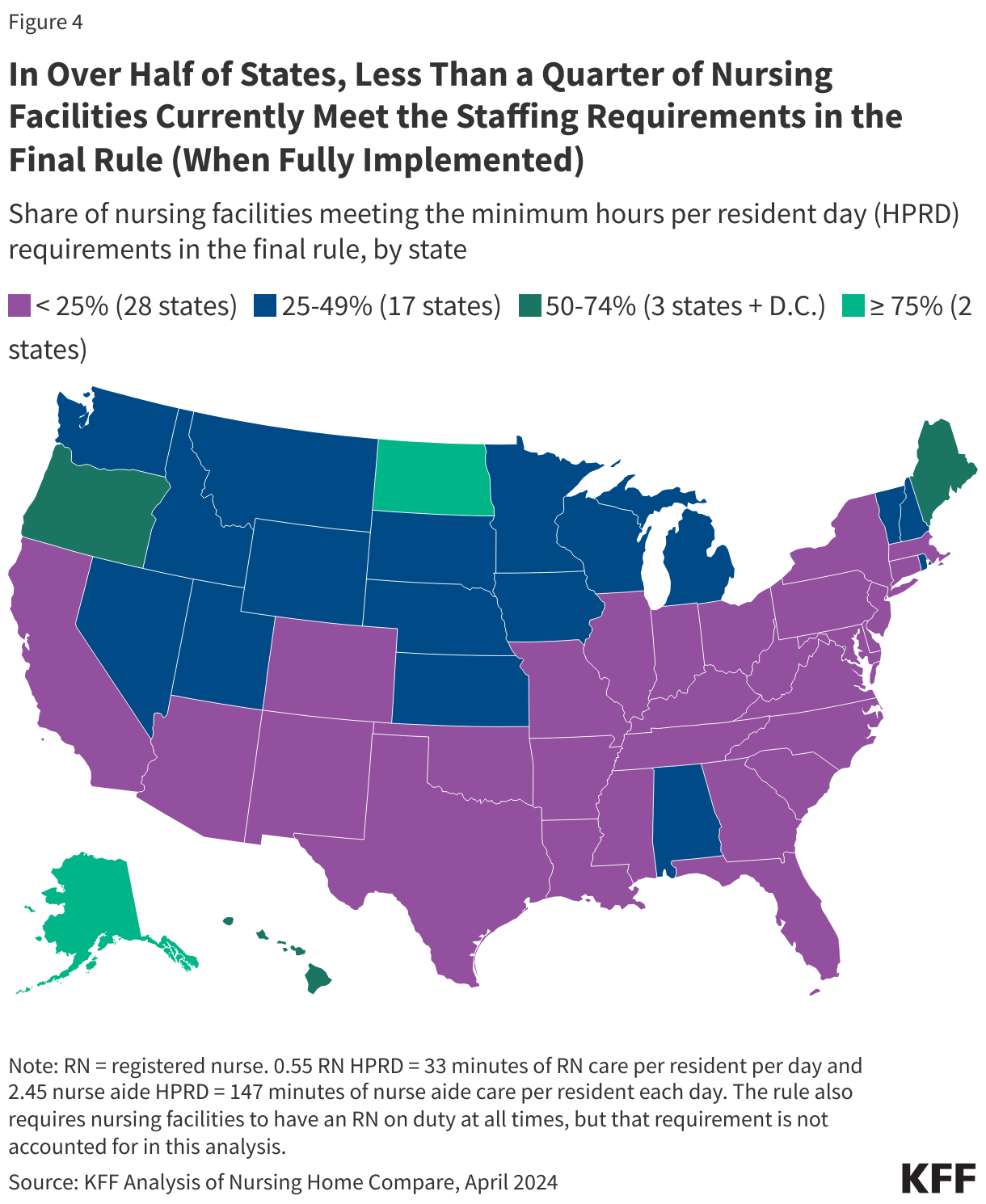
- In over half of states, fewer than one-quarter of facilities meet all three staffing minimums required in the final rule. The share of facilities that meet the requirements ranges from 5% or lower in four states (AR, TN, TX, and LA) to 50% or higher in five states and D.C. (AK, ND, ME, DC, HI, and OR).
What are the major requirements in the final rule and how do they differ from the proposed rule?
There are many provisions of the final rule, which will be phased in over time. The first phase requirements are the same as the proposed rule and include enhanced facility-wide staffing assessment requirements, which will strengthen existing requirements by requiring facilities to: assess the needs of each resident, include input from nursing facility staff and residents’ families or legal representatives, and develop a plan to meet required staffing levels given residents’ needs. The final rule adds language to the proposed rule to require the active participation of the nursing home leadership and management and direct care workers in completing the assessments. The first phase will take effect on August 8, 2024, 90 days after publication of the final rule (which is 30 more days than were provided in the proposed rule).
The second phase of implementation requires nursing facilities to have a registered nurse on duty 24 hours a day and 7 days a week (24/7), but the final rule also requires facilities to have at least 3.48 HPRD of nursing care. Like the proposed rule, the second phase would take effect 2 years after publication of the final rule for urban nursing facilities (May 2026) and 3 years after publication of the final rule for rural nursing facilities (May 2027). Unlike the proposed rule, nursing facilities may apply for a hardship exemption from the 24/7 requirement, which would allow them to have a registered nurse on duty for only 16 hours per day. See below for more details about how facilities may apply for a hardship exemption.
The final phase of implementation requires nursing facilities to have a minimum of 0.55 registered nurse (RN) and 2.45 nurse aide HPRD in addition to the overall 3.48 HPRD requirement. Facilities could fulfill the requirement of the additional 0.48 HPRD with any nursing staff type, including nurse aides, RNs, or licensed practical nurses (LPNs). The third phase would take effect 3 years after publication of the final rule for urban nursing facilities (May 2027) and 5 years after publication of the final rule for rural nursing facilities (May 2029). These requirements are unchanged from the proposed rule.
The final rule includes hardship exemptions that allow nursing facilities to maintain lower staffing levels, but includes additional requirements tied to those exemptions. Nursing facilities may apply for exemptions from any of the minimum staffing requirements if they are located in an area with workforce unavailability (defined as having a provider to population ratio that is at least 20% lower than the national average). The final rule eliminated a provision in the proposed rule that would have allowed nursing facilities to apply for an exemption if they were located at least 20 miles from the nearest nursing facility, regardless of workforce availability. Nursing facilities would also have to demonstrate good faith efforts to hire and retain staff and a financial commitment to staffing by reporting the total amount of money spent on direct care staff. Finally, facilities would be ineligible for an exemption if they had any staffing-related violations including a failure to submit required data, being identified as a Special Focus Facility (a federal designation provided to facilities with a history of serious quality issues – see Box 1), or having violations related to insufficient staffing.
Nursing facilities that receive hardship exemptions will be required to:
- Post a notice of its hardship exemption status in a “prominent and publicly viewable location,”
- Share information about its exemption status and the degree to which it is not in compliance with the staffing requirements to current and prospective residents, and
- Send a copy of the notice to a representative of the Office of the State Long-Term Care Ombudsman.
The final rule also notes that exemption information will be publicly available on Care Compare in an effort to provide transparency and provide additional information that consumers, families, and caregivers may use to compare nursing facilities in their area. The federal government estimates that a quarter of all 15,000 nursing facilities could end up obtaining exemptions for at least some of the requirements.
The final rule includes other requirements as part of a broader efforts to address quality and staffing in nursing facilities. Those requirements are nearly the same as in the proposed rule. The final rule:
- Requires state Medicaid agencies to report the percent of Medicaid payments for institutional long-term services and supports (LTSS) that are spent on compensation for direct care workers and support staff. This aligns with a similar requirement for home and community-based LTSS that was enumerated in the final rule on access to care in Medicaid in a broader effort to increase transparency.
- Eliminates a requirement from the proposed rule to report the data by type of delivery system (fee-for-service versus managed care) to reduce the administrative burden on states.
- Includes $75 million in financial incentives such as scholarships and tuition reimbursement for individuals to enter careers in nursing homes. CMS aims to balance the goal of establishing stronger staffing requirements against the practicalities of implementation and costs.
What share of nursing facilities currently meet minimum staffing requirements in the final rule?
KFF estimates that 19% of nursing facilities currently meet all three staffing hour minimums required in the final rule (3.48 HPRD overall, 0.55 RN HPRD, and 2.45 NA HPRD). (Figure 1). The interim requirement that nursing facilities must meet is 3.48 HPRD, among all types of nursing staff. The final requirements retain the total minimum hours of care but specify that of that total, there must be at least 0.55 HPRD of RN care and 2.45 HPRD of nurse aide care. Facilities may use any type of nursing care to fulfill the final 0.48 hours. Nearly 60% of facilities have staffing levels at least equal to the interim requirement of 3.48 HPRD, but fewer (19%) of facilities currently meet all staffing requirements, including the minimum number of hours of RN and nurse aide care that are required when the rule is fully implemented (49% and 30% respectively). Though higher shares of facilities meet the overall, RN, and nurse aide requirements individually, the share that meet all three requirements is substantially lower since facilities could meet one or two requirements without meeting the other(s). Facilities that need to hire new RNs to comply with the final rule may find it difficult to compete with hospitals, many of which are also trying to increase the number of RNs they employ. The rule estimates that to meet both the 24/7 RN and 0.55 RN HPRD requirements, facilities would need to hire about 16,000 RNs. To meet the 2.45 nurse aide HPRD requirements, CMS estimates that facilities would need to hire 35,306 nurse aides. CMS states that the existing survey, certification, and enforcement processes will be used to assess compliance, with more details to come.
Only 11% of for-profit nursing facilities currently meet all three staffing minimums required in the final rule compared with 41% of non-profit facilities and 39% of government facilities (Figure 2). There are approximately 10,500 for-profit nursing facilities (73% of all nursing facilities); 3,000 non-profit nursing facilities (21%); and 900 government-owned nursing facilities (6%). When looking at the ownership of facilities that meet the interim requirement of 3.48 HPRD requirement, fewer for-profit facilities would meet the 3.48 overall standard than non-profit and government facilities (52%, 79%, and 71%, respectively; data not shown). Similarly, for-profit facilities are less likely to meet the registered nurse and nurse aide requirements when compared with government and for-profit facilities (data not shown).
The percentage of nursing facilities that currently meet the final rule’s requirements are similar in rural and urban areas, but rural facilities will have longer to comply with the new requirements (Figure 3). In rural areas, 20% of nursing facilities have staffing levels that would meet the rule’s requirements compared to 18% in urban areas. Despite similar levels of current staffing, nursing facilities in urban areas will need to comply with all of the provisions in the final rule two years earlier than those in rural areas (May 2027 and May 2029 respectively). In the rule, CMS cites that “rural areas face a myriad of challenges ranging from worker housing shortages to severe transportation challenges for remote facilities that are unique to their location.” Both rural and urban facilities face challenges with hiring but perhaps for different reasons. Rural facilities may have difficulty finding staff because there are fewer available workers, while urban facilities may have difficulty because available workers have more low-wage jobs to choose from in urban areas. Despite those different challenges, staffing patterns in urban and rural facilities are remarkably similar (data not shown).
In over half of states, fewer than a quarter of facilities would meet all three HPRD provisions in the final rule (Figure 4). The five states with the most nursing facilities (Texas, California, Ohio, Florida, and Illinois) all fall into this category, skewing the national average down to 19%. In six states, over half of facilities would meet these provisions, and in the remaining 17 states, 25-49% of facilities would meet the provisions. Variation across the states reflects many factors including what percentage of facilities are for-profit, the availability of RNs and nurse aides in the state, and state requirements regarding minimum staffing levels.
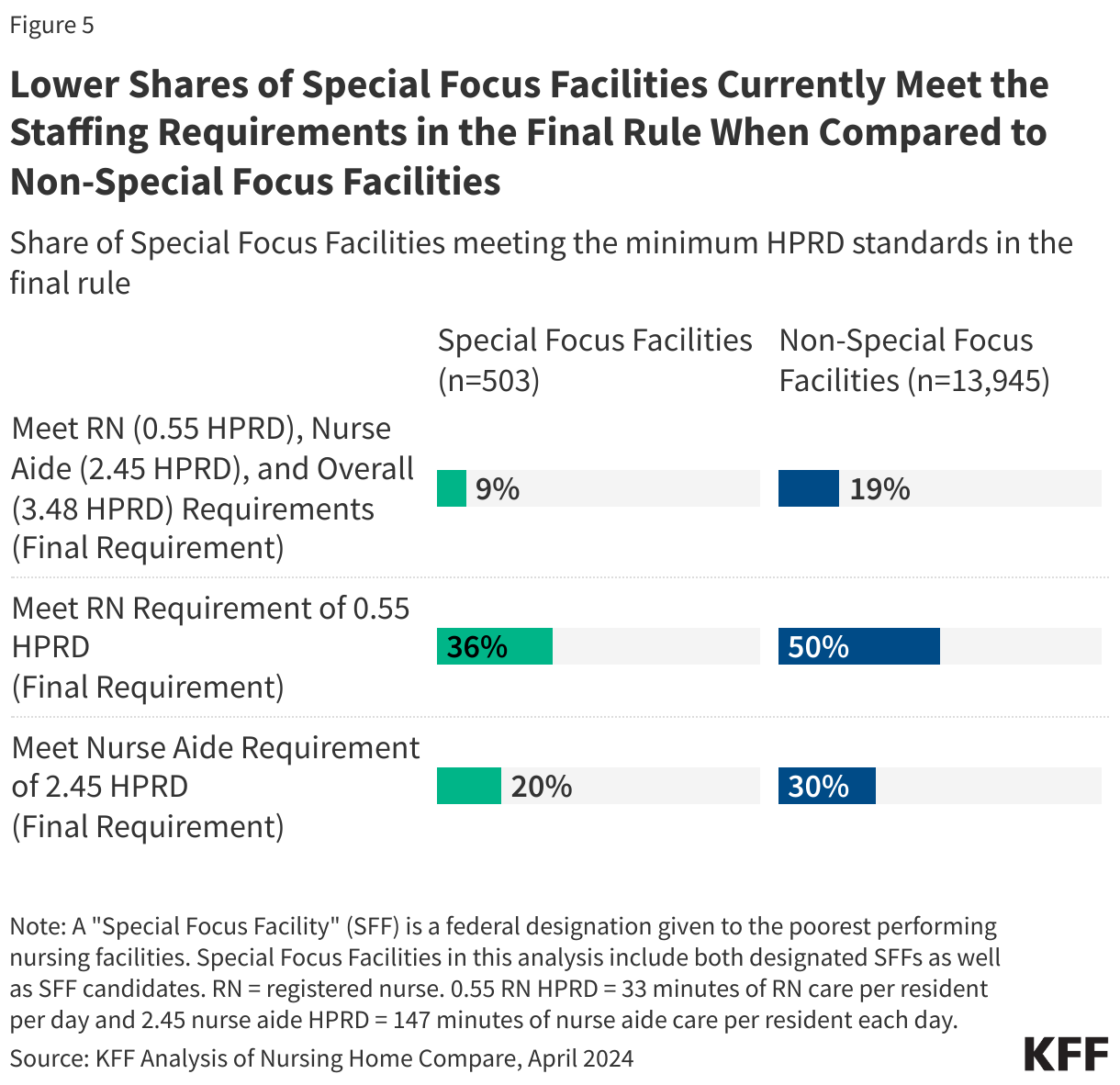
Among the 503 Special Focus Facilities (SFF) & SFF candidates (facilities with a history of serious quality issues), only 9% have staffing levels that would meet the requirements in the final rule (Figure 5). CMS established the Special Focus Facility program in 1998 to improve care in the poorest performing nursing homes that have a history of serious quality issues. To avoid poor-quality facilities receiving exemptions from the staffing minimums, the final rule states that Special Focus Facilities are not eligible for an exemption to the provisions in the final staffing rule. These facilities are described as having a “yo-yo” compliance history, meaning that even when these facilities correct problems identified on one inspection, they often have significant problems by the time the next inspection occurs. These repeated quality issues arise because the facilities rarely address underlying systemic problems, which can lead to cycles of serious deficiencies and pose risks to residents’ health and safety. For SFFs, state agencies conduct a full, onsite inspection of all health and safety requirements every six months, and recommend progressive enforcement (e.g., civil money penalty, denial of federal funds, etc.) until the facility either (1) graduates from the SFF program; or (2) is terminated from the Medicare and/or Medicaid program(s). Due to resource constraints, the SFF designation is limited to a certain number of nursing facilities. States also have the option to designate facilities as SFF candidates, with a maximum of 30 SFF candidates per state. Once an SFF graduates or is terminated, the state selects a new SFF from the list of candidates.
CMS estimates that complying with the final rule will cost $43 billion in the 10 years after the final rule takes effect. Since the rule was released, prominent labor unions have applauded its release while the nursing home industry has issued statements criticizing its finalization and other groups have expressed concerns about the high costs the rule may create for nursing homes and states. Labor unions commended the elements of the rule, noting that it was long overdue and would go a long way in protecting the residents and staff that live and work in nursing facilities. From the industry, there has been criticism related to funding of the rule and workforce shortages. The cost of implementing the staffing requirements has been raised as a major concern by the nursing home industry, among others. For nursing facilities, hiring and retaining sufficient staff will increase their operational costs. Such costs are likely to be passed on to public and private payers for nursing facility services including residents and family members, Medicaid and Medicare. Medicaid is the single largest payer for nursing facilities so increased costs could have implications for state budgets as well as federal spending. The rule also requires state Medicaid agencies to report on the percent of Medicaid payments for institutional long-term services and supports (LTSS) that are spent on compensation for direct care workers and support staff, which is similar to a requirement for home-and-community based LTSS.
The final rule includes few details on enforcement, though CMS states that the existing survey, certification, and enforcement processes will be used to assess compliance. According to the final rule, CMS intends to publish more details on how compliance will be assessed in advance of each implementation date for different components of the rule. Forthcoming decisions about enforcement of the new staffing requirements and the ease with which nursing homes are able to receive hardship exemptions may impact the extent to which the final rule has its desired effect on the quality of care for nursing home residents. The need for nursing facility care is also likely to increase as the population continues to age, which may intensify these unintended consequences.
Methods
This analysis uses Nursing Home Compare as of April 2024 and reflects staffing levels from October 2023 to December 2023. Nursing Home Compare is a publicly available dataset that provides a snapshot of information on quality of care and key characteristics for approximately 14,900 Medicare and/or Medicaid-certified nursing facilities. This analysis drops about 3% of nursing facilities, including the facilities in Guam and Puerto Rico and nursing facilities for which there was not staffing data available for the fourth quarter of 2023, for a total analytic sample of 14,448 facilities. The number of facilities identified in this analysis as meeting/not meeting requirements may differ from CMS’ estimates due to different years and quarters of data used for estimates.
In Figure 3, the analysis uses the Office of Management and Budget’s (OMB) delineation of metropolitan and micropolitan statistical areas to designate rural and urban areas. Urban and rural facilities have different timelines to come into compliance with the rule, but the analysis reflects compliance rates if the HPRD requirements were in effect now for all facilities.
Due to the limitations of publicly available data, this analysis does not look at facilities that meet the requirement to have an RN on staff 24 hours a day, seven days a week (24/7). Nursing home staffing data is calculated from the Payroll Based Journal (PBJ), which includes data on the total number of RN hours worked per day at a facility, but no data on the timing of shifts. This limits our understanding of whether shifts were worked simultaneously by multiple employees (possibly not fulfilling the 24-hour requirement) or whether those hours were spread out over a 24-hour period (fulfilling the 24-hour requirement). CMS estimates that close to 80% of nursing facilities would already meet the RN 24/7 requirement. It is unclear how the agency estimated whether nursing facilities had RNs on staff 24/7 or what data they used to do so.