
How has the ACA Medicaid Expansion Affected Providers Serving the Homeless Population: Analysis of Coverage, Revenues, and Costs
The Affordable Care Act (ACA) Medicaid expansion to adults closed a longstanding gap in eligibility in the 32 states, including DC, that have adopted it to date, providing a new coverage option for millions of uninsured adults. In Medicaid expansion states, many people experiencing homelessness are newly eligible for coverage since this population includes many single adults who were excluded from Medicaid prior to the expansion. Coverage is particularly important for this population given that they have poor health and intensive health care and social service needs. To further understand how the first full year of Medicaid expansion has affected patients who are homeless and the providers who care for them, this analysis uses data from the Uniform Data System (UDS) for health centers1 to examine changes in insurance coverage, revenues, and costs among Health Care for the Homeless (HCH) projects serving the homeless population. Key findings include the following:
There have been significant coverage gains among patients at HCH projects since implementation of the ACA in 2014, with much larger gains among patients at HCH projects in states that expanded Medicaid compared to non-expansion states. In Medicaid expansion states, the health coverage rate for patients at HCH projects increased by 22 percentage points from 45% in 2012 to 67% during 2014, while the coverage rate increased by only 4 percentage points from 26% to 30% in non-expansion states (Figure 1). HCH projects experienced larger coverage gains among patients compared to other health centers, but their coverage rates remain lower than other health centers in 2014.
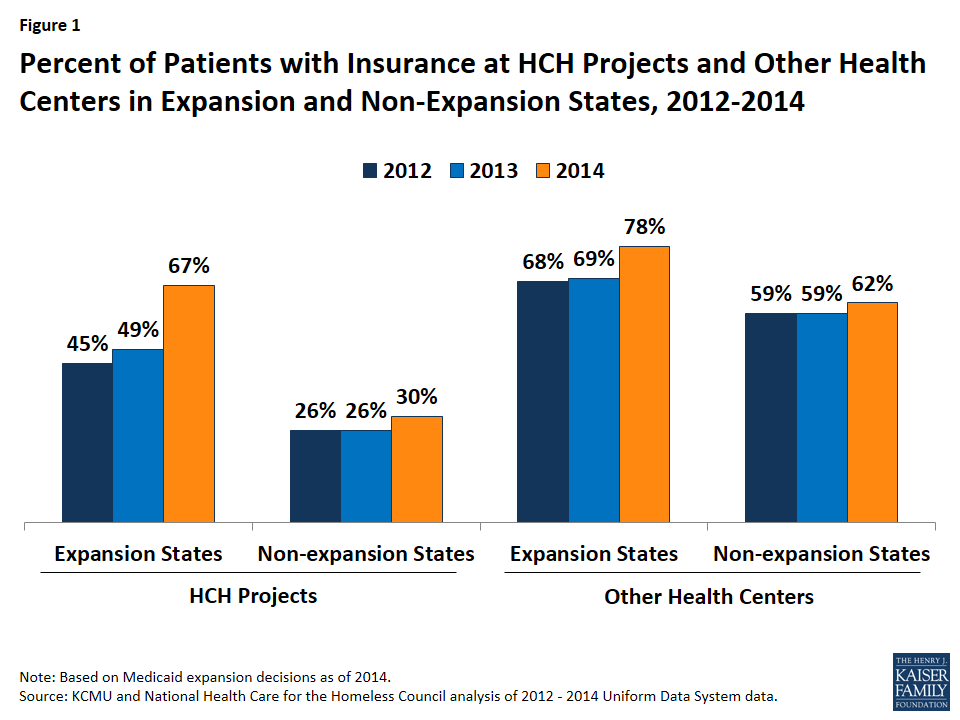
Figure 1: Percent of Patients with Insurance at HCH Projects and Other Health Centers in Expansion and Non-Expansion States, 2012-2014
HCH Projects in expansion states also had larger gains in revenue and smaller increases in costs compared to those in non-expansion states (Figure 2). In expansion states, total revenues for HCH projects in 2014 were 7% higher than total revenues in 2013. In contrast, revenues for HCH projects in non-expansion states increased marginally, rising only 2%. Conversely, total costs for HCH projects in non-expansion states were 9% higher in 2014 than 2013, compared to 3% higher for those in expansion states. HCH projects had smaller revenue and cost increases compared to other health centers in both expansion and non-expansion states.
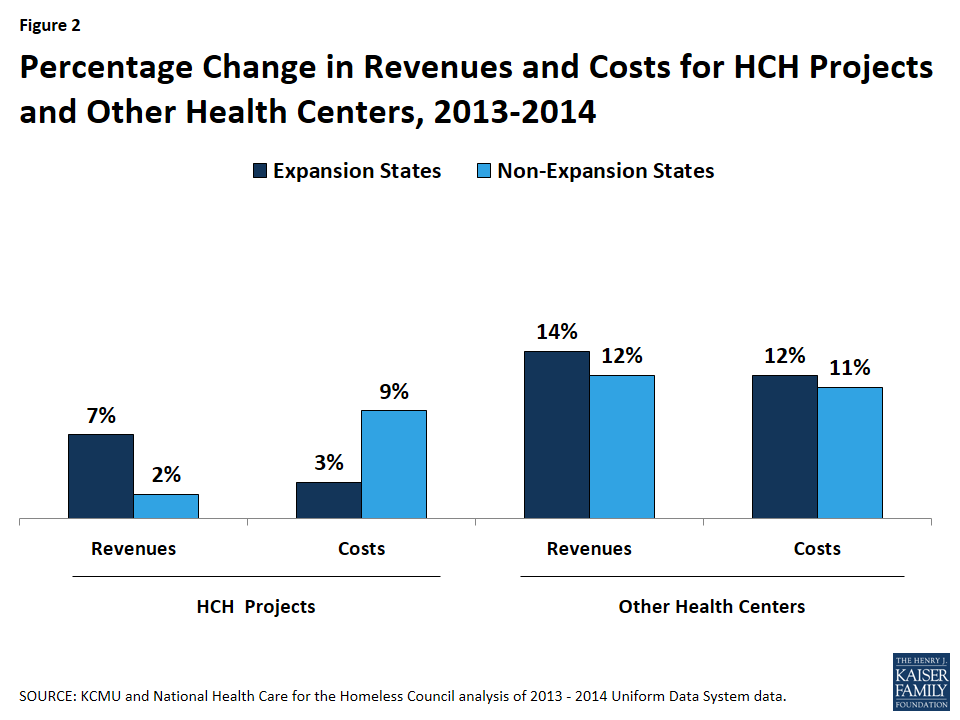
Figure 2: Percentage Change in Revenues and Costs for HCH Projects and Other Health Centers, 2013-2014
For HCH projects in expansion states, third-party payments increased as a share of total revenue due to coverage gains among patients. With this increase, only about half (49%) of total revenue for HCH projects in expansion states came from grants in 2014. In contrast, HCH projects in non-expansion states experienced little change in third-party payments as a share of revenue and remain heavily reliant on grant funding (Figure 3).
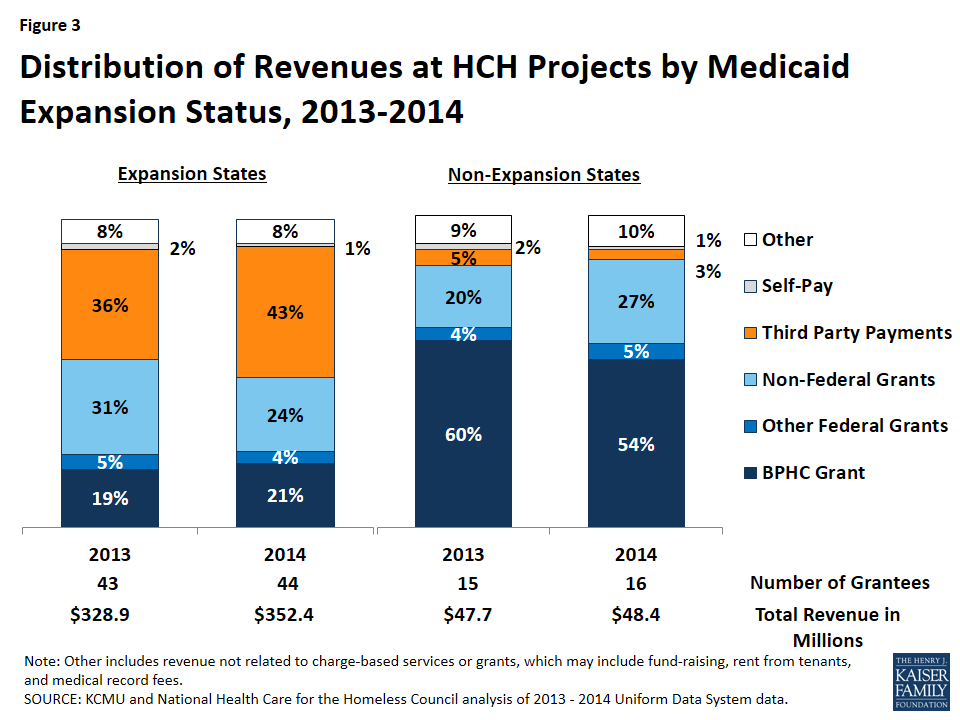
Figure 3: Distribution of Revenues at HCH Projects by Medicaid Expansion Status, 2013-2014
The distribution of costs remained fairly stable among HCH projects in both expansion and non-expansion states. Among HCH projects in expansion and non-expansion states, medical care (medical care personnel, laboratory and x-ray, and other direct medical costs) accounted for about half of costs, clinical care (dental, mental health, substance abuse, pharmacy, vision and other services) made up about 30% of costs, and the remainder of costs were for enabling services (case management, outreach, transportation, translation and interpretation, education, eligibility assistance and other support).
In sum, HCH projects in expansion states have had larger coverage gains among patients as well as greater revenue gains and smaller increases in costs compared to those in non-expansion states, with third-party payments increasing as a share of revenue due to coverage gains among patients. Together, the coverage gains and revenue increases may facilitate broader access to services among patients and greater stability for HCH projects in expansion states. Gains in third-party revenue may also support strategic and operational improvements. Yet even with gains in third-party revenue, grant funding still remains important, particularly for services such as case management and outreach that are not reimbursed by Medicaid. HCH projects may also face new administrative challenges associated with serving an increasing share of patients with coverage. In contrast, HCH projects in non-expansion states continue to serve a largely uninsured population, experienced increased costs but little increase in revenue, and rely almost exclusively on grant funding.
